Epineurial Neurorrhaphy: Advanced Microsurgical Techniques

Key Takeaway
Epineurial neurorrhaphy is a foundational microsurgical technique for peripheral nerve repair. It involves the precise coaptation of severed nerve ends by placing sutures exclusively through the epineurium. Achieving a tension-free repair, ensuring accurate fascicular alignment via surface landmarks, and utilizing appropriate magnification are critical for optimal axonal regeneration. This guide details epineurial, perineurial, and combined repair techniques for orthopedic and hand surgeons.
Comprehensive Introduction and Patho-Epidemiology
Peripheral nerve injuries represent one of the most profound and technically demanding reconstructive challenges encountered by the orthopedic and hand surgeon. The ultimate objective of any nerve repair—formally termed neurorrhaphy—is to restore definitive motor and sensory function by facilitating the precise, unimpeded regeneration of axons across the zone of injury. Among the diverse armamentarium of microsurgical techniques available, epineurial neurorrhaphy remains the established gold standard for the primary repair of sharply transected peripheral nerves. The execution of this procedure demands not only meticulous surgical precision but also a profound comprehension of neurobiology and the temporal dynamics of nerve regeneration.
The epidemiology of peripheral nerve injuries (PNIs) dictates that they predominantly affect a young, active demographic, often resulting from high-energy trauma, industrial accidents, or sharp penetrating mechanisms such as glass lacerations. Upper extremity injuries are markedly more common than those in the lower extremity, with the digital, median, ulnar, and radial nerves frequently implicated. Iatrogenic nerve injuries, occurring during complex orthopedic procedures such as fracture fixation, arthroplasty, or tumor resection, also constitute a significant subset of PNIs. The socioeconomic burden of these injuries is staggering, as they frequently lead to prolonged disability, chronic neuropathic pain, and severe loss of occupational function if not managed with immediate and expert surgical intervention.
When a peripheral nerve is severed, a complex, highly orchestrated cellular cascade is initiated. The distal nerve segment undergoes Wallerian degeneration, an inevitable process wherein the severed axons and their surrounding myelin sheaths enzymatically degrade. Macrophages rapidly infiltrate the distal stump to clear the myelin debris, leaving empty endoneurial tubes. Concurrently, Schwann cells proliferate and align longitudinally to form the Bands of Büngner, which serve as biological conduits to guide regenerating axons. Proximally, the neuronal cell body within the anterior horn of the spinal cord or the dorsal root ganglion undergoes chromatolysis, shifting its metabolic machinery from neurotransmitter production to the synthesis of structural proteins required for axonal elongation.
The success of a neurorrhaphy depends entirely on the surgeon’s ability to capitalize on this biological window by coapting the proximal and distal nerve stumps with meticulous fascicular alignment, minimal surgical trauma, and an absolute absence of tension. The regenerating axonal growth cone must traverse the surgical repair site and enter the distal endoneurial tubes. Failure to adhere to strict microsurgical principles results in axonal escape, where axons grow blindly into the surrounding soft tissue, leading to the formation of a painful neuroma, dense fibroplasia, and ultimately, a catastrophic failure of functional recovery. This necessitates a mastery of the micro-environment and the surgical techniques required to optimize it.
Detailed Surgical Anatomy and Biomechanics
To perform a successful neurorrhaphy, the operating surgeon must possess an intimate, three-dimensional understanding of intraneural microanatomy. A peripheral nerve is not merely a bundle of wires; it is a highly organized, metabolically active, and structurally complex organ. The outermost layer is the epineurium, which is conceptually divided into the epifascicular epineurium (the robust external sheath surrounding the entire nerve trunk) and the interfascicular epineurium (the loose, vascularized connective tissue separating individual fascicles). The epineurium provides the primary tensile strength of the nerve and acts as a crucial cushion against compressive forces.
Deep to the epineurium lies the perineurium, a dense, metabolically active, and mechanically formidable layer of connective tissue that surrounds individual fascicles. The perineurium is a critical structure; it maintains the blood-nerve barrier, regulates intrafascicular pressure, and protects the delicate internal environment from external chemical and mechanical fluctuations. Suturing the perineurium directly provides a highly specific mechanical alignment for fascicular repair but inherently risks violating the privileged intraneural environment, potentially introducing foreign body reactions and subsequent scarring. Within the perineurial sheath lies the endoneurium, the delicate connective tissue matrix surrounding individual axons and their associated Schwann cells.
The topographical anatomy of a peripheral nerve is highly variable and changes continuously along its longitudinal axis. Nerves can be classified based on their internal architecture as monofascicular, oligofascicular (containing a few large fascicles), or polyfascicular (containing numerous smaller fascicles). In proximal regions, nerves often exhibit a complex, interwoven polyfascicular plexus-like arrangement, making precise topographical matching exceedingly difficult. As nerves course distally toward their target end-organs, the fascicles tend to segregate into distinct motor and sensory groups, rendering them more amenable to group fascicular or perineurial repair techniques.
Biomechanically, peripheral nerves are viscoelastic structures capable of accommodating a certain degree of physiological excursion and deformation during normal joint movement. However, they are exquisitely sensitive to longitudinal tension. Surgical tension is the absolute enemy of nerve regeneration. The microvascular supply of the nerve, known as the vasa nervorum, consists of a delicate network of longitudinal extrinsic and intrinsic vessels. Elongation of a peripheral nerve by just 8% to 15% significantly decreases intraneural microvascular blood flow, leading to venular occlusion, subsequent arterial ischemia, fibroplasia, and dense scarring at the coaptation site. If a primary repair cannot be achieved without tension, the surgeon must immediately abandon direct coaptation and pivot to nerve grafting or conduit interposition.
Exhaustive Indications and Contraindications
The decision-making process regarding the timing and technique of peripheral nerve repair is dictated by the mechanism of injury, the zone of trauma, the condition of the soft tissue envelope, and the temporal presentation of the patient. Primary repair, performed within the first few days following injury, is the optimal intervention for specific clinical scenarios, whereas delayed repair or reconstruction is mandated for others.
Primary direct neurorrhaphy is unequivocally indicated for sharp, clean transections, such as those caused by glass shards, knife blades, or surgical scalpels. In these scenarios, the zone of injury is highly localized, with minimal crush or avulsion components, allowing for immediate debridement to healthy fascicular tissue without significant loss of nerve length. Iatrogenic nerve transections identified intraoperatively should also be repaired immediately before the conclusion of the primary procedure. The ideal acute window for primary repair is within 48 to 72 hours; during this period, the distal nerve stump remains electrically stimulable (aiding in topographical identification), and significant retraction and epineurial fibrosis have not yet occurred.
Conversely, delayed primary repair (within 2 to 3 weeks) or secondary reconstruction is indicated for blunt trauma, high-energy crush injuries, gunshot wounds, or avulsion injuries. In these high-energy mechanisms, the longitudinal extent of intraneural damage (the zone of injury) is initially indeterminate. Attempting primary repair in a crushed nerve inevitably leads to coaptation of non-viable, fibrotic tissue, resulting in a dense scar block. Delaying the repair allows the true extent of the necrosis to demarcate, enabling the surgeon to accurately resect back to healthy, pouting fascicles, even if this necessitates the subsequent use of an interpositional nerve graft.
Absolute contraindications to primary direct neurorrhaphy include severe, uncontrolled wound contamination, active gross infection, and massive segmental nerve loss where direct approximation would induce ischemia. Furthermore, a highly compromised soft tissue envelope that cannot provide a well-vascularized, gliding bed for the repaired nerve precludes primary repair; in such cases, soft tissue coverage (e.g., free flap transfer) must take precedence or be performed concomitantly.
| Category | Indications for Primary Neurorrhaphy | Contraindications for Primary Neurorrhaphy |
|---|---|---|
| Mechanism of Injury | Sharp, clean lacerations (glass, knife, scalpel). | High-energy crush, severe avulsions, blast injuries. |
| Timing | Acute presentation (ideally < 72 hours). | Delayed presentation with significant retraction (> 3 weeks). |
| Wound Characteristics | Clean wound, adequate soft tissue envelope. | Gross contamination, active infection, inadequate soft tissue coverage. |
| Anatomical Factors | Minimal segmental loss, tension-free coaptation possible. | Massive segmental defect requiring > 15% elongation for closure. |
| Iatrogenic | Intraoperative sharp transection identified immediately. | Delayed recognition of traction/crush neuropraxia or axonotmesis. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is paramount to the success of complex peripheral nerve reconstructions. The clinical evaluation must meticulously document the baseline neurological deficit. Motor function is quantified using the Medical Research Council (MRC) grading system, while sensory function is mapped using static and moving two-point discrimination, as well as Semmes-Weinstein monofilament testing. While electromyography (EMG) and nerve conduction studies (NCS) are of limited utility in the acute setting (as Wallerian degeneration takes up to 3 weeks to manifest electrically), they are critical for establishing a baseline in delayed presentations. Advanced imaging modalities, such as High-Resolution Ultrasound (HRUS) and Magnetic Resonance Neurography (MRN), are increasingly utilized to preoperatively define the exact site of transection, the gap length, and the presence of neuromas.
The operating room setup must be optimized for the highly demanding nature of microsurgery. Ergonomics are critical; the surgeon and assistant must be seated comfortably with adequate arm and wrist support to eliminate physiological tremor. High-quality optical magnification is non-negotiable. While 3.5× to 5× magnifying loupes are sufficient for the initial surgical exposure, neurolysis, and epineurial preparation, an operating microscope (set to 6× to 10× magnification or higher) is strongly recommended for the actual coaptation, particularly for perineurial and group fascicular repairs. The visual clarity provided by the microscope ensures precise needle placement and minimizes inadvertent endoneurial trauma.
A dedicated microsurgical instrumentation tray is required. This must include non-toothed jeweler's forceps (e.g., Dumont #5), specialized microscissors (both straight for epineurial trimming and curved for dissection), a micro-needle holder with a smooth, non-catching jaw, and a background contrast material (typically a sterile blue or green silicone mat). Suture selection is dictated by the specific technique and the size of the nerve. Generally, 8-0 or 9-0 monofilament nylon on spatulated micro-needles is used for epineurial repairs in major nerve trunks, while 10-0 nylon is reserved for delicate perineurial coaptations or digital nerve repairs.
Patient positioning is dictated by the anatomical location of the injured nerve, but the overarching principle is to allow unhindered, circumferential access to the extremity. The limb is typically prepped and draped widely to allow for the harvesting of autologous nerve grafts (e.g., the sural nerve or medial antebrachial cutaneous nerve) should a primary tension-free repair prove impossible. A pneumatic tourniquet is routinely applied to maintain a bloodless field during the initial dissection and debridement. However, it is a critical surgical principle to deflate the tourniquet prior to the final coaptation to achieve absolute pinpoint hemostasis and to visually confirm the restoration of flow within the vasa nervorum across the repair site.
Step-by-Step Surgical Approach and Fixation Technique
General Principles of Nerve Preparation
Regardless of whether an epineurial, perineurial, or combined technique is ultimately selected, the preparation of the nerve ends must adhere strictly to established microsurgical principles. The initial step involves meticulous proximal and distal dissection. The nerve must be mobilized sufficiently to gain length and overcome elastic retraction, but this must be balanced against the risk of devascularization. The segmental mesoneurial blood supply must be preserved wherever possible; excessive, circumferential stripping of the nerve trunk will render the stumps ischemic and doom the repair to failure.
Once mobilized, the traumatized nerve ends must be resected back to healthy, viable tissue. Using a fresh scalpel blade (e.g., a #11 or #15 blade on a sterile wooden tongue depressor) or specialized serrated nerve-cutting scissors, the surgeon gently trims the nerve ends. The resection must continue until healthy neural tissue is encountered. Viable, healthy fascicles will characteristically "mushroom" or pout slightly from the cut end of the epineurium, and the intraneural vascularity will demonstrate punctate bleeding. If the fascicles appear fibrotic, pale, or retracted within the epineurium, further resection is mandatory.
Absolute hemostasis is a non-negotiable prerequisite for coaptation. A hematoma forming at the repair site will inevitably organize into a dense fibrotic scar, creating an impenetrable mechanical barrier to axonal crossing. Hemostasis is achieved using bipolar electrocautery set to the absolute lowest effective wattage. The bipolar forceps must be applied with pinpoint precision only to the specific bleeding vessel within the epineurium or interfascicular tissue; indiscriminate cauterization will cause thermal necrosis of the adjacent delicate endoneurial tubes. Frequent irrigation with heparinized saline is employed to prevent the neural tissues from desiccating under the heat of the operating lights and to wash away micro-thrombi.
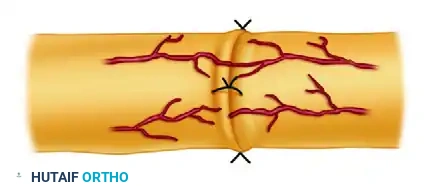
Epineurial Neurorrhaphy Technique
Epineurial neurorrhaphy is the most commonly performed and widely applicable nerve repair technique. It is highly effective for monofascicular or oligofascicular nerves, as well as for polyfascicular nerves where the internal fascicular topography is well-defined, symmetrical, and easily matched.
Under 3.5× to 5× magnification, the surgeon begins by using fine microsurgical scissors to circumferentially dissect and excise the redundant, loose areolar tissue from the external surface of the epineurium, extending a few millimeters proximally and distally from the cut edge. This crucial step prevents the areolar tissue from being inadvertently dragged into the repair site by the suture, which would cause a mechanical block to axonal growth.
Accurate rotational alignment is the single most critical step in epineurial repair. The surgeon must meticulously examine the cross-section of both the proximal and distal stumps. The internal arrangement of the fascicles is mapped, looking for distinct patterns of large and small fascicular groups. Concurrently, the surgeon identifies the longitudinal epineurial blood vessels (vasa nervorum) on the surface of the nerve. Matching these vessels across the laceration provides a highly reliable, extrinsic topographical landmark for ensuring correct rotation.

Once perfect alignment is determined, the background contrast material is placed behind the nerve to optimize visualization. The first suture (typically 8-0 or 9-0 monofilament nylon) is placed through the epineurium on the posterior (deep) surface of the nerve. Placing the posterior suture first is a strategic, fundamental maneuver. If the anterior sutures are placed initially, accessing the posterior aspect of the nerve becomes exceedingly difficult without twisting the nerve trunk, thereby risking disruption of the anterior repair and inducing rotational malalignment.

This initial posterior stitch is tied, or alternatively, the ends are left untied and clamped with a micro-clip to act as a traction and orientation suture. The surgeon then proceeds to place sutures circumferentially around the cut surface. The micro-needle must pass strictly through the epifascicular epineurium, taking bites approximately 1 to 2 mm from the cut edge. The trajectory of the needle must parallel the fascicles to avoid inadvertently piercing them.
The knots are tied with just enough tension to gently approximate the nerve ends. Strangulation of the epineurium will cause immediate ischemia and subsequent necrosis. A completely tension-free repair must be achieved; if the nerve ends pull apart when the traction sutures are released, or if a gap persists between the fascicles, the repair is under excessive tension. In such instances, the primary repair must be aborted in favor of nerve grafting.
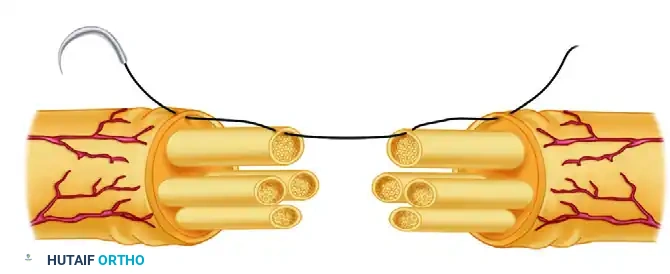
Perineurial (Fascicular) Neurorrhaphy Technique
Perineurial neurorrhaphy involves the direct, selective suturing of individual fascicles or distinct groups of fascicles. This highly specialized technique is indicated for nerves with a distinct polyfascicular architecture where motor and sensory fascicles are clearly segregated and can be reliably identified (e.g., the distal median or ulnar nerve at the level of the wrist).
The procedure begins with the careful excision of the epifascicular epineurium. Using the operating microscope (6× to 10× magnification), the surgeon utilizes micro-scissors to carefully peel back and resect the outer epineurial sheath from the circumference of the cut ends, thereby exposing the underlying fascicles. Following this, the interfascicular epineurium surrounding the specific groups of fascicles is gently dissected and resected to allow for the independent, tension-free mobilization of each fascicular group.
Fascicular mapping is then performed with extreme care. The surgeon attempts to match corresponding groups of fascicles proximally and distally based on their size, shape, and topographical location within the nerve trunk. Intraoperative electrical stimulation of the distal stump (if performed within the acute 72-hour window) can occasionally assist in differentiating motor from sensory fascicles.
Once the fascicles have been definitively matched, coaptation is performed. A 10-0 monofilament nylon suture on a fine, spatulated micro-needle is utilized. The needle is passed strictly through the perineurium—the dense sheath surrounding the individual fascicle—meticulously avoiding the delicate endoneurial contents and the axons within. Typically, two 10-0 sutures are placed through the perineurium at 180 degrees to each other to ensure circumferential alignment and prevent fascicular buckling. A critical pitfall in this technique is over-suturing; introducing excessive foreign body material (nylon) directly into the regenerative pathway stimulates robust intraneural scarring. The absolute minimum number of sutures required to maintain coaptation must be used.
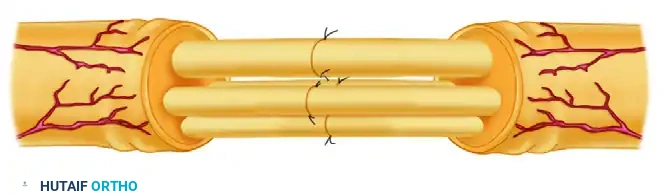
Combined Epineurial-Perineurial Neurorrhaphy Technique
The combined epineurial-perineurial neurorrhaphy is a highly versatile, hybrid technique. It is particularly useful in aligning large groups of fascicles in major peripheral nerve trunks (e.g., the sciatic nerve or the proximal radial nerve) and is frequently the technique of choice when nerves have been incompletely transected. This approach leverages the robust mechanical strength provided by epineurial sutures while simultaneously ensuring the precise topographical alignment afforded by perineurial sutures.
After adequate exposure and the excision of redundant areolar tissue, the cross-section of the nerve is examined, and the large groups of fascicles are matched proximally and distally. The repair typically begins with the central portion of the nerve. The individual deep fascicles or central fascicular groups are coapted using 10-0 nylon sutures placed directly through the perineurium, exactly as described in the isolated perineurial technique.
Once the central fascicles are securely coapted, the surgeon addresses the fascicles and fascicular groups that lie near the periphery of the nerve trunk. For these peripheral structures, a 9-0 nylon suture is typically employed. The needle is passed first through the external epineurium, then directly through the edge of the perineurium of the peripheral fascicle. The surgeon then crosses the laceration site and passes the needle through the matching perineurium on the opposite side, finally exiting through the external epineurium.
This combined, full-thickness stitch securely anchors the peripheral fascicles in perfect alignment while simultaneously closing the outer epineurial sheath. This dual-action technique adds substantial biomechanical strength to the repair, shielding the delicate internal perineurial coaptations from physiological shearing forces during the early phases of rehabilitation.
Complications, Incidence Rates, and Salvage Management
Despite flawless microsurgical technique, peripheral nerve repairs are fraught with potential complications, primarily due to the complex, unforgiving biological nature of axonal regeneration. The most devastating complication is the failure of axonal progression across the repair site, leading to the formation of a terminal neuroma or a neuroma-in-continuity. This occurs when regenerating axons escape the confines of the endoneurial tubes and proliferate haphazardly into the surrounding scar tissue. The pathophysiology is almost always linked to excessive tension at the repair site, rotational malalignment, or an inadequate resection of the initial zone of injury (leaving fibrotic tissue that acts as a physical barrier).
Another significant complication is repair dehiscence or ischemic failure. If a nerve is coapted under even mild tension (exceeding the 8% elongation threshold), the vasa nervorum become occluded. The resulting ischemia leads to profound fibroplasia, effectively strangulating the regenerating axons. Clinically, this presents as a failure of the Tinel's sign to advance distally over time, accompanied by stagnant or deteriorating electromyographic findings at the 3-to-6-month postoperative mark. Infection and wound breakdown, while less common in clean sharp transections, can occur in high-energy open injuries and invariably lead to severe scarring and repair failure. Furthermore, Complex Regional Pain Syndrome (CRPS) can develop, requiring aggressive, multidisciplinary pain management and sympathetic blocks.
When a primary repair fails, or when a massive gap precludes direct coaptation, salvage procedures must be employed. The traditional salvage technique involves the excision of the neuroma and the interposition of autologous nerve grafts (most commonly the reversed sural nerve) to bridge the defect without tension. However, in cases of delayed presentation where the distal motor endplates have irreversibly degraded (typically beyond 12 to 18 months), nerve grafting is futile. In these end-stage scenarios, the surgeon must pivot to regional nerve transfers (neurotization)—such as transferring redundant fascicles of a functioning nerve to the distal motor branch of the injured nerve close to the target muscle—or traditional tendon transfers to restore gross biomechanical function.
| Complication | Estimated Incidence | Pathophysiology / Risk Factors | Salvage Management / Treatment |
|---|---|---|---|
| Neuroma-in-Continuity | 10% - 25% | Axonal escape due to tension, malalignment, or inadequate debridement. | Neuroma excision, nerve grafting, or nerve transfer if distal endplates are viable. |
| Ischemic Scar Block | 15% - 30% | Excessive tension (>8% elongation) causing vasa nervorum occlusion. | Resection of fibrotic segment, tension-free autologous nerve grafting. |
| Repair Dehiscence | < 5% | Extreme tension, premature aggressive mobilization, poor knot-tying technique. | Immediate re-exploration and repair, likely requiring nerve grafting due to retraction. |
| Complex Regional Pain Syndrome (CRPS) | 2% - 10% | Abnormal sympathetic nervous system response to nerve trauma. | Aggressive physical therapy, gabapentinoids, sympathetic nerve blocks. |
| Irreversible Motor Endplate Degeneration | Varies (Time-dependent) | Prolonged denervation (>12-18 months) prior to axonal arrival at the target muscle. | Regional nerve transfers (neurotization) or functional tendon transfers. |
Phased Post-Operative Rehabilitation Protocols
The immediate postoperative period is a highly vulnerable phase for the reconstructed nerve. The microvascular anastomoses of the vasa nervorum and the delicate epineurial sutures are highly susceptible to mechanical disruption. Consequently, the initial wound closure and dressing application must be performed with extreme care. If hemostasis is a concern, small closed-suction Silastic drains may be placed; however, they must be routed far away from the nerve repair site to prevent mechanical interference, suction-induced trauma, or accidental disruption of the coaptation during drain removal. The wound is dressed with a nonadherent, wide-mesh gauze directly adjacent to the incision to prevent the coagulum from adhering, followed by layers of soft gauze and abundant cotton padding applied from the distal extremity extending proximally past the adjacent joints.
During Phase I (Immobilization, Weeks 0 to 3), the limb must be strictly immobilized in a custom-molded plaster or fiberglass splint. The joints adjacent to the injury are positioned in a "position of function" specifically designed to minimize longitudinal tension on the repair. For example, a volar forearm median nerve repair requires the wrist and elbow to be immobilized in slight flexion. This absolute immobilization is maintained for 3 weeks to allow the initial fibrin clot at the coaptation site to organize and for early fibroblastic healing of the epineurium to occur. This biological bridging provides the nascent repair with sufficient tensile strength to withstand gentle movement in subsequent phases.
Phase II (Protected Mobilization, Weeks 3 to 6) involves the gradual modification of the splint to allow for progressive, highly protected active range of motion. The primary objective during this phase is to encourage longitudinal nerve gliding within its soft tissue bed, thereby preventing the formation of dense extraneural adhesions that would tether the nerve and induce traction injuries during normal limb use. Movement is strictly limited to synergistic arcs that do not place stretch on the repair site. Passive stretching is absolutely contraindicated during this phase.
Phase III (Strengthening and Sensory Re-education, Week 6 and beyond) initiates progressive strengthening of the reinnervated musculature and formal sensory re-education protocols. Sensory re-education is critical for harnessing cortical plasticity, helping the brain reinterpret the altered afferent signals arriving from the misdirected regenerating axons. Clinical recovery is meticulously monitored via the advancing Tinel's sign, which is expected to progress distally at a rate of approximately 1 mm per day (or 1 inch per month). Serial electromyography (EMG) is typically initiated at 3 to 6 months
