Mastering Surgical Approaches to the Radial and Ulnar Nerves

Key Takeaway
Mastering the surgical approaches to the radial and ulnar nerves requires profound anatomical knowledge and meticulous technique. This guide provides an evidence-based, step-by-step framework for exposing the radial nerve from the axilla to the posterior interosseous branch, alongside comprehensive protocols for managing ulnar nerve pathology. Key principles include strategic mobilization, interfascicular grafting for defect closure, and precise clinical evaluation to optimize postoperative motor and sensory recovery in complex peripheral nerve injuries.
Comprehensive Introduction and Patho-Epidemiology
The surgical management of peripheral nerve injuries in the upper extremity remains one of the most technically demanding and intellectually rigorous domains within orthopedic surgery. Mastery of the surgical approaches to the radial and ulnar nerves is not merely an exercise in anatomical dissection; it requires a profound understanding of neural biomechanics, patho-epidemiology, and the biological limits of axonal regeneration. As the primary conduits for motor function and sensory feedback to the hand and forearm, the radial and ulnar nerves dictate the functional viability of the upper limb. An orthopedic surgeon's ability to safely expose, decompress, or reconstruct these structures directly correlates with the patient's ultimate functional outcome and quality of life.
The patho-epidemiology of radial nerve injuries is inextricably linked to the osteology of the humerus. The radial nerve is the most frequently injured major peripheral nerve secondary to long bone fractures, with an incidence ranging from 8% to 18% in closed humeral shaft fractures. The classic Holstein-Lewis fracture—a spiral fracture of the distal third of the humeral shaft—poses a uniquely high risk for nerve entrapment. In this scenario, the radial nerve is tethered as it pierces the lateral intermuscular septum, making it highly vulnerable to being drawn into the fracture site during reduction maneuvers. Furthermore, iatrogenic radial nerve palsies during open reduction and internal fixation (ORIF) of the humerus remain a significant clinical challenge, underscoring the necessity for meticulous surgical technique and precise anatomical knowledge.
Conversely, the patho-epidemiology of ulnar nerve pathology is predominantly characterized by compressive neuropathies and traction injuries at the elbow. Cubital tunnel syndrome represents the second most common compression neuropathy of the upper extremity, surpassed only by carpal tunnel syndrome. The ulnar nerve's superficial course posterior to the medial epicondyle renders it susceptible to direct trauma, while its dynamic excursion during elbow flexion predisposes it to traction and frictional neuritis. Tardy ulnar nerve palsy—a delayed manifestation of ulnar neuropathy—frequently develops decades after childhood lateral humeral condyle fractures that result in a progressive cubitus valgus deformity. Understanding these diverse mechanisms of injury is paramount for determining the appropriate surgical intervention, whether it be in situ decompression, anterior transposition, or complex nerve reconstruction.
The biological response to peripheral nerve injury dictates the critical timelines for surgical intervention. Following a severe axonotmetic or neurotmetic injury, Wallerian degeneration occurs distal to the lesion, characterized by the breakdown of axons and myelin sheaths. The subsequent regeneration of axons proceeds at a rate of approximately 1 millimeter per day, heavily dependent on the local microenvironment and the integrity of the endoneurial tubes. Prolonged denervation of skeletal muscle leads to irreversible motor endplate degradation and muscle atrophy, establishing a finite window of opportunity for successful nerve repair. Therefore, the surgeon must balance the benefits of expectant management against the ticking clock of irreversible muscle fibrosis, particularly in high proximal lesions where the distance to the target musculature is substantial.
Detailed Surgical Anatomy and Biomechanics
Radial Nerve Anatomy and Excursion
The radial nerve, representing the largest terminal branch of the posterior cord of the brachial plexus (C5-T1), possesses a complex and highly vulnerable anatomical course. Originating in the axilla, it descends posterior to the third part of the axillary artery and the proximal brachial artery. As it exits the axilla, it passes anterior to the tendons of the latissimus dorsi and teres major muscles before passing between the long and medial heads of the triceps brachii. Accompanied by the profunda brachii artery, the nerve enters the spiral groove (radial sulcus) of the humerus. It is a common misconception that the nerve lies directly on the periosteum throughout this groove; in reality, it is separated from the bone by the medial head of the triceps for a significant portion of its posterior course, only coming into direct contact with the bare periosteum at the lateral aspect of the humerus.
A critical anatomical landmark and zone of vulnerability occurs where the radial nerve pierces the lateral intermuscular septum to transition from the posterior to the anterior compartment of the arm. This typically occurs approximately 10 centimeters proximal to the lateral epicondyle. At this juncture, the nerve is relatively fixed and tethered, severely limiting its mobility. This tethering is the primary biomechanical reason the nerve is so susceptible to traction injuries during distal third humeral shaft fractures and iatrogenic damage during aggressive lateral retraction for plate application. Once in the anterior compartment, the nerve descends in the intermuscular interval between the brachialis medially and the brachioradialis laterally, supplying motor branches to the brachioradialis and the extensor carpi radialis longus (ECRL).
At the level of the radiocapitellar joint, the radial nerve bifurcates into its two terminal branches: the superficial sensory radial nerve and the deep motor branch, also known as the posterior interosseous nerve (PIN). The superficial branch continues distally deep to the brachioradialis, providing exclusively sensory innervation to the dorsal aspect of the hand. The PIN, however, dives deep, passing between the two heads of the supinator muscle. The proximal fibrous edge of the superficial head of the supinator, known as the Arcade of Frohse, is the most common site of PIN entrapment. The PIN provides critical motor innervation to the extensor compartment of the forearm, dictating finger and thumb extension.
Biomechanically, the radial nerve undergoes significant longitudinal excursion during upper extremity kinematics. During full elbow flexion and extension, the nerve must glide smoothly within its fascial beds to prevent traction neuritis. However, its fixed points at the axilla, the lateral intermuscular septum, and the Arcade of Frohse limit this excursion. When the humerus is fractured, the normal tension-banding effect of the intact bone is lost, and the dynamic forces of the surrounding musculature can exert abnormal sheer and traction forces on the nerve. Understanding these biomechanical constraints is essential when planning nerve transpositions or when mobilizing the nerve to close a gap during neurorrhaphy.
Ulnar Nerve Anatomy and Kinematics
The ulnar nerve originates from the medial cord of the brachial plexus, carrying fibers predominantly from the C8 and T1 nerve roots. In the proximal arm, it descends medial to the brachial artery and anterior to the triceps. At the mid-arm level, approximately 8 centimeters proximal to the medial epicondyle, the nerve pierces the medial intermuscular septum to enter the posterior compartment. Here, it passes beneath the Arcade of Struthers—a fascial band extending from the medial head of the triceps to the medial intermuscular septum—which can serve as a potential site of compression, particularly after anterior transposition procedures if not adequately released.
As the ulnar nerve approaches the elbow, it enters the cubital tunnel, a fibro-osseous canal bordered anteriorly by the medial epicondyle, laterally by the elbow joint capsule and the medial collateral ligament (MCL), and medially by the Osborne ligament (cubital tunnel retinaculum). The Osborne ligament spans from the medial epicondyle to the olecranon process and forms the roof of the tunnel. Distal to the cubital tunnel, the nerve passes between the humeral and ulnar heads of the flexor carpi ulnaris (FCU) muscle. The deep flexor-pronator aponeurosis in this region represents another critical zone of potential entrapment, requiring meticulous release during surgical decompression.
Distal to the elbow, the ulnar nerve travels through the anterior compartment of the forearm, deep to the FCU, providing motor branches to the FCU and the ulnar half of the flexor digitorum profundus (FDP). At the wrist, it enters Guyon's canal, a fibro-osseous tunnel bordered by the pisiform medially and the hook of the hamate laterally. Within or just distal to Guyon's canal, the nerve bifurcates into a superficial sensory branch and a deep motor branch. The deep motor branch is paramount for hand function, innervating the hypothenar muscles, all interossei, the two ulnar lumbricals, and the adductor pollicis.
The biomechanics of the ulnar nerve at the elbow are highly dynamic and clinically significant. During elbow flexion, the distance between the medial epicondyle and the olecranon increases, causing the Osborne ligament to become taut. This decreases the cross-sectional area of the cubital tunnel by up to 55%, significantly increasing intraneural pressure. Concurrently, elbow flexion causes the ulnar nerve to elongate by up to 4.7 millimeters and translate medially. In patients with a deficient Osborne ligament or congenital laxity, this medial translation can result in symptomatic subluxation or dislocation of the nerve over the medial epicondyle, leading to a friction-induced neuritis that necessitates surgical stabilization via transposition.
Exhaustive Indications and Contraindications
The decision to proceed with surgical exploration of the radial or ulnar nerve requires a nuanced evaluation of the mechanism of injury, the temporal progression of symptoms, and the physiological status of the patient. The overarching philosophy dictates that immediate exploration is reserved for scenarios where the nerve is highly likely to be anatomically transected or severely compressed by an irreducible bony fragment. In contrast, closed low-energy injuries are typically managed expectantly, allowing time for spontaneous recovery of neuropraxic or mild axonotmetic lesions. However, the surgeon must remain vigilant; failure to intervene within the critical biological window can condemn the patient to permanent functional deficits.
For the radial nerve, immediate surgical exploration is unequivocally indicated in the setting of open humeral shaft fractures with an associated radial nerve deficit. In these cases, the nerve is frequently lacerated, contused, or interposed within the fracture site, and primary repair or tagging for future grafting is essential. Penetrating trauma, such as sharp lacerations or high-velocity gunshot wounds traversing the nerve's anatomical path, also mandates early exploration. A critical and often debated indication is the "secondary palsy"—a radial nerve deficit that develops immediately after closed reduction of a humeral shaft fracture. This clinical presentation strongly suggests iatrogenic entrapment of the nerve within the fracture fragments, necessitating prompt surgical release to prevent irreversible crush injury.
Indications for ulnar nerve intervention frequently revolve around compressive neuropathies and delayed post-traumatic deformities. Tardy ulnar palsy, secondary to progressive cubitus valgus from a malunited pediatric lateral condyle fracture, is a classic indication for anterior transposition to relieve chronic traction. Severe cubital tunnel syndrome characterized by objective motor weakness (e.g., intrinsic muscle wasting, positive Froment's sign), profound sensory loss, or failure of conservative management (splinting, activity modification) warrants surgical decompression. Additionally, acute lacerations at the wrist or forearm, common in civilian glass injuries, require urgent microsurgical neurorrhaphy to restore the critical intrinsic motor function of the hand.
Contraindications to peripheral nerve surgery are generally relative and must be weighed against the catastrophic consequences of permanent paralysis. Severe soft tissue compromise, such as active infection or massive crush injuries with non-viable muscle beds, may preclude immediate nerve repair or transposition, necessitating delayed reconstruction once the soft tissue envelope has been optimized. Extreme medical instability that prohibits prolonged anesthesia is an absolute contraindication. Crucially, the temporal limit of delay serves as a biological contraindication; return of motor function is exceedingly rare when radial nerve neurorrhaphy is delayed beyond 15 months, or beyond 9 months for the posterior interosseous nerve, due to irreversible motor endplate fibrosis. In such scenarios, nerve exploration is futile, and the surgeon must pivot to salvage procedures such as tendon transfers.
| Clinical Scenario | Indication for Surgery | Timing of Intervention | Contraindications / Caveats |
|---|---|---|---|
| Open Humeral Fracture with Radial Palsy | Absolute | Immediate (< 24 hours) | Severe physiological instability; damage control orthopedics takes priority. |
| Secondary Radial Palsy post-Closed Reduction | Absolute | Urgent (Within 24-48 hours) | None, assuming patient is medically fit. High suspicion of nerve entrapment. |
| Closed Humeral Fracture with Primary Radial Palsy | Relative | Delayed (3-4 months if no clinical/EMG recovery) | Do not explore acutely unless fracture requires ORIF for other indications. |
| Severe Cubital Tunnel Syndrome (Motor Wasting) | Absolute | Elective but prompt | Avoid simple decompression if nerve subluxates; requires transposition. |
| Acute Sharp Laceration (Radial/Ulnar Nerve) | Absolute | Immediate to Early (Within 1-2 weeks) | Heavily contaminated wounds may require tagging and delayed repair. |
| Delayed Presentation (> 15 months for Radial Nerve) | Contraindicated (for repair) | N/A (Proceed to Salvage) | Irreversible motor endplate degradation makes nerve repair futile. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is the cornerstone of successful peripheral nerve surgery. The clinical evaluation must be exhaustive, documenting precise motor grading using the Medical Research Council (MRC) scale and mapping sensory deficits using static and moving two-point discrimination. For the radial nerve, it is imperative to distinguish between a high radial nerve palsy (involving the triceps), a mid-shaft lesion (sparing the triceps but affecting the brachioradialis and wrist/finger extensors), and a PIN syndrome (sparing the ECRL and superficial sensory branch, resulting in radial deviation during wrist extension). For the ulnar nerve, specific attention must be paid to intrinsic muscle function, evaluating for clawing, Wartenberg's sign, and Froment's sign.
Electrodiagnostic studies, including electromyography (EMG) and nerve conduction studies (NCS), are indispensable tools, though their timing is critical. An EMG performed immediately after an injury is of limited value for localizing a complete lesion, as Wallerian degeneration takes up to 3 weeks to manifest as fibrillation potentials in the denervated muscle. Therefore, a baseline EMG is typically obtained at 3 to 4 weeks post-injury, with serial studies performed at 12 weeks to assess for nascent motor unit action potentials (MUAPs) indicative of early reinnervation. High-resolution ultrasound (HRUS) and magnetic resonance neurography (MRN) have emerged as powerful adjuncts, allowing the surgeon to visualize neuromas, nerve discontinuities, and anatomical entrapment sites prior to incision.
Patient positioning for radial nerve exploration depends entirely on the suspected level of the lesion. For proximal axillary and upper arm exposures, the patient is positioned supine with the arm abducted and externally rotated on an arm board. For mid-to-distal humeral shaft lesions requiring a posterior or lateral approach, the patient may be placed in the lateral decubitus position with the arm draped free over a sterile padded post, allowing for unhindered access to the posterior compartment and facilitating elbow flexion to relax the triceps. Alternatively, a prone position can be utilized for isolated posterior exposures, though this limits access to the anterior compartment if distal extension is required. A sterile tourniquet is highly recommended to maintain a bloodless field, though it should be deflated periodically during prolonged procedures to assess tissue viability and achieve hemostasis.
For ulnar nerve procedures at the elbow, the patient is positioned supine with the arm abducted and externally rotated on a hand table. The elbow is typically flexed to 45-90 degrees during the initial exposure. A sterile tourniquet is applied high on the arm. It is critical to prep and drape the entire limb from the axilla to the fingertips, allowing for intraoperative assessment of nerve tension during full range of motion. For complex nerve reconstructions or microsurgical neurorrhaphy, an operating microscope must be positioned appropriately, and microsurgical instruments, including jeweler's forceps, micro-scissors, and 8-0 or 9-0 nylon sutures, must be readily available on the sterile field.
Step-by-Step Surgical Approach and Fixation Technique
Radial Nerve: Axillary and Proximal Exposure
Exposure of the radial nerve in the axilla and proximal third of the arm requires a meticulous extensile approach, navigating the complex neurovascular anatomy of the proximal brachial plexus. The procedure begins with the patient supine and the arm abducted.
- Incision and Superficial Dissection: Initiate the incision at the tip of the coracoid process, extending it distally along the deltopectoral groove. Curve the incision smoothly into the medial bicipital groove and carry it distally along the medial aspect of the arm. This incision should be positioned slightly more posteriorly than the standard approach for the median or ulnar nerves to facilitate access to the posterior cord.
- Fascial Release and Neurovascular Identification: Incise the deep brachial fascia directly over the neurovascular bundle. The initial dissection focuses on identifying and protecting the superficial structures. Isolate the median nerve and the brachial artery and vein. Retract these structures, along with the ulnar nerve, laterally and anteriorly to expose the deeper fascial planes.
- Deep Dissection and Radial Nerve Isolation: The radial nerve lies deep to the brachial artery, situated between the triceps posteriorly and the coracobrachialis/brachialis complex anteriorly. Carefully dissect the epineurial areolar tissue to isolate the radial nerve. Trace the nerve proximally to its origin from the posterior cord and distally as it gives off its first motor branches to the long and medial heads of the triceps.
- Tracing into the Spiral Groove: Continue the dissection distally, following the nerve as it dives obliquely and posteriorly, accompanied by the profunda brachii vessels, to enter the spiral groove of the humerus. Extreme care must be taken here, as the vascular bundle is intimately associated with the nerve, and aggressive dissection can lead to troublesome bleeding that obscures the surgical field.
Radial Nerve: Mid-to-Distal Humeral Shaft
For lesions involving the mid-to-distal humeral shaft, including those associated with Holstein-Lewis fractures, a posterior or lateral extensile approach is mandatory.
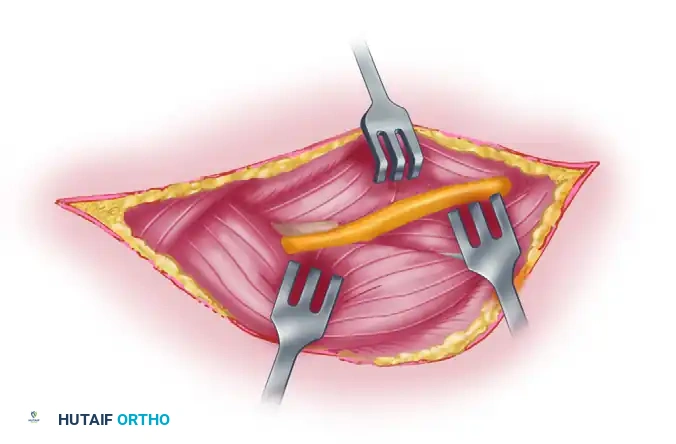
Figure 62-27 A: The skin incision begins at the posterior margin of the deltoid muscle and extends distally in the midline, curving laterally and anteriorly to end at the interval between the brachioradialis and brachialis.
- Posterior Incision and Flap Elevation: Begin the incision along the posterior border of the distal third of the deltoid. Extend it distally in the midline of the posterior arm, curving it laterally as it approaches the lateral epicondyle.
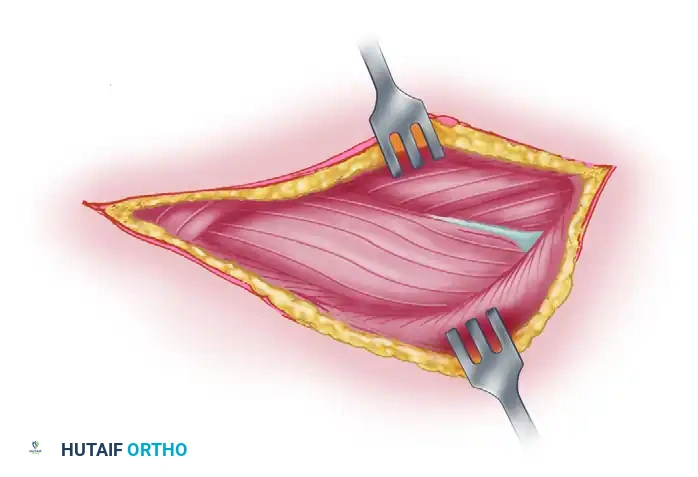
Figure 62-27 B: The posterior skin flap is dissected and retracted. The deep fascia is incised in line with the skin incision. The dotted line indicates the planned incision in the triceps muscle between the long and lateral heads.
- Developing the Triceps Interval: Incise the deep fascia in line with the skin incision. Identify the interval between the long and lateral heads of the triceps brachii. Bluntly develop this avascular plane.
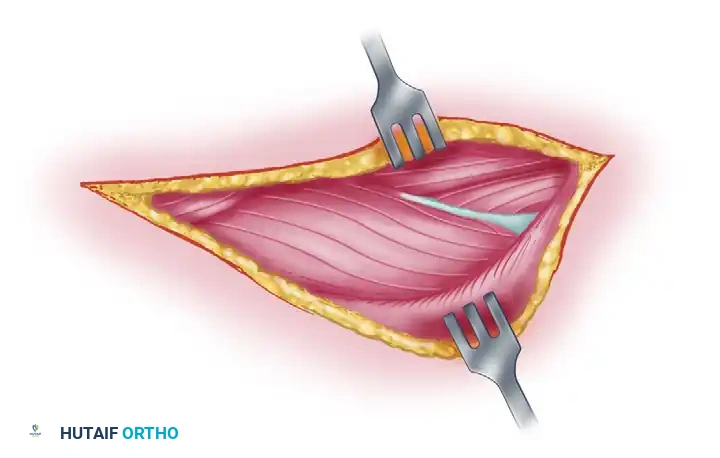
Figure 62-27 C: The radial nerve and accompanying profunda brachii vascular bundle are exposed by retracting the two heads of the triceps muscle. The nerve is dissected to the point where it passes beneath the lateral head of the triceps.
- Identifying the Nerve in the Spiral Groove: Deep retraction of the triceps heads reveals the radial nerve and the profunda brachii vessels lying within the spiral groove. Carefully perform neurolysis, tracing the nerve distally to the point where it passes deep to the lateral head of the triceps and pierces the lateral intermuscular septum.
Figure 62-27 D: The arm is externally rotated. The interval between the proximal end of the brachioradialis and brachialis is dissected, exposing the radial nerve along the anterolateral aspect of the humerus.
- Anterolateral Extension: To expose the nerve in the anterior compartment, curve the distal portion of the incision anteriorly along the medial border of the brachioradialis. Externally rotate the arm. Incise the deep fascia and develop the interval between the brachialis (medial) and the brachioradialis (lateral).
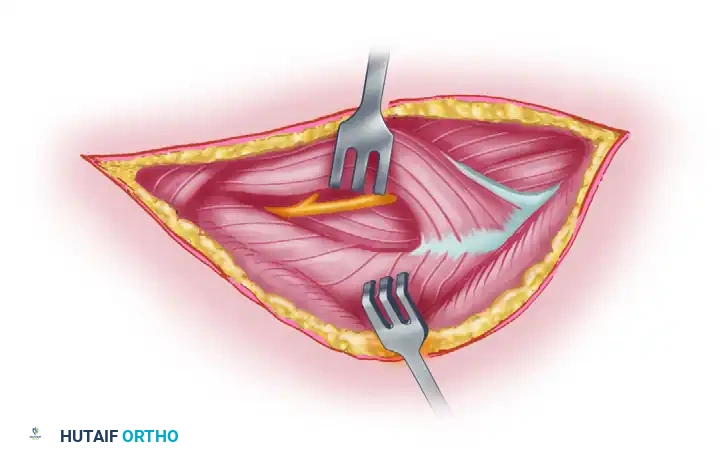
Figure 62-27 E: The dotted line indicates the incision through which the lateral head of the triceps is mobilized from the underlying bone, facilitating exposure of the radial nerve deep to it.
- Releasing the Septum: The most critical step is releasing the lateral intermuscular septum. The nerve is highly vulnerable here. Incise the fascia and mobilize the lateral head of the triceps from the underlying humerus.
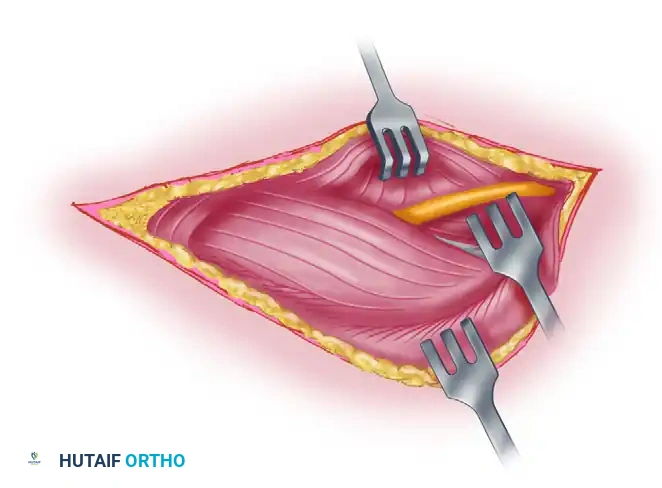
Figure 62-27 F: Final exposure of the radial nerve following mobilization of the lateral triceps head.
- Final Exposure: With the septum released and the triceps mobilized, the radial nerve is fully exposed from the posterior spiral groove down to the radiocapitellar joint. This allows for comprehensive neurolysis, fracture fixation, or nerve repair without undue tension.
Radial Nerve: Posterior Interosseous Nerve (PIN)
Exposure of the deep motor branch (PIN) is required for compressive neuropathies at the Arcade of Frohse or lacerations in the proximal forearm.
Figure 62-28 A: Line of incision for PIN exposure. The forearm is prone, and the elbow is flexed.
- Distal Forearm Incision: With the forearm pronated and the elbow flexed, initiate the incision 8 to 10 centimeters proximal to the lateral epicondyle. Extend it distally across the elbow joint, curving along the radial border of the extensor digitorum communis (EDC) towards the middle of the dorsal forearm.
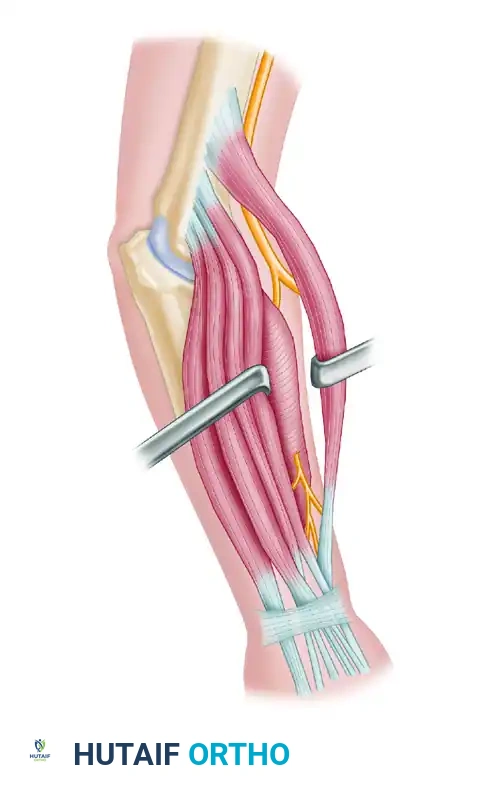
Figure 62-28 D: Alternative line of incision with the elbow extended.
- Identifying the Bifurcation: Deepen the incision through the subcutaneous tissue. Identify the interval between the brachioradialis and the brachialis proximally to locate the main radial nerve. Trace it distally to its bifurcation.

Figure 62-28 C: Diagrammatic representation of the course of the radial nerve and its bifurcation into the superficial sensory branch and the posterior interosseous nerve.
- Protecting the Superficial Branch: Isolate and protect the superficial sensory branch, which continues distally deep to the brachioradialis. Injury to this branch results in painful neuromas that are notoriously difficult to treat.
Figure 62-28 B: The posterior interosseous nerve is exposed as it enters the supinator muscle.
- Supinator Dissection and Release: Follow the PIN as it dives deep into the supinator muscle. Identify the proximal fibrous border of the superficial head of the supinator (Arcade of Frohse). Using tenotomy scissors, meticulously incise
Clinical & Radiographic Imaging Archive