Welcome, fellows and colleagues, to the operating theater and this definitive masterclass. Today, we are tackling metacarpal fractures, a ubiquitous yet functionally critical injury that demands absolute precision in both decision-making and surgical execution. Our primary directive is not merely the radiographic restoration of osseous continuity; rather, it is the meticulous reconstruction of the hand’s intricate biomechanical engine, ensuring optimal, pain-free long-term kinematics for our patient. This endeavor transcends the simple application of screws and plates; it requires a profound, three-dimensional understanding of micro-anatomy, soft-tissue envelopes, and the nuanced interplay of intrinsic and extrinsic forces that dictate the patient’s ultimate return to high-level activity.
Comprehensive Introduction and Patho-Epidemiology
Metacarpal fractures represent a substantial proportion of all upper extremity trauma, accounting for approximately 18% to 44% of all hand fractures. Their epidemiological footprint is vast, disproportionately affecting the young, active, and working-age populations, thereby imposing a significant socioeconomic burden due to lost productivity and prolonged rehabilitation. The pathogenesis of these injuries spans a broad spectrum of energy transfer. The majority arise from one of two primary mechanisms: an axial load transmitted along the metacarpal shaft—classically seen in the "boxer's fracture" of the fifth metacarpal neck following a closed-fist strike—or high-energy, direct-impact trauma, such as motor vehicle collisions or industrial crush injuries, which often yield complex, comminuted, or multi-digit fracture patterns.
A metacarpal fracture, at its core, is a structural failure of the longitudinal pillars that bridge the stable carpal arch to the highly mobile phalanges. The clinical significance of this disruption is directly proportional to its deleterious effect on the associated digit's functional cascade. While a vast majority of closed, non-displaced, or minimally angulated metacarpal fractures can be managed successfully with conservative immobilization, the threshold for surgical intervention is crossed when the inherent sequelae of the fracture—namely shortening, rotation, and severe angulation—threaten to permanently compromise the hand's biomechanical efficiency.
Intra-articular fractures, particularly those involving the metacarpophalangeal (MCP) joint, introduce a heightened, often unforgiving risk of post-traumatic stiffness and early-onset osteoarthritis. These injuries demand anatomical reduction of the articular surface to minimize step-offs and restore the congruent gliding mechanism of the joint. Conversely, carpometacarpal (CMC) joint injuries, especially those involving the border digits (thumb and small finger), present unique challenges involving fracture-dislocations that require specialized fixation strategies to prevent chronic instability and grip weakness.
The modern paradigm of metacarpal fracture management has progressively shifted away from prolonged periods of cast immobilization towards principles of stable internal fixation and immediate, aggressive postoperative mobilization. This evolution is driven by the recognition that the soft-tissue complications of immobilization—specifically extensor tendon adhesions and capsular contractures—are often more debilitating than the osseous injury itself. Our surgical objective, therefore, is to achieve an osteosynthesis robust enough to withstand the physiological loads of early active motion, thereby winning the race against restrictive scar tissue formation.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel is ever raised, an intimate, almost intuitive grasp of the hand's surgical anatomy is absolutely paramount. The hand is an unforgiving marvel of biological engineering; a thorough understanding of its osteology, musculature, and neurovascular networks is the foundation upon which successful surgical outcomes are built.
Osteology and Architecture
The metacarpals are sophisticated, long tubular bones characterized by a distinct, roughly triangular cross-section in their diaphyseal regions. The relatively flat dorsal surface provides a natural, albeit limited, footprint for plate application, while the medial and lateral cortices converge volarly to form the apex of the triangle. This unique geometry is not merely morphological; it dictates the bone's inherent biomechanical strength, optimizing its resistance to the complex bending and torsional forces experienced during grip and pinch activities.

The mid-diaphyseal region, particularly within the fourth metacarpal, can be remarkably narrow and gracile. This anatomical bottleneck makes it inherently vulnerable to specific torsional fracture patterns, such as long spiral fractures, and demands meticulous, delicate handling during surgical manipulation and hardware placement. Furthermore, the intramedullary canal exhibits significant morphological variation, typically featuring an hourglass shape with the narrowest isthmus located in the midshaft. This constraint must be carefully evaluated when considering intramedullary fixation techniques, as aggressive reaming or the insertion of oversized implants can precipitate iatrogenic comminution or cortical blowout.
At their proximal extents, the metacarpal bases articulate with the distal carpal row, forming the CMC joints. The index and long finger CMC joints are highly constrained, interlocking articulations that form the rigid central pillar of the hand. In stark contrast, the ring and small finger CMC joints are highly mobile, allowing for the critical cupping motion of the palm. This differential mobility dictates our tolerance for angular deformity: the rigid central metacarpals tolerate almost no sagittal angulation, whereas the mobile ulnar metacarpals can compensate for significantly greater degrees of apex-dorsal angulation.
Musculature, Tendon Systems, and Soft Tissue Envelope
The metacarpals are intimately enveloped by a dense, highly functional network of intrinsic muscles and extrinsic tendinous structures. The dorsal and volar interossei muscles lie adjacent to the medial and lateral surfaces of the metacarpal shafts. In their undisturbed state, these muscle bellies provide a rich, robust periosteal blood supply crucial for primary and secondary fracture healing. However, severe trauma or overly aggressive surgical stripping can lead to localized ischemia, profound scarring, and the devastating complication of intrinsic plus contracture.

The extensor apparatus is a complex, delicate system that drapes over the dorsal aspect of the metacarpals and the MCP joints. It comprises the extrinsic extensor tendons (EDC, EIP, EDQ), the sagittal bands that centralize the tendons over the metacarpal heads, and the dorsal joint capsule. Deep to this, the proper collateral ligaments originate from distinct dorsal tubercles on the metacarpal heads and insert onto the volar base of the proximal phalanges. Due to the eccentric, "cam-shaped" profile of the metacarpal head, these ligaments are lax in extension and maximally taut in flexion. Prolonged immobilization in extension allows these ligaments to shorten and fibrose, leading to intractable MCP joint extension contractures.
The deep transverse intermetacarpal ligaments (DTML) are robust, unyielding fascial bands connecting the volar plates of adjacent MCP joints. These structures play a critical, often underappreciated role in limiting deformity following low-energy metacarpal neck and shaft fractures. They effectively tether the metacarpal heads, typically restricting longitudinal shortening to approximately 3 to 5 millimeters. When shortening exceeds this threshold, it is a definitive clinical indicator that the DTML complex has been compromised, predisposing the digit to significant biomechanical dysfunction and necessitating operative restoration of length.
Neurovascular Considerations and Biomechanics
The dorsal aspect of the hand, the primary territory for our surgical approaches, is traversed by a delicate arborization of dorsal sensory nerves. The superficial branch of the radial nerve and the dorsal sensory branch of the ulnar nerve cross the bases of the border metacarpals and are highly susceptible to iatrogenic traction, compression, or transection. We must meticulously identify, mobilize, and protect these neural structures to prevent the formation of agonizing neuromas or debilitating areas of dysesthesia that can ruin an otherwise technically perfect osteosynthesis.
The vascular supply to the metacarpals is dual-sourced. The nutrient arteries, branching from the deep palmar arch, enter the volar aspect of the midshaft and course proximally. The periosteal vessels, supplied by the dorsal and palmar metacarpal arteries, rely heavily on the integrity of the attached interossei muscles. Extensive subperiosteal dissection during open reduction jeopardizes this delicate vascular network, increasing the risk of delayed union or nonunion. Thus, the modern surgeon must employ "minimal touch" techniques, preserving soft-tissue attachments wherever possible.
Biomechanically, metacarpal fractures are subject to predictable deforming forces. Extra-articular shaft and neck fractures almost universally collapse into apex-dorsal angulation. This is a direct consequence of the volar flexion forces exerted by the intrinsic interossei and lumbricals, combined with the proximal pull of the extrinsic flexors and extensors. Furthermore, rotational malalignment is the most poorly tolerated of all deformities. Because the digits normally converge toward the scaphoid tubercle during flexion, even a subtle 5-degree rotational malrotation at the metacarpal shaft translates to a 1.5-centimeter overlap at the fingertip, resulting in debilitating digital scissoring that severely impairs grasp mechanics.
Exhaustive Indications and Contraindications
The decision to transition a patient from conservative management to the operating theater is governed by a rigorous, evidence-based evaluation of the fracture's inherent stability and its projected impact on hand kinematics. The overarching philosophy of surgical decision-making requires the surgeon to constantly balance the biological "hit" of the surgical approach against the mechanical necessity of rigid stabilization.
Absolute indications for operative intervention are non-negotiable scenarios where conservative management is guaranteed to yield an unacceptable functional outcome. Chief among these is rotational malalignment. As previously established, any degree of clinical scissoring during digital flexion is an absolute mandate for surgical derotation and fixation. Open fractures, particularly those heavily contaminated or resulting from human or animal bites ("fight bites"), require urgent surgical débridement, irrigation, and concurrent stabilization to mitigate the catastrophic risk of deep space infection and osteomyelitis. Furthermore, highly unstable fractures, such as those involving the border metacarpals (index and small finger) which lack the tethering support of adjacent intact rays on both sides, typically demand surgical fixation to prevent progressive collapse.
Relative indications require a more nuanced, individualized assessment, weighing patient-specific functional demands against established deformity thresholds. Shortening greater than 5 millimeters is a strong relative indication, as biomechanical studies have demonstrated that every 2 millimeters of metacarpal shortening results in an average of 7 degrees of extensor lag at the MCP joint, significantly weakening grip strength. Angular deformity thresholds are digit-specific due to the compensatory mobility of the CMC joints. The index and long fingers tolerate less than 10 to 15 degrees of apex-dorsal angulation. In contrast, the ring finger can tolerate up to 30 degrees, and the small finger up to 45 degrees, before the palmar prominence of the metacarpal head causes painful grip interference or pseudo-clawing.
Contraindications to surgical intervention, while less common, must be strictly respected to avoid doing harm. Absolute contraindications include patients who are medically unstable and cannot tolerate anesthesia, or those with active, untreated local soft-tissue infections that preclude the safe implantation of hardware. Relative contraindications encompass severe, pre-existing soft-tissue compromise—such as massive crush injuries with impending necrosis or severe burns—where surgical incisions would precipitate catastrophic wound breakdown. Additionally, extreme patient non-compliance or severe cognitive impairment that precludes adherence to postoperative rehabilitation protocols may tip the scales toward conservative management, as early motion is the linchpin of surgical success.
| Parameter | Operative Indications | Contraindications |
|---|---|---|
| Clinical Presentation | Rotational malalignment (scissoring) | Medically unstable for anesthesia |
| Soft Tissue Status | Open fractures requiring débridement | Active, untreated local infection |
| Anatomical Location | Multiple adjacent metacarpal fractures | Severe overlying soft-tissue necrosis |
| Shortening | > 5 mm of longitudinal collapse | Extreme patient non-compliance |
| Angulation (Index/Long) | > 10 - 15 degrees apex-dorsal | Pre-existing severe joint contracture |
| Angulation (Ring/Small) | > 30 - 45 degrees apex-dorsal | Lack of functional demand (bedbound) |
| Articular Involvement | > 1-2 mm step-off at MCP/CMC joint | Terminal illness with short life expectancy |
Pre-Operative Planning, Templating, and Patient Positioning
The success of any complex orthopedic intervention is largely predetermined before the patient enters the operating room. Meticulous preoperative planning serves as the blueprint for surgical execution, minimizing intraoperative surprises, reducing tourniquet time, and ensuring the availability of all necessary instrumentation and implants.

Clinical Evaluation and Advanced Imaging
A rigorous, systematic clinical assessment is the first step in preoperative planning. Inspection must evaluate the hand at rest, noting the natural digital cascade, and through a full active arc of motion. The surgeon must critically assess for any deviation of the nail beds during flexion, the hallmark of rotational malalignment. Palpation should trace the dorsal contour of the metacarpals to identify fracture step-offs, while simultaneous volar palpation assesses for symptomatic metacarpal head prominence. The surgeon must maintain a high index of suspicion for associated injuries, meticulously examining the skin for subtle puncture wounds over the MCP joints that signify a human tooth strike, and evaluating the CMC joints for subtle subluxations that frequently accompany basilar fractures.
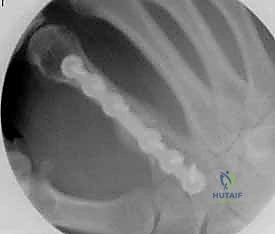
Standard radiographic imaging forms the cornerstone of diagnostic evaluation, requiring, at minimum, a dedicated posteroanterior (PA), a true lateral, and a pronated oblique view of the injured hand. The PA view is excellent for assessing coronal plane angulation and transverse displacement, though it notoriously underestimates sagittal plane deformity. The true lateral view is critical for quantifying apex-dorsal angulation, though overlapping metacarpal shadows can complicate interpretation. The pronated oblique view often provides the clearest visualization of the fracture profile and the degree of comminution.

When standard radiographs are equivocal, or when dealing with complex intra-articular fractures and suspected CMC fracture-dislocations, advanced cross-sectional imaging is mandatory. High-resolution Computed Tomography (CT) with 3D reconstructions provides unparalleled detail of articular step-offs, occult comminution, and the precise spatial orientation of fracture fragments. This information is invaluable for determining the feasibility of lag screw fixation versus the necessity of bridge plating. Furthermore, obtaining radiographs of the uninjured, contralateral hand serves as a vital anatomical template, allowing the surgeon to accurately gauge the patient's native metacarpal length and intrinsic diaphyseal curvature.
Surgical Templating and Implant Selection
With high-quality imaging in hand, the surgeon must engage in precise surgical templating. This involves selecting the optimal fixation modality—be it Kirschner wires, lag screws, dorsal plates, or intramedullary headless screws—based on the fracture's personality. For a long, oblique diaphyseal fracture where the fracture length is at least twice the diameter of the bone, interfragmentary lag screw fixation alone may provide sufficient stability. Conversely, a comminuted, unstable midshaft fracture with bone loss will necessitate a rigid dorsal locking plate utilized in a bridging construct.

Implant sizing must be anticipated. Metacarpal plates are typically low-profile (1.2mm to 1.5mm thickness) to minimize extensor tendon irritation, utilizing 2.0mm or 2.4mm screws. The surgeon must template the plate length to ensure at least three cortices of fixation (ideally four to six) proximal and distal to the fracture zone. If intramedullary fixation is chosen, the canal diameter must be measured to select an appropriately sized headless compression screw (typically 3.0mm to 4.5mm) that will achieve adequate cortical purchase without causing iatrogenic bursting of the narrow diaphysis.
Anesthesia, Positioning, and Tourniquet Application
The choice of anesthesia is a collaborative decision between the surgeon, the anesthesiologist, and the patient. Regional anesthesia, specifically an ultrasound-guided supraclavicular or axillary brachial plexus block, is highly favored. It provides excellent intraoperative muscle relaxation, profound postoperative analgesia, and facilitates a smooth emergence without the systemic side effects of general anesthesia. General anesthesia remains a viable alternative for highly anxious patients, prolonged multi-digit reconstructions, or when harvesting autologous bone graft from distant sites (e.g., iliac crest) is anticipated.

Patient positioning must optimize surgical ergonomics and fluoroscopic access. The patient is positioned supine with the operative extremity extended onto a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. Prior to inflation, the limb is strictly exsanguinated using an Esmarch bandage to ensure a completely bloodless surgical field, which is absolutely critical for the safe identification of delicate dorsal sensory nerves and the precise execution of osteosynthesis. The C-arm fluoroscopy unit is positioned perpendicular to the hand table, allowing the surgeon to obtain orthogonal views seamlessly throughout the procedure without manipulating the surgical field or compromising sterility.
Step-by-Step Surgical Approach and Fixation Technique
The execution of metacarpal fixation demands a meticulous, tissue-respecting technique. The specific approach and fixation construct are dictated by the fracture pattern, but the overarching principles of anatomical reduction, stable fixation, and soft-tissue preservation remain constant.
Percutaneous and Intramedullary Techniques
For transverse or short oblique fractures of the metacarpal neck and shaft, particularly in the fifth metacarpal, percutaneous or minimally invasive intramedullary techniques offer excellent stability while sparing the dorsal soft-tissue envelope. The procedure begins with a closed reduction utilizing the Jahss maneuver: the MCP and PIP joints are flexed to 90 degrees, relaxing the intrinsic muscles and tightening the collateral ligaments, allowing the proximal phalanx to be used as a lever to push the metacarpal head dorsally, correcting the apex-dorsal angulation.

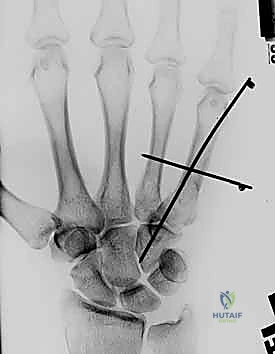
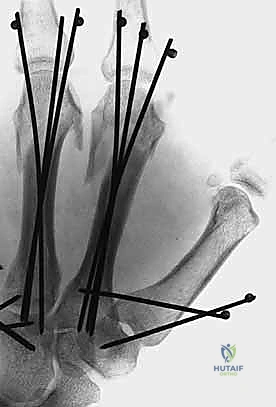
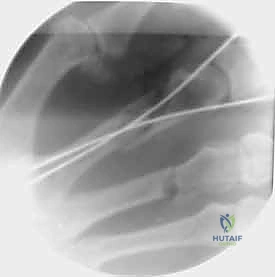
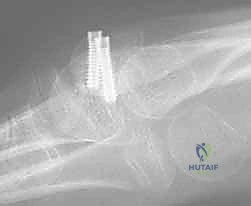
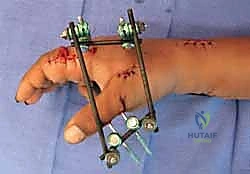
Once reduced, fixation can be achieved via crossed Kirschner wires or retrograde intramedullary pinning (the "bouquet" technique). However, the modern gold standard for minimally invasive fixation is the retrograde intramedullary headless compression screw. A small stab incision is made over the dorsal aspect of the flexed MCP joint. The entry portal is meticulously established in the articular "safe zone" of the metacarpal head—specifically the dorsal-ulnar or dorsal-radial collateral recess, strictly avoiding the central weight-bearing articular cartilage.
A guidewire is advanced down the medullary canal across the fracture site under fluoroscopic guidance. After confirming perfect rotational alignment and length, the canal is sequentially broached or drilled, and an appropriately sized headless compression screw is buried beneath the articular cartilage. This technique provides robust, load-sharing stability that allows for immediate, unrestricted active range of motion, vastly reducing the incidence of postoperative stiffness compared to traditional K-wire constructs.
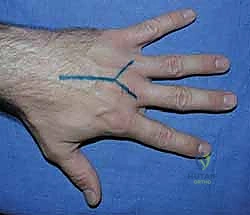
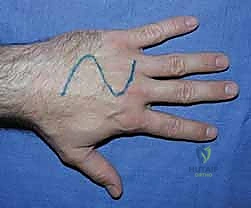
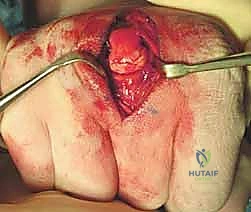
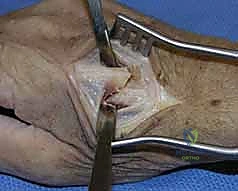
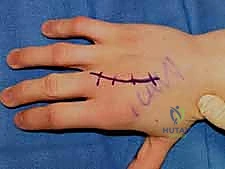
Open Reduction and Internal Fixation (ORIF) Approaches
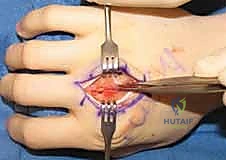
When closed reduction fails, or for complex, comminuted, or multiple metacarpal fractures, Open Reduction and Internal Fixation (ORIF) is mandated. A dorsal longitudinal or slightly gently curved incision is made centered over the fractured metacarpal. Careful subcutaneous dissection is performed to identify and meticulously retract the dorsal sensory nerve branches using vessel loops. The extensor apparatus is exposed. Depending on the fracture location, the extensor tendon can be retracted laterally, or the extensor mechanism can be split longitudinally (e.g., splitting the EDC tendon) to access the dorsal periosteum.

Periosteal elevation must be judicious and strictly limited to the footprint required for plate application. Circumferential stripping of the periosteum is a catastrophic error that devascularizes the bone fragments and invites nonunion. The fracture site is gently debrided of hematoma and interposed soft tissue. Anatomical reduction is achieved using specialized reduction forceps, taking immense care to avoid crushing fragile cortical edges. Provisional fixation is maintained with fine (0.035-inch or 0.045-inch) K-wires.
Plate and Screw Fixation Execution
The application of hardware must adhere to strict biomechanical principles. For long oblique fractures, interfragmentary lag screws are the most biomechanically efficient method of achieving absolute stability. The technique requires drilling a gliding hole (e.g., 2.0mm or 2.4mm) in the near cortex, followed by a smaller thread hole (e.g., 1.5mm or 1.8mm) in the far cortex, utilizing a specialized drill guide. The near cortex is countersunk to prevent the screw head from acting as a stress riser or irritating the overlying tendon. As the screw is tightened, the fracture fragments are dynamically compressed together.

When a dorsal plate is required, it must be meticulously contoured to match the natural dorsal convexity of the metacarpal to prevent secondary displacement during screw insertion. For transverse fractures, the plate is applied in compression mode using eccentrically placed screws. For comminuted fractures, the plate functions as a bridge, bypassing the zone of comminution to maintain length and alignment without disturbing the fracture hematoma. Locking screws are utilized in osteoporotic bone or very short distal segments to prevent hardware pullout.
Following definitive fixation, a rigorous fluoroscopic check is performed in multiple planes to confirm anatomical reduction, appropriate hardware placement, and crucially, to ensure no screws are penetrating the volar cortex excessively, which could tether the underlying flexor tendons. The tourniquet is deflated, meticulous hemostasis is achieved, and the extensor mechanism is meticulously repaired with fine absorbable sutures. The skin is closed without tension, and a bulky, well-padded dressing is applied, splinting the hand in the intrinsic-plus position.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, operative management of metacarpal fractures carries a distinct profile of potential complications. The surgeon must be acutely aware of these pitfalls, actively working to prevent them, and possessing the requisite skills to manage them when they arise. The most ubiquitous and functionally devastating complication following hand trauma and surgery is postoperative stiffness.
Stiffness primarily arises from two distinct pathophysiological processes: extensor tendon adhesions and MCP joint capsular contracture. The dorsal placement of hardware places it in intimate contact with the gliding extensor apparatus. Low-profile plates mitigate this, but any prominent screw head or excessively thick plate can cause mechanical friction, leading to tenosynovitis, profound adhesions, and ultimately, a severe extensor lag. Furthermore, prolonged immobilization or failure to splint the MCP joints in 70 to 90 degrees of flexion allows the proper collateral ligaments to fibrose in a shortened state, resulting in intractable extension contractures.

Malunion and nonunion represent failures of mechanical stability or biological healing. Rotational malunion, as previously emphasized, is entirely unacceptable and requires complex salvage via a corrective derotational osteotomy at the metacarpal base or shaft, followed by rigid re-fixation. Nonunion is relatively rare (less than 1-2% in closed fractures) due to the robust vascularity of the hand, but its incidence rises sharply in cases of severe open
Clinical & Radiographic Imaging Archive