Perineurial (Fascicular) Neurorrhaphy: A Comprehensive Microsurgical Guide

Key Takeaway
Perineurial (fascicular) neurorrhaphy is a precise microsurgical technique utilized to repair peripheral nerve transections. By aligning and coapting individual fascicles or fascicular groups using 9-0 or 10-0 sutures under high magnification, surgeons optimize motor and sensory axonal regeneration. This approach is particularly indicated for mixed nerves with distinct topographical anatomy, minimizing axonal misdirection and maximizing functional recovery compared to standard epineurial repair.
Comprehensive Introduction and Patho-Epidemiology
Peripheral nerve injuries represent one of the most profound and technically demanding reconstructive challenges encountered by orthopedic, plastic, and hand surgeons. The ultimate physiological goal of any nerve repair is the restoration of maximal motor and sensory function through the precise, topographical realignment of axonal pathways. While standard epineurial repair remains the historical and practical workhorse for many acute nerve lacerations, perineurial (fascicular) neurorrhaphy offers a highly targeted, conceptually superior microsurgical approach. By directly coapting individual fascicles or grouped fascicles (interfascicular repair), the surgeon actively minimizes axonal misdirection—a critical, often outcome-defining factor when reconstructing mixed motor and sensory nerves.
To fully appreciate the necessity of perineurial repair, one must understand the patho-epidemiology of peripheral nerve trauma. Epidemiological data suggests that peripheral nerve injuries occur in approximately 2% to 3% of all major extremity traumas, with a significant predilection for young, active individuals. The consequences of these injuries are devastating, frequently leading to lifelong disability, chronic neuropathic pain, and profound socioeconomic burden. The injury initiates a complex cellular cascade. Distal to the site of transection, the nerve undergoes Wallerian degeneration, a process characterized by axonal disintegration, myelin clearance by macrophages, and the subsequent proliferation of Schwann cells. These Schwann cells align to form the bands of Büngner, which serve as the vital biological conduits guiding regenerating axonal growth cones from the proximal stump.
However, this regenerative potential is strictly time-dependent and highly susceptible to architectural mismatch. Regenerating axons sprout at a rate of approximately 1 millimeter per day, but if a motor axon is misdirected down a sensory endoneurial tube, it will never reinnervate its target muscle, rendering that specific regeneration utterly futile. Furthermore, motor endplates undergo irreversible degradation if not reinnervated within 12 to 18 months. Therefore, the surgical intervention must not only be timely but must also ensure the highest possible fidelity of axonal alignment. Perineurial neurorrhaphy directly addresses this requirement by bypassing the macroscopic epineurial sheath and forcing alignment at the functional, fascicular level.
The mastery of this technique demands an advanced degree of microsurgical proficiency. The surgeon must possess an intimate understanding of intraneural topography, which shifts and arborizes continuously along the length of the extremity. Furthermore, the technical execution requires absolute mastery of the operating microscope, the ability to mitigate physiological tremors, and the finesse to manipulate delicate 9-0, 10-0, or even 11-0 monofilament sutures with atraumatic precision. The margin for error is microscopic; a poorly placed perineurial suture can induce localized ischemia, incite a robust foreign-body inflammatory response, and ultimately block the advancing growth cone, leading to a neuroma-in-continuity and surgical failure.
The Cellular Response to Injury and Repair
Following transection, the proximal stump undergoes retrograde degeneration to the first node of Ranvier, while the neuronal cell body in the anterior horn or dorsal root ganglion undergoes chromatolysis, shifting its metabolic machinery from neurotransmitter production to structural protein synthesis. The success of perineurial neurorrhaphy relies on capturing these newly synthesized proteins (tubulin, actin) as they form the axonal growth cone. By suturing the perineurium, the surgeon re-establishes the crucial blood-nerve barrier at the fascicular level, minimizing the influx of inflammatory cytokines and fibroblasts from the extraneural environment. This isolated microenvironment is highly conducive to the neurotrophic factors (such as Nerve Growth Factor and Brain-Derived Neurotrophic Factor) secreted by the distal Schwann cells.
Historical Context and Evolution
The evolution of nerve repair techniques has been a subject of intense academic debate for decades. Historically, epineurial repair was the sole method utilized, largely due to the lack of adequate magnification. With the advent of the operating microscope in the mid-20th century, pioneers like Hanno Millesi and Sydney Sunderland began advocating for interfascicular dissection and perineurial repair, positing that reducing tension and aligning fascicles would yield superior outcomes. While subsequent meta-analyses have shown that routine fascicular repair for all nerve injuries does not universally outperform epineurial repair, it is now widely accepted that for specific indications—namely distal mixed nerves with distinct topography—perineurial neurorrhaphy is the gold standard for optimizing functional recovery.
Detailed Surgical Anatomy and Biomechanics
A thorough, almost microscopic comprehension of peripheral nerve anatomy and its inherent biomechanical properties is non-negotiable for any surgeon attempting fascicular repair. The peripheral nerve is not merely a biological wire; it is a highly complex, dynamic organ composed of specialized neural elements, hierarchical connective tissue sheaths, and a dedicated, fragile vascular network.
Hierarchical Microanatomy of the Peripheral Nerve
The connective tissue framework of the peripheral nerve serves to protect the delicate axons from mechanical stress while allowing for physiological excursion during joint movement.
* Mesoneurium: This is the outermost layer, consisting of loose areolar tissue that suspends the nerve within its anatomical bed. It is highly vascularized and allows for the longitudinal gliding of the nerve. Preservation of the mesoneurium is critical to prevent postoperative tethering and ischemic contracture of the nerve.
* Epineurium: This layer is anatomically divided into two distinct components. The epifascicular epineurium is the robust outer sheath that provides the nerve with its primary structural integrity and resistance to compressive forces. The interfascicular epineurium is the loose connective tissue packing that surrounds and cushions the individual fascicles within the main nerve trunk.
* Perineurium: This is the critical layer engaged during fascicular neurorrhaphy. It is a dense, lamellated connective tissue sheath enclosing individual fascicles. Biomechanically, it provides the primary tensile strength of the nerve. Physiologically, its inner layers feature specialized tight junctions that form the blood-nerve barrier, maintaining the privileged endoneurial microenvironment required for axonal conduction and regeneration.
* Endoneurium: The innermost, delicate collagenous matrix surrounding individual axons and their associated Schwann cells. It contains the capillary networks of the intrinsic vascular system and the endoneurial fluid.
Intraneural Topography and Plexus Formation
The arrangement of fascicles within a nerve—its topography—is not static. As a nerve travels proximally to distally, the fascicles repeatedly divide, anastomose, and intermingle, forming complex intraneural plexuses. In the proximal segments of a limb (e.g., the proximal sciatic or median nerve in the arm), the nerve is typically polyfascicular with highly intermingled motor and sensory fibers, making accurate fascicular mapping nearly impossible. Conversely, in the distal segments (e.g., the median nerve at the wrist), the nerve becomes oligofascicular, and the fascicles segregate into distinct, functional groups (e.g., the recurrent motor branch fascicles separate from the digital sensory fascicles). It is in these distal, segregated regions that perineurial neurorrhaphy is most efficacious.
Vascular Anatomy: The Vasa Nervorum
The blood supply to the peripheral nerve is highly specialized and highly vulnerable to surgical trauma. It is divided into an extrinsic and an intrinsic system. The extrinsic system consists of segmental feeding vessels that enter the mesoneurium and form a longitudinal plexus on the epifascicular epineurium. These vessels penetrate the epineurium to join the intrinsic system, which consists of longitudinal microvessels running within the interfascicular epineurium, perineurium, and endoneurium. During perineurial repair, extensive interfascicular dissection can disrupt this intrinsic network. Therefore, dissection must be meticulous and limited only to the extent necessary to identify and coapt the fascicles, thereby preventing iatrogenic intraneural ischemia.
Biomechanics of Nerve Repair and the Tension Paradigm
Tension is the absolute enemy of nerve regeneration and the primary cause of neurorrhaphy failure. The peripheral nerve exhibits viscoelastic properties; it can stretch to accommodate normal joint motion. However, excessive tension across a repair site has catastrophic biological consequences. Lundborg's landmark studies demonstrated that an elongation of merely 8% reduces intraneural venular flow, while an elongation of 15% causes complete cessation of all intraneural microcirculation.
When a perineurial repair is subjected to tension, the localized ischemia stimulates aggressive fibroblast proliferation. These fibroblasts lay down dense collagenous scar tissue at the coaptation site, effectively forming an impenetrable physical barrier to the advancing axonal growth cones. The perineurium, while robust enough to hold a 10-0 suture, will inevitably tear or undergo pressure necrosis if subjected to undue longitudinal stress. Therefore, perineurial neurorrhaphy must only be performed when a completely tension-free coaptation can be achieved in the neutral physiological position. If any tension is present, the surgeon must immediately abandon primary repair and bridge the defect with interfascicular nerve autografts.
Exhaustive Indications and Contraindications
The decision to perform a perineurial (fascicular) neurorrhaphy versus a standard epineurial repair or a nerve graft requires nuanced clinical judgment. The surgeon must carefully weigh the benefits of precise topographical alignment against the risks of increased surgical trauma, prolonged operative time, and the introduction of additional foreign body material into the intraneural space.
Indications for Perineurial Neurorrhaphy
The primary indication for perineurial repair is the presence of a mixed motor and sensory nerve injury in a topographical region where the functional fascicular groups are distinctly segregated and identifiable. The classic example is the median nerve at the level of the distal forearm or carpal tunnel. Here, the motor fascicles destined for the thenar musculature are localized anteroradially, while the sensory fascicles to the digits are located more ulnarly. Precise grouped fascicular repair ensures that the critical motor axons are directed specifically into the recurrent motor branch endoneurial tubes.
Partial nerve transections represent another absolute indication. In scenarios where a sharp laceration has severed only a portion of the nerve trunk (e.g., a glass laceration dividing only the ulnar sensory fascicles of the ulnar nerve while sparing the deep motor branch), an epineurial repair is impossible without transecting the intact, functioning fascicles. In such cases, the surgeon must perform an interfascicular dissection and a targeted perineurial repair of the injured fascicles only, carefully protecting the uninjured components.
Secondary nerve reconstructions following neuroma excision also frequently necessitate fascicular techniques. When a neuroma-in-continuity is resected, the resulting proximal and distal stumps often exhibit splayed, disorganized fascicular architecture. Epineurial repair is often mechanically impossible or biologically unsound in this setting. The surgeon must dissect the individual fascicular groups back to healthy tissue and coapt them, often utilizing short intercalary nerve grafts.
Contraindications to Perineurial Neurorrhaphy
Conversely, there are strict contraindications where perineurial repair is either biologically detrimental or technically futile. Severe crush, avulsion, or blast injuries result in a wide zone of trauma where the delicate fascicular architecture is destroyed over a long segment. In these cases, attempting to identify and suture individual fascicles within the zone of injury is impossible and will only result in securing necrotic tissue. These injuries require aggressive resection back to healthy tissue, inevitably creating a gap that mandates nerve grafting.
Significant gaps that preclude a tension-free repair are an absolute contraindication. As previously discussed, tension leads to ischemia and failure. If the nerve ends cannot be approximated with an 8-0 epineurial suture without tension, fascicular repair must not be attempted. The surgeon must transition to an interfascicular nerve grafting technique.
Finally, oligofascicular nerves without distinct topography (purely motor or purely sensory nerves, or highly intermingled proximal mixed nerves) do not benefit from the extensive dissection required for perineurial repair. In a purely sensory nerve like the sural nerve, any regenerating axon will reach a sensory target; therefore, the precise alignment of individual fascicles does not significantly alter the functional outcome compared to a well-performed epineurial repair. In these scenarios, the iatrogenic trauma of interfascicular dissection outweighs the theoretical benefits.
Summary Table of Indications and Contraindications
| Clinical Scenario | Recommendation | Rationale / Pathophysiological Basis |
|---|---|---|
| Distal Mixed Nerves (e.g., Median at wrist) | Strongly Indicated | Distinct topographical segregation of motor and sensory fascicles allows for precise anatomical matching, preventing axonal misdirection. |
| Partial Nerve Transections | Strongly Indicated | Allows repair of the severed fascicles without iatrogenic transection or compromise of the intact, functioning fascicular groups. |
| Purely Motor or Sensory Nerves | Contraindicated | Axonal misdirection is functionally irrelevant (all targets are the same modality). Epineurial repair is faster and less traumatic to the vasa nervorum. |
| Proximal Mixed Nerves (e.g., Sciatic at thigh) | Relative Contraindication | Highly polyfascicular and intermingled topography makes accurate mapping impossible. High risk of iatrogenic injury with minimal functional benefit. |
| Severe Crush / Avulsion Injuries | Contraindicated | Destruction of fascicular architecture over a wide zone. Requires extensive resection and interfascicular nerve grafting. |
| Repairs Under Tension | Absolute Contraindication | Tension induces intraneural ischemia, fibroblast proliferation, and neuroma formation. Mandates nerve grafting regardless of topography. |
Pre-Operative Planning, Templating, and Patient Positioning
The success of a complex microsurgical nerve reconstruction begins long before the first incision is made. Meticulous preoperative planning, advanced imaging, and optimal intraoperative setup are critical components that dictate the fluidity and ultimate success of the procedure.
Clinical Evaluation and Advanced Imaging
The preoperative evaluation must establish a precise baseline of motor and sensory deficits. Serial clinical examinations, documenting advancing Tinel's signs and specific muscle grading (Medical Research Council scale), are essential. Electromyography (EMG) and Nerve Conduction Studies (NCS) are typically obtained at 3 to 4 weeks post-injury to confirm the diagnosis of axonotmesis or neurotmesis and to establish a baseline for future comparison.
In recent years, high-resolution ultrasound (HRUS) and Magnetic Resonance Neurography (MRN) have revolutionized the preoperative templating of nerve injuries. HRUS, utilizing high-frequency probes (15-22 MHz), allows the surgeon to visualize the fascicular architecture non-invasively, identify the exact location of a neuroma, and accurately measure the gap between retracted nerve stumps. This information is invaluable for preoperative consent, allowing the surgeon to accurately counsel the patient on the likelihood of requiring autologous nerve grafts (e.g., sural nerve harvest) and the expected prolonged recovery timeline.
Equipment and Microsurgical Instrumentation
Perineurial neurorrhaphy cannot be performed with standard macroscopic instruments. The operating theater must be equipped with a high-quality operating microscope featuring foot-pedal control for zoom, focus, and X-Y axis movement. Magnification ranges from 10x for initial preparation to 40x for the actual perineurial coaptation are required.
The instrumentation must be specialized and meticulously maintained. The core tray includes jeweler’s forceps (straight and curved with ultra-fine tips), Castroviejo or Barraquer needle holders, microscissors (both straight for nerve trimming and curved adventitial scissors for epineurial dissection), and a micro-nerve hook. Suture selection is paramount; the surgeon typically utilizes 9-0 or 10-0 non-absorbable monofilament (e.g., Nylon or Polypropylene) armed with a spatulated or taper-point micro-needle. A colored silicone background material (usually blue or green) is essential; it is placed behind the nerve to enhance visual contrast, reduce glare from the microscope light, and prevent the delicate micro-sutures from adhering to the underlying moist soft tissues.
Patient Positioning and Tourniquet Management
Patient positioning must prioritize both surgical exposure and surgeon ergonomics. Microsurgery is physically demanding; the surgeon must be seated comfortably with forearms fully supported to eliminate physiological tremor. The patient is positioned supine or prone depending on the specific nerve involved, and the extremity is prepped and draped widely to allow for extensile exposures. If nerve grafting is a possibility, the ipsilateral or contralateral lower extremity must also be prepped for sural nerve harvest.
A pneumatic tourniquet is routinely applied to provide an absolutely bloodless surgical field. This is not merely a convenience; it is a strict requirement for identifying the microscopic vascular landmarks on the epineurium that guide rotational alignment. However, tourniquet management requires extreme vigilance. Strict adherence to tourniquet time limits (typically 90 to 120 minutes depending on the limb and patient comorbidities) is vital. Prolonged ischemia can compound the existing nerve injury, delay Wallerian degeneration, and severely impair subsequent axonal regeneration. The surgeon must plan the procedure to deflate the tourniquet, achieve meticulous hemostasis, and allow for reactive hyperemia prior to the final micro-suturing phase.
Step-by-Step Surgical Approach and Fixation Technique
The execution of a perineurial neurorrhaphy is a highly choreographed sequence of microsurgical maneuvers. Each step must be performed with atraumatic precision to preserve the delicate intraneural microenvironment.
Step 1: Exposure and Preparation of the Nerve Ends
The surgical approach begins with an extensile longitudinal incision, incorporating the traumatic wound if present, but extending well into healthy tissue proximally and distally. The golden rule of peripheral nerve surgery is to always identify the normal, uninjured nerve in virgin tissue planes first. Once the healthy nerve is identified, it is carefully traced toward the zone of injury. This approach minimizes the risk of iatrogenic injury within the distorted scar tissue of the traumatic bed.
Once the injured segment is isolated, the traumatized ends of the nerve must be resected. Using a fresh scalpel blade (No. 11 or 15 on a sterile wooden tongue depressor) or specialized diamond-edged nerve-cutting scissors, the surgeon sharply "bread-loafs" the proximal and distal stumps. The resection continues sequentially until healthy, "pouting" fasciculi are visualized. The fascicles should herniate slightly from the epineurial sheath, indicating normal intraneural pressure and the absence of fibrotic tethering. Following tourniquet deflation, the presence of punctate bleeding from the vasa nervorum on the cut ends confirms adequate resection to viable, well-vascularized tissue.
Step 2: Topographical Alignment and Fascicular Mapping
Placing the nerve ends in proper rotational alignment is arguably the most critical step in preventing axonal mismatch. The surgeon must utilize all available anatomical clues.
* Vascular Landmarks: The longitudinal epineurial blood vessels often follow a distinct, slightly spiraling course. Aligning these vessels provides the primary rotational orientation.
* Fascicular Size and Shape: The cross-sectional topography is carefully examined under high magnification. Motor fascicles often differ in size, shape, and grouping from sensory fascicles.
💡 Clinical Pearl: Fascicular Mapping
It is highly highly recommended to diagram the arrangement of the fascicular groups on sterile paper (often fashioned from the inner glove wrapper or suture packaging). This "map" serves as a crucial visual reference during the complex coaptation phase, ensuring that the surgeon does not lose orientation as the repair progresses.
Step 3: Transfixation of Nerve Ends
To maintain the painstakingly achieved rotational alignment and to relieve tension during the delicate fascicular suturing, the nerve ends are transfixed. The surgeon passes straight stainless steel needles (e.g., 25-gauge hypodermic needles) through the epineurium of the proximal and distal stumps, pinning them to the adjacent soft tissues or underlying muscle bed. This stabilizes the nerve stumps, preventing them from retracting, rotating, or drifting out of the microscopic field during the repair.
Step 4: Epineurial Dissection
With the nerve stabilized, the interfascicular dissection begins. The surgeon incises the epifascicular epineurium longitudinally, both proximally and distally, for a distance of 5 to 10 mm from the cut ends. Using micro-forceps and adventitial scissors, the epineurium is carefully peeled back to expose the underlying fasciculi. Excision of a small cuff of this redundant epineurium is often necessary; if left in place, it can interpose between the fascicles during repair, acting as a physical barrier to regeneration.
Step 5: Fascicular Coaptation
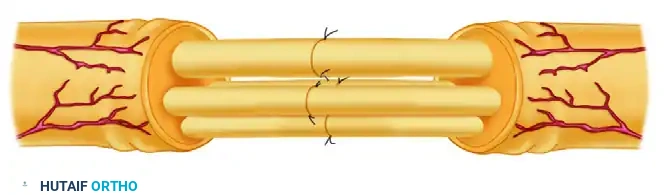
The core of the procedure is the approximation of the corresponding fasciculi. Where the nerve is composed of multiple small fasciculi (polyfascicular), it is biologically sound and practically necessary to approximate several adjacent fasciculi as a single functional unit (group fascicular repair). Suturing every single micro-fascicle individually introduces excessive foreign body material (suture), which incites a robust inflammatory response and subsequent fibrosis.
The surgeon begins by passing the 10-0 nylon suture through the perineurium of the proximal fascicle. The micro-needle should enter the perineurium approximately 1 to 2 mm from the cut edge. The bite must engage only the tough, lamellated perineurium, strictly avoiding the delicate endoneurial contents and the axons within.

The suture is carefully drawn through, ensuring it does not tangle or catch on adjacent tissues. Next, the surgeon passes the needle through the corresponding distal fascicle. This pass is made from inside to outside, ensuring that the needle exits the distal perineurium at the exact corresponding anatomical point, thereby maintaining the precise topographical alignment.
The suture is then tied using a standard microsurgical instrument tie. The critical factor here is tension. The knot must be tied with just enough tension to approximate the fascicular ends without causing them to buckle, overlap, or gap. A perfect coaptation resembles two pipes meeting flush end-to-end. Typically, two to three interrupted 9-0 or 10-0 nylon sutures are required per fascicle or fascicular group to achieve a secure, gap-free coaptation.
Step 6: Epineurial Management and Hemostasis
Once all fasciculi have been matched and approximated, the surgeon must decide how to manage the reflected epineurium. If the fascicular neurorrhaphy is highly secure and there is absolutely no tension on the repair, it is often preferable to omit the epineurial closure entirely. Leaving the epineurium open decreases the total amount of foreign body material and significantly reduces the risk of constrictive epineurial fibrosis, which can choke the regenerating axons in a "compartment syndrome" like mechanism.
Before closing the surgical wound, absolute hemostasis must be confirmed. The tourniquet is deflated, and the repair site is observed for several minutes. Hematoma formation at the repair site is disastrous; the degrading blood products incite severe scarring and inevitably lead to failure of nerve regeneration. Bipolar electrocautery must be used with extreme caution, utilizing fine tips and low power settings, and kept strictly away from the nerve itself. The soft tissues are then closed in layers, ensuring that the nerve repair is covered by a healthy, well-vascularized soft tissue bed (e.g., a transposed muscle belly). The repair must never be left directly under the skin incision to prevent tethering and painful cutaneous neuromas.
Complications, Incidence Rates, and Salvage Management
Despite flawless microsurgical technique, perineurial neurorrhaphy carries inherent risks and potential complications. The biological variables of nerve regeneration are vast, and the surgeon must be prepared to identify and manage failures aggressively.
Common Complications and Pathophysiology
The most devastating complication is failure of regeneration due to tension at the repair site. As emphasized repeatedly, tension induces ischemia and dense scar formation. This typically presents clinically as a stalled Tinel's sign (failing to progress distally at the expected rate of 1mm/day) and an absence of motor or sensory recovery on serial examinations and EMG.
Fascicular mismatch is another significant complication, particularly in mixed nerves. If rotational alignment is incorrect, motor axons will regenerate down sensory endoneurial tubes. This results in an absolute failure of motor recovery, as the motor axons cannot form functional synapses with sensory receptors. Clinically, the patient may regain some protective sensation but will exhibit profound, irreversible muscle atrophy and paralysis.
Neuroma-in-continuity occurs when regenerating axons escape the repair site due to micro-gapping, poor coaptation, or excessive scar tissue blocking the endoneurial tubes. These escaping axons form a disorganized, highly sensitive mass of neural tissue. Patients present with severe, localized neuropathic pain, an exquisitely sensitive localized Tinel's sign, and halted distal regeneration.
Summary Table of Complications and Management
| Complication | Estimated Incidence | Pathophysiology | Salvage Management / Revision Strategy |
|---|---|---|---|
| Tension Failure / Scarring | 5% - 15% | Ischemia leading to fibroblast proliferation and mechanical block of axonal growth cones. | Surgical re-exploration, resection of the fibrotic segment, and interfascicular nerve autografting. |
| Fascicular Mismatch | 10% - 20% (in proximal nerves) | Incorrect rotational alignment causing motor axons to enter sensory pathways. | Late presentation often precludes revision nerve surgery. Requires definitive tendon transfers or free functioning muscle transfers. |
| Neuroma-in-Continuity | 5% - 10% | Axonal escape at the coaptation site due to gapping or physical blockage by suture granuloma. | Exploration and intraoperative nerve conduction testing. If no conduction across the neuroma, resect and graft. If partial conduction, perform internal neurolysis. |
| Suture Granuloma | < 5% | Robust foreign body reaction to excessive or excessively large suture material (e.g., using 8-0 instead of 10-0). | Excision of the granuloma; may require revision of the neurorrhaphy if the nerve architecture is heavily involved. |
| Infection | < 2% | Bacterial colonization of the surgical site, exacerbated by hematoma formation. | Aggressive surgical debridement, targeted intravenous antibiotics. The nerve repair is at extremely high risk of failure. |
Salvage Strategies: Beyond Primary Repair
When a perineurial neurorrhaphy fails, the window for successful revision nerve surgery is narrow due to the progressive, irreversible degradation of the distal motor endplates. If a failure is identified early (e.g., 4 to 6 months post-op with no advancing Tinel's and flat EMG), surgical re-exploration is indicated. The failed repair is resected back to healthy fascicles, and the resulting gap is bridged with nerve autografts (typically the sural nerve).
If the failure is identified late (>12-18 months), the motor endplates are considered non-viable, and revision nerve surgery to the original target muscle is futile. In these scenarios, the surgeon must pivot to salvage procedures. Nerve transfers (neurotization), utilizing expendable local motor donors transferred directly into the distal motor nerve close to the target muscle, can sometimes salvage function if performed within the viable time window. However, the most reliable definitive salvage for late failures remains tendon transfers, where a functioning, synergistic muscle-tendon unit is re-routed to substitute for the paralyzed muscle, completely bypassing the failed neurological pathway.
Phased Post-Operative Rehabilitation Protocols
The surgical coaptation of the nerve is merely the first step in the reconstructive journey. The ultimate success of a perineurial neurorrhaphy relies heavily on a disciplined, highly structured, and phased postoperative rehabilitation program directed by a specialized hand or neuro-physiotherapist. The rehabilitation must balance the mechanical protection of the fragile repair with the physiological necessity of preventing tissue adhesions and promoting cortical re-education.
Phase 1: Immobilization and Protection (Weeks 0-3)
Immediately following surgery, the primary goal is the absolute protection of the micro-sutured fascicles. The extremity is immobilized in a custom-fabricated orthosis or
