Microsurgical Nerve Repair and Vein Grafting Techniques
Key Takeaway
Microsurgical neurorrhaphy requires meticulous fascicular alignment and tension-free coaptation to optimize peripheral nerve regeneration. This comprehensive guide details the indications, timing, and step-by-step surgical techniques for epineurial and perineurial repairs. By leveraging high-powered magnification and precise microsurgical principles, orthopedic surgeons can significantly improve functional outcomes in complex nerve injuries, mitigating the risks of neuroma formation and irreversible motor endplate atrophy.
Comprehensive Introduction and Patho-Epidemiology
The restoration of peripheral nerve continuity following traumatic transection remains one of the most technically demanding and biologically complex challenges in orthopedic microsurgery. Despite significant advancements in optical magnification, microsurgical instrumentation, and our understanding of neurobiology, functional recovery following severe peripheral nerve injury is rarely absolute. The clinical outcomes are dictated not merely by the mechanical precision of the neurorrhaphy but by an intricate cascade of cellular events, Wallerian degeneration, and the relentless race between axonal regeneration and target organ atrophy. As such, the operating surgeon must possess a profound understanding of both the macroscopic surgical techniques and the microscopic physiological environment that governs neuroregeneration.
Epidemiologically, peripheral nerve injuries occur in approximately 2% to 3% of all patients admitted to Level I trauma centers, with a significant predilection for the upper extremity. The mechanisms of injury are broadly categorized into sharp lacerations, crush injuries, and traction/avulsion injuries, each presenting distinct pathophysiological profiles. Sharp lacerations, typically sustained from glass, knives, or sheet metal, produce a highly localized zone of injury that is highly amenable to primary microsurgical repair. Conversely, high-energy crush and avulsion injuries, often resulting from motor vehicle collisions or industrial accidents, inflict extensive longitudinal ultrastructural damage. This results in a wide zone of injury characterized by intraneural hemorrhage, edema, and subsequent extensive fibrosis, which profoundly complicates the timing and technique of surgical intervention.
A meticulous and detailed clinical examination of the extremity prior to surgical intervention is of paramount importance, particularly due to the relatively high prevalence of anomalous innervations. Anatomical variants such as the Martin-Gruber anastomosis (a communicating branch from the median to the ulnar nerve in the proximal forearm) or the Riche-Cannieu anastomosis (a connection between the deep branch of the ulnar nerve and the recurrent branch of the median nerve in the hand) are sufficiently common to produce profound confusion when evaluating preoperative deficits and postoperative nerve regeneration. The surgeon must accurately map both motor and sensory deficits to establish an infallible baseline for future comparison. Failure to recognize these anomalies can lead to catastrophic misinterpretations of the injury severity, potentially resulting in the neglect of a transected nerve due to falsely preserved distal motor function.
The ultimate success of peripheral neurorrhaphy is influenced by a multitude of physiological and mechanical factors. The two most critical prognostic determinants are the chronological age of the patient and the amount of tension present at the suture anastomosis. Pediatric patients demonstrate vastly superior neuroplasticity, enhanced central nervous system adaptation, and a more robust peripheral regenerative potential, often achieving functional outcomes that are biologically impossible in the adult population. Furthermore, the anatomical level of the injury plays a crucial role; proximal injuries carry a significantly poorer prognosis due to the sheer distance regenerating axons must traverse before reaching their target motor endplates, which may undergo irreversible fatty infiltration and fibrosis if denervated for prolonged periods (typically beyond 12 to 18 months).
Detailed Surgical Anatomy and Biomechanics
A profound comprehension of peripheral nerve microanatomy is the foundational prerequisite for successful microsurgical repair. A peripheral nerve is not a simple biological cable, but rather a highly complex, organized, and dynamic organ system. The outermost layer, the adventitia or mesoneurium, is a loose areolar tissue that allows the nerve to glide smoothly against surrounding fascial planes during joint motion. Immediately deep to this is the epineurium, which is subdivided into the epifascicular epineurium (the outer sheath) and the interfascicular epineurium (the loose connective tissue separating individual fascicles). The epineurium acts as a vital mechanical shock absorber, protecting the delicate internal structures from compressive and tensile forces.
The functional subunits of the nerve are the fascicles, which are individually encased by the perineurium. The perineurium is a robust, multilaminated structure composed of specialized perineurial cells and tight junctions that form the critical blood-nerve barrier. This barrier maintains the specialized endoneurial fluid pressure and protects the axons from toxic macromolecules and inflammatory mediators. Within the perineurium lies the endoneurium, a delicate collagenous matrix that surrounds individual axons and their associated Schwann cells. Understanding this topographical arrangement is crucial, as the fascicular pattern changes continuously along the longitudinal axis of the nerve, forming complex intraneural plexuses. This means that a nerve transected and retracted by even a few centimeters will present a vastly different cross-sectional fascicular map at the proximal and distal stumps, severely complicating precise anatomical alignment.
The vascular supply to the peripheral nerve, the vasa nervorum, is an intricate dual system consisting of extrinsic and intrinsic networks. The extrinsic system comprises segmental regional vessels that enter the nerve via the mesoneurium and arborize within the epineurium. These vessels anastomose with the intrinsic system, a highly redundant longitudinal plexus of microvessels traveling within the epineurium, perineurium, and endoneurium. During surgical mobilization, the surgeon must exercise extreme caution to preserve the segmental extrinsic vessels wherever possible. Aggressive stripping of the mesoneurium will devascularize the nerve ends, leading to ischemic necrosis of the repair site, exuberant intraneural scarring, and an impenetrable barrier to advancing axonal growth cones.
Biomechanically, peripheral nerves possess distinct viscoelastic properties that dictate their response to tension. The undulating course of the fascicles and the elasticity of the epineurium allow a nerve to stretch up to 8% of its resting length without significant physiological compromise. However, elongation beyond this critical threshold induces a precipitous decline in intraneural microcirculation. Studies have demonstrated that at 8% elongation, venular flow begins to stagnate; at 15% elongation, all intraneural blood flow ceases entirely, leading to profound ischemia. A neurorrhaphy performed under such tension will inevitably suffer from ischemic fibrosis, resulting in a dense neuroma-in-continuity and absolute failure of axonal progression. Therefore, the absolute mandate of peripheral nerve surgery is a tension-free coaptation, necessitating the use of nerve grafts or biological conduits whenever this mechanical limit is breached.
Exhaustive Indications and Contraindications
The decision-making algorithm for peripheral nerve repair is governed by the mechanism of injury, the condition of the soft tissue envelope, the longitudinal extent of the nerve damage, and the precise timing of presentation. Surgical intervention must be meticulously tailored to the specific biological environment of the wound. The timing of repair is generally classified into primary, delayed primary, and secondary interventions, each carrying strict indications and potential pitfalls.
Primary repair, performed within the first 24 hours of injury, is the gold standard for clean, sharp lacerations, such as those inflicted by glass or surgical scalpels. The primary indication is a stable patient with a well-circumscribed wound devoid of gross contamination or extensive crush injury. In these scenarios, the nerve ends have not yet retracted significantly, and the fascicular topography remains easily identifiable, allowing for optimal anatomical alignment. Delayed primary repair, undertaken between 2 and 18 days post-injury, is indicated when initial wound conditions preclude immediate microsurgery—such as heavily contaminated wounds requiring serial debridement, or situations where specialized microsurgical equipment and personnel are initially unavailable.
Secondary repair, performed beyond 18 days but typically within 3 months, is strictly indicated for high-energy crush, stretch, or avulsion injuries. In these mechanisms, the true longitudinal extent of intraneural damage is initially occult. Attempting primary repair in a crush injury inevitably leads to coaptation of traumatized, non-viable fascicles, resulting in massive scar formation. Delaying the repair allows the zone of injury to fully demarcate. When the surgeon re-explores the wound weeks later, the fibrotic neuroma at the proximal stump and the glioma at the distal stump can be serially sectioned until healthy, pouting fascicles are definitively identified, ensuring a biologically sound environment for regeneration.
When direct, tension-free repair is impossible, the surgeon must bridge the gap. Microvascular vein grafting is highly indicated for bridging short nerve gaps, typically less than 3 centimeters, in small-diameter nerves such as digital nerves or sensory branches. Autologous nerve grafting (e.g., using the sural nerve) remains the gold standard for gaps exceeding 3 centimeters or for large, mixed motor-sensory nerves.
| Intervention Type | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Primary Direct Repair | Clean, sharp lacerations (glass, knife); < 24 hours old; tension-free approximation possible. | High-energy crush/avulsion injuries; gross wound contamination; hemodynamic instability. | Lack of microsurgical equipment/expertise; severe concomitant skeletal instability. |
| Delayed/Secondary Repair | Crush/stretch injuries; contaminated wounds post-debridement; gaps requiring demarcation. | Delay > 18-24 months (irreversible motor endplate atrophy). | Poor soft tissue bed coverage; untreated osteomyelitis. |
| Vein Graft Conduit | Nerve gaps < 3 cm; small sensory nerves (e.g., digital nerves); tension > 8% on direct repair. | Gaps > 3 cm; large mixed nerves (e.g., sciatic, main trunk median/ulnar). | Venous insufficiency; inadequate donor vein caliber. |
| Autologous Nerve Graft | Gaps > 3 cm; large mixed nerves; failed primary repairs requiring excision. | Inadequate soft tissue bed (requires vascularized bed for graft survival). | Patient refusal of donor site morbidity (e.g., sural nerve harvest). |
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative preparation for microsurgical nerve repair demands an exhaustive clinical evaluation and sophisticated logistical planning. The physical examination must painstakingly document two-point discrimination, specific motor strength grading, and the presence of any autonomic dysfunction (such as anhidrosis). In cases of delayed presentation, electrodiagnostic studies (EMG and Nerve Conduction Velocities) are indispensable. However, the surgeon must remember that Wallerian degeneration takes up to 3 weeks to fully manifest electrophysiologically; thus, early EMG studies may yield falsely reassuring results and are generally deferred until 3 to 4 weeks post-injury. High-resolution ultrasound and Magnetic Resonance Neurography (MRN) are increasingly utilized to delineate the exact site of transection, the presence of neuroma formation, and the longitudinal extent of the gap, thereby allowing the surgeon to anticipate the need for autologous grafts or conduits.
The operating room setup is critical to the success of the procedure. The use of a high-quality operating microscope (e.g., Zeiss or Leica platforms) equipped with dual-viewing heads for the primary surgeon and assistant is non-negotiable for perineurial and epiperineurial techniques. The microscope must be balanced and draped prior to the patient entering the room to minimize ischemic time once the tourniquet is inflated. Microsurgical instrumentation must be meticulously inspected; jeweler’s forceps (No. 2 and No. 5), micro-scissors with serrated blades to prevent nerve extrusion during cutting, and diamond-tipped needle holders must be pristine. Suture selection typically involves 8-0 or 9-0 monofilament nylon for epineurial repairs of large nerves, and 10-0 or 11-0 nylon on a micro-spatula needle for perineurial or digital nerve repairs.
Patient positioning must optimize both surgical access and the ergonomics of the microsurgeon. Microsurgery demands absolute stillness; therefore, the surgeon must be seated comfortably with forearms fully supported to eliminate physiological tremor. For upper extremity repairs, the patient is positioned supine with the arm extended on a radiolucent hand table. A pneumatic tourniquet is applied to the proximal limb. Ischemic time management is critical; the tourniquet is typically inflated to 250 mmHg for the upper extremity to provide a bloodless field during the initial dissection, neuroma resection, and fascicular identification.
Crucially, before the final microsurgical coaptation is performed, the tourniquet should be deflated. This serves two vital purposes: first, it allows for meticulous bipolar micro-hemostasis of the epineurial vessels, preventing postoperative intraneural hematoma formation which can catastrophically compress regenerating fascicles. Second, it allows the surgeon to visualize the hyperemic response of the vasa nervorum, confirming that the mobilized nerve ends possess adequate vascularity to support the immense metabolic demands of axonal regeneration. Only after absolute hemostasis is achieved and tissue viability is confirmed should the final suturing commence.
Step-by-Step Surgical Approach and Fixation Technique
The application of microsurgical techniques to neurorrhaphy requires rigorous discipline, specialized instrumentation, and a deep understanding of nerve topography. The primary goal is to achieve a tension-free, anatomically precise coaptation of viable nerve fascicles. The surgical approach begins with generous longitudinal incisions, avoiding crossing flexion creases at 90-degree angles to prevent scar contracture. The nerve is always identified in pristine, uninjured tissue both proximally and distally before tracing it into the zone of injury.
Once the nerve ends are exposed using standard surgical loupes (3.5× to 4.5× magnification), the surgeon transitions to the operating microscope at low to medium magnification (6× to 10×). The nerve ends must be mobilized sufficiently to allow for approximation, but the surgeon must strictly adhere to the principle of preserving the mesoneurium to protect the extrinsic blood supply. The preparation of the nerve stumps is arguably the most critical step. Using a diamond knife or a fresh scalpel blade (No. 11 or 15) pressed against a sterile wooden tongue depressor, the surgeon serially sections the proximal and distal stumps. This is continued until healthy, "pouting" or "mushrooming" fascicles are visualized, indicating healthy endoneurial tissue free of fibrotic scarring.
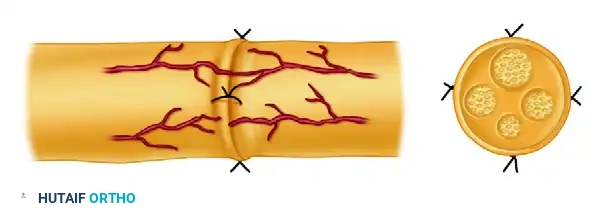
Rotational alignment is the next critical phase. The surgeon must meticulously align the nerve ends by matching the longitudinal surface epineurial blood vessels across the gap. Furthermore, the relative size, shape, and topographical position of the internal fascicles must be matched. For complex polyfascicular nerves, a grouped fascicular (epiperineurial) repair is often employed to ensure motor and sensory fascicles are accurately directed to their corresponding distal pathways.
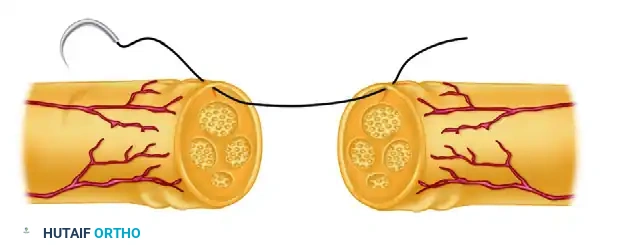
FIGURE 63-5 A: Suture placed through the epineurium, maintaining precise rotational alignment according to surface vessels and the relative size and position of the underlying fascicles.
The suturing process begins with the placement of the initial epineurial coaptation sutures. Using a 9-0 or 10-0 monofilament nylon suture on a micro-spatula needle, the first suture is passed through the epineurium, taking care to bite only the epifascicular layer without piercing the underlying perineurium. A second epineurial suture is then placed exactly 180 degrees opposite the first. These two primary sutures establish the structural framework of the repair.
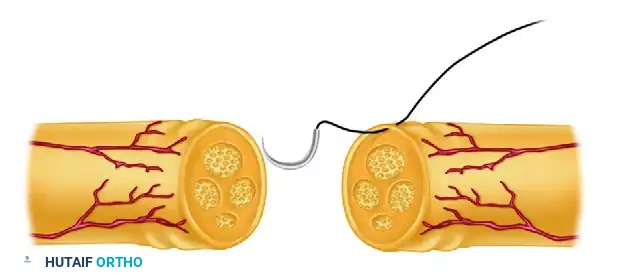
FIGURE 63-5 B: Initial sutures are left untied or tied and left long for traction, providing rotational control of the nerve cylinder.
These initial sutures are often tied and left long to serve as traction sutures. This elegant technique allows the surgeon to gently rotate the nerve cylinder by pulling the traction sutures in opposite directions, granting access to the posterior aspect of the coaptation site without ever grasping the delicate nerve tissue with forceps. Once the posterior wall is visualized, interrupted sutures are placed circumferentially.
FIGURE 63-5 C: Neurorrhaphy completed with interrupted sutures placed circumferentially. The repair must be entirely tension-free to ensure optimal intraneural vascularity.
When a gap exists that exceeds physiological tension limits (typically > 8% elongation, or a gap of 1-3 cm), microvascular vein grafting is a highly effective biological conduit. An autologous vein, such as a dorsal hand vein or the distal saphenous vein, is harvested. The vein graft serves as a physical guide for regenerating axons, preventing the ingrowth of surrounding scar tissue while simultaneously concentrating neurotrophic factors secreted by the severed nerve ends. Crucially, the "Inside-Out" technique is frequently employed. The vein is either reversed anatomically or literally turned inside-out. This ensures that the venous valves do not physically obstruct advancing regenerating axons. Furthermore, the empty conduit provides an optimal microenvironment for Schwann cell migration and the clearance of myelin debris, which are critical phases of Wallerian degeneration preceding axonal sprouting. The vein is sutured to the epineurium of the proximal and distal stumps using 10-0 nylon, ensuring the nerve fascicles are gently drawn into the lumen of the vein without buckling.
Complications, Incidence Rates, and Salvage Management
Despite flawless microsurgical technique, peripheral nerve repairs are fraught with potential complications, primarily due to the unpredictable nature of neurobiology and the absolute reliance on the patient's intrinsic regenerative capacity. The most devastating complication is the failure of axonal regeneration, which inevitably leads to irreversible atrophy of the target motor endplates and permanent functional deficits. This failure is most commonly caused by excessive tension at the repair site, leading to ischemia, intraneural fibrosis, and the formation of a dense neuroma-in-continuity that acts as an impenetrable physical barrier to the advancing growth cones.
Another significant complication is the rupture of the suture line postoperatively. This typically occurs due to patient non-compliance with immobilization protocols or an overly aggressive transition to physical therapy. A ruptured repair site will rapidly fill with dense scar tissue, necessitating a complex secondary revision surgery that almost always requires interpositional nerve grafting due to the resultant retraction and tissue loss. Neuropathic pain and Complex Regional Pain Syndrome (CRPS) are also profound complications, particularly following crush injuries or injuries involving major mixed nerves like the median or sciatic nerves. The aberrant regeneration of sensory fibers can lead to debilitating hyperalgesia and allodynia, which are notoriously refractory to standard pharmacological management.
When a primary or secondary repair fails, the surgeon must pivot to salvage procedures. If an advancing Tinel's sign halts for more than 3 to 4 months, or if serial EMG studies show no evidence of nascent motor unit potentials, surgical re-exploration is mandatory. If a neuroma-in-continuity is identified, intraoperative nerve action potential (NAP) monitoring is utilized. If no NAP is conducted across the lesion, the neuroma must be excised and bridged with autologous nerve grafts. In cases of delayed presentation where the motor endplates have already undergone irreversible fatty degeneration (typically > 12-18 months), nerve repair is futile. In these scenarios, the surgeon must rely on regional tendon transfers (e.g., radial nerve palsy tendon transfers) or free functioning muscle transfers (e.g., gracilis transfer for brachial plexus injuries) to restore functional biomechanics to the extremity.
| Complication | Estimated Incidence | Pathophysiology & Risk Factors | Prevention and Salvage Management |
|---|---|---|---|
| Neuroma-in-Continuity | 10% - 25% | Ischemic fibrosis due to tension; inadequate resection of traumatized fascicles. | Prevention: Tension-free repair; adequate serial sectioning. Salvage: Excision and interfascicular nerve grafting; NAP monitoring. |
| Suture Line Rupture | 2% - 5% | Premature mobilization; inadequate splinting; excessive initial tension. | Prevention: Strict 3-week immobilization in tension-relieving posture. Salvage: Re-exploration and autologous nerve grafting. |
| Complex Regional Pain Syndrome (CRPS) | 5% - 15% | Aberrant sensory regeneration; prolonged immobilization; psychological factors. | Prevention: Early protected mobilization; aggressive pain management. Salvage: Stellate ganglion blocks; gabapentinoids; neuromodulation. |
| Irreversible Motor Endplate Atrophy | Variable (Time-dependent) | Prolonged denervation (>12-18 months); slow regeneration over long distances. | Prevention: Early diagnosis and repair; use of distal nerve transfers (e.g., Oberlin transfer). Salvage: Tendon transfers; free functioning muscle transfers. |
Phased Post-Operative Rehabilitation Protocols
The technical brilliance of a microsurgical nerve repair is easily rendered obsolete by an inadequate or poorly executed postoperative rehabilitation protocol. The healing nerve requires a delicate balance between absolute protection during the initial phase of collagen cross-linking and controlled mechanical stress to promote physiological nerve gliding and prevent extraneural tethering. The rehabilitation process is highly specialized and is typically divided into three distinct, biologically driven phases.
Phase I: Immobilization (Weeks 0-3)
Immediately postoperatively, the extremity is immobilized in a custom-fabricated, well-padded orthosis. The primary objective during this phase is the absolute protection of the micro-suture line. The adjacent joints are positioned to minimize tension on the repair site. For example, following a median nerve repair at the wrist, the splint maintains the wrist in 20 to 30 degrees of flexion, with the metacarpophalangeal joints slightly flexed. Immobilization is strictly maintained for a minimum of 3 weeks. During this time, the fibrin clot at the coaptation site organizes, and early fibroblast proliferation provides the initial tensile strength necessary to withstand subsequent mobilization.
Phase II: Protected Mobilization (Weeks 3-6)
At the 3-week mark, the biological integrity of the repair is sufficient to tolerate gentle, controlled stress. The static splint is transitioned to a dynamic or hinged orthosis that physically blocks extension past the point of tension but allows active and passive flexion. Supervised range-of-motion exercises are initiated by a specialized hand therapist. The goal of this phase is to promote nerve gliding within its soft tissue bed. Excursion of the nerve prevents the formation of dense extraneural adhesions that can tether the nerve, causing secondary traction injuries during normal joint movement. The extension block is gradually reduced by 10 to 15 degrees per week until full extension is achieved.
Phase III: Sensory Re-education and Strengthening (Weeks 6+)
As the regenerating axons cross the repair site and begin their descent down the distal nerve sheath (a progress clinically tracked by an advancing Tinel's sign, averaging 1 mm per day or approximately 1 inch per month), the focus shifts to cortical integration and muscular rehabilitation. Sensory re-education protocols are paramount. Because axonal misdirection at the repair site is inevitable, the brain receives scrambled sensory signals from the periphery. Sensory re-education involves cortical retraining using varied textures, shapes, and temperatures to help the somatosensory cortex reinterpret this altered input. Motor strengthening is delayed until there is definitive clinical or electromyographic (EMG) evidence of reinnervation at the target muscle endplates, at which point progressive resistance exercises are integrated to combat disuse atrophy.
Summary of Landmark Literature and Clinical Guidelines
The evolution of peripheral nerve microsurgery is deeply rooted in a rich history of landmark anatomical studies and pioneering surgical innovations. The foundational topographical work of Sir Sydney Sunderland in the mid-20th century remains the bedrock of modern nerve repair. Sunderland meticulously mapped the internal fascicular architecture of major peripheral nerves, demonstrating that the fascicular pattern changes every few millimeters due to complex intraneural plexus formations. This monumental discovery shifted the surgical paradigm away from blind epineurial approximations toward the necessity of precise rotational alignment and the development of grouped fascicular repair techniques, aiming to minimize the catastrophic misdirection of motor axons down sensory endoneurial tubes.
Similarly, the clinical classifications proposed by Sir Herbert Seddon (Neuropraxia, Axonotmesis, Neurotmesis) and later expanded by Sunderland into a five-degree grading system, continue to dictate the modern indications for surgical intervention. These classifications provided the first biological framework for predicting spontaneous recovery versus the absolute necessity for surgical resection and grafting. In the realm of microvascular physiology, the seminal studies by Göran Lundborg elucidated the critical importance of the vasa nervorum and the devastating effects of tension on intraneural microcirculation. Lundborg's work definitively established the 8% elongation threshold, cementing the modern absolute mandate for tension-free repairs and validating the use of nerve grafts and conduits.
In contemporary practice, the guidelines set forth by the American Society for Surgery of the Hand (ASSH) and the American Academy of Orthopaedic Surgeons (AAOS) heavily emphasize the utilization of advanced microsurgical techniques, the critical timing of intervention, and the emerging role of biological conduits. While autologous nerve grafting remains the gold standard for large gaps, the literature over the past two decades has robustly validated the use of microvascular vein grafts and synthetic collagen conduits for small, non-critical sensory nerve gaps (< 3 cm). Furthermore, the pioneering work of Susan Mackinnon in the popularization of distal nerve transfers (such as the transfer of redundant fascicles of the ulnar nerve to the motor branch of the biceps for brachial plexus avulsions) has revolutionized the salvage management of proximal nerve injuries, offering functional restoration previously deemed impossible.
🔗 Read the comprehensive guide: Wrist Nerve Injuries: Anatomy, Epidemiology, & Advanced Surgical Repair
