Proximal Ulna: Optimal Internal Fixation of Fractures
Key Takeaway
Your ultimate guide to Proximal Ulna: Optimal Internal Fixation of Fractures starts here. Olecranon fractures are common, typically displaced injuries of the elbow resulting from direct trauma or falls, almost always requiring operative treatment to ensure proper alignment and function. Internal fixation of fractures is crucial for stabilizing these and other proximal ulna fractures, such as Monteggia lesions involving proximal radioulnar joint dislocation, to restore stability and prevent long-term complications.
Introduction and Epidemiology
Fracture of the olecranon process and proximal ulna represents a common orthopedic injury, constituting approximately ten percent of all upper extremity fractures. These injuries are usually displaced due to the unopposed pull of the triceps brachii and are nearly always treated operatively to restore the extensor mechanism and articular congruity. Important injury characteristics include displacement, comminution, and subluxation or dislocation of the elbow joint.

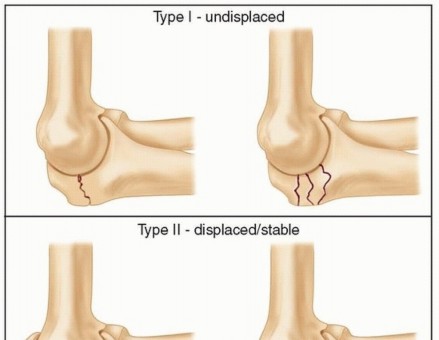
The Mayo classification is the most widely utilized system for olecranon fractures, accounting for factors that directly influence treatment decisions. Type I fractures are undisplaced, Type II are displaced but stable, and Type III are displaced and unstable (associated with subluxation or dislocation). Each type is further subdivided into A (non-comminuted) and B (comminuted).

Fracture-dislocations of the proximal ulna can be anterior (transolecranon) or posterior. The eponym Monteggia is best applied to metaphyseal or diaphyseal proximal ulnar fractures associated with dislocation of the proximal radioulnar joint (PRUJ). The Bado classification categorizes these lesions based on the direction of radial head dislocation. Type I involves anterior dislocation of the radial head with anterior angulation of the ulnar fracture. Type II involves posterior dislocation, Type III involves lateral dislocation, and Type IV involves fractures of both the radius and ulna with anterior radial head dislocation.

The Jupiter subclassification of Bado Type II fractures further delineates these complex posterior lesions based on the location of the ulnar fracture (IIa involves the coronoid and olecranon, IIb is metaphyseal-diaphyseal, IIc is diaphyseal, and IId extends along the proximal half of the ulna). Equivalent injuries in adults present variable pathology that is felt to be equivalent to injuries classified by the Bado system, though they do not always have a concomitant radiocapitellar dislocation.

Epidemiologically, proximal ulna fractures demonstrate a bimodal distribution. High-energy trauma, such as motor vehicle collisions and sports injuries, typically affects younger populations, resulting in comminuted fractures or complex fracture-dislocations. Conversely, low-energy falls from a standing height predominantly affect the elderly, osteoporotic population, frequently resulting in simple, transverse, or oblique fracture patterns.

Surgical Anatomy and Biomechanics
The proximal ulna is a complex osseous structure integral to the stability and kinematic function of the elbow. The greater sigmoid notch of the ulna is formed by the coronoid and olecranon processes, creating a nearly 180-degree articular arc that perfectly captures the trochlea of the distal humerus. This highly congruent ulnohumeral articulation is the primary stabilizer against anteroposterior translation of the elbow.

The region between the coronoid and olecranon articular facets is the nonarticular transverse groove of the olecranon, often referred to as the "bare area." This is a structurally weaker zone, making it a common location for transverse fractures. Because it is devoid of hyaline cartilage, precise articular reduction at this specific groove is not strictly critical, though overall anatomic alignment of the greater sigmoid notch remains paramount to prevent post-traumatic arthrosis.

The triceps brachii has a broad, thick, and confluent insertion from just superior to the point of the olecranon down to the tip of the olecranon process. This robust tendinous insertion can be utilized to enhance the fixation of small, osteoporotic, or severely fragmented proximal fractures. During surgical approaches, the triceps tendon can be split longitudinally or elevated to facilitate the application of dorsal plates. The pull of the triceps is the primary deforming force in olecranon fractures, necessitating fixation constructs that can withstand significant tensile loads.

The radioulnar articulation is stabilized by a triad of structures. Distally, it is supported by the triangular fibrocartilage complex (TFCC) at the distal radioulnar joint. Centrally, the interosseous ligament provides longitudinal stability in the midforearm. Proximally, the annular ligament stabilizes the proximal radioulnar joint (PRUJ). Fracture of the ulna with dislocation of the PRUJ disrupts the annular ligament, but typically, the central and distal structures are spared unless longitudinal radioulnar dissociation (Essex-Lopresti lesion) occurs. In a true Monteggia lesion, the radial head dislocates from the PRUJ, requiring anatomic restoration of ulnar length and alignment to indirectly reduce the radiocapitellar joint.

Biomechanically, the proximal ulna is subjected to immense tensile forces on its dorsal surface during active elbow extension, while the volar articular surface experiences compressive loads. This biomechanical environment makes the proximal ulna an ideal candidate for tension band principles, where a dorsally applied implant (wire or plate) converts tensile distraction forces into articular compression forces during early active motion.
Indications and Contraindications
The decision-making process for managing proximal ulna fractures relies heavily on the degree of displacement, the integrity of the extensor mechanism, patient demands, and bone quality. Stable, nondisplaced, or minimally displaced olecranon fractures are uncommon. The vast majority of olecranon fractures are displaced and benefit from operative treatment. The occasional untreated displaced simple olecranon fracture in a low-demand patient may demonstrate a slight flexion contracture and weakness of extension, but often results in minimal pain and functional limitation.

| Clinical Scenario | Management Strategy | Rationale and Considerations |
|---|---|---|
| Undisplaced Fracture (<2mm) | Non-Operative | Intact extensor mechanism. Immobilization in 45-90 degrees of flexion for 3-4 weeks, followed by progressive ROM. |
| Elderly, Low-Demand, High Surgical Risk | Non-Operative | Accept nonunion. Focus on pain control and early motion. Often yields acceptable functional results despite extensor lag. |
| Displaced Simple Transverse Fracture | Operative (Tension Band Wiring) | Restoration of extensor mechanism. Converts dorsal tension to articular compression. Ideal for non-comminuted patterns. |
| Comminuted or Oblique Fractures | Operative (Plate Osteosynthesis) | Tension band wiring will fail in comminution (causes shortening/articular step-off). Plate acts as a neutralization or buttress construct. |
| Monteggia Fracture-Dislocations | Operative (Plate Osteosynthesis) | Requires rigid restoration of ulnar length and alignment to maintain radial head reduction. |
| Fracture with Coronoid Involvement | Operative (Plate Osteosynthesis) | Coronoid is critical for anterior stability. Requires rigid fixation, often with specialized plates or anterior-to-posterior screws. |
Contraindications to surgical intervention include active local soft tissue infection (e.g., infected olecranon bursitis), severe medical comorbidities precluding anesthesia, and non-ambulatory patients with minimal upper extremity demands where the risks of surgery outweigh the functional benefits of an intact extensor mechanism.

Pre Operative Planning and Patient Positioning
Thorough preoperative planning is essential for achieving optimal outcomes in proximal ulna fixation. Standard radiographic evaluation must include true anteroposterior (AP) and lateral views of the elbow, as well as full-length orthogonal views of the forearm to rule out distal radioulnar joint disruption or associated diaphyseal injuries. The lateral radiograph is critical for assessing the extent of articular displacement, comminution, and the presence of coronoid fractures.

For complex fracture patterns, particularly Monteggia lesions, transolecranon fracture-dislocations, or cases with suspected coronoid involvement, a computed tomography (CT) scan with 3D reconstructions is highly recommended. CT imaging allows for precise characterization of articular fragmentation, preoperative templating of plate positioning, and identification of marginal impaction that may require bone grafting.

Patient positioning depends on surgeon preference, the specific fracture pattern, and the need for concomitant procedures. The two most common positions are the lateral decubitus position and the supine position.
In the lateral decubitus position, the operative arm is draped over a radiolucent post or positioned on a padded Mayo stand. This setup allows for excellent exposure of the posterior elbow and facilitates gravity-assisted elbow flexion, which is advantageous for fracture reduction and intraoperative fluoroscopy.

Alternatively, the patient can be positioned supine with the arm draped across the chest. This position is particularly useful for polytrauma patients who cannot be turned laterally or when simultaneous anterior and posterior elbow access is anticipated. A sterile tourniquet is typically applied to the proximal arm to maintain a bloodless surgical field. Intraoperative fluoroscopy must be positioned to allow unhindered orthogonal views throughout the procedure.

Detailed Surgical Approach and Technique
Posterior Surgical Approach
The posterior approach to the elbow provides universal access to the proximal ulna. A longitudinal incision is made over the posterior aspect of the elbow, typically curving slightly laterally around the tip of the olecranon to avoid placing the surgical scar directly over the olecranon bursa and the bony prominence, which can lead to painful postoperative hardware prominence and wound breakdown.

Full-thickness fasciocutaneous flaps are elevated to preserve the tenuous vascular supply to the skin. The ulnar nerve must be identified and protected medially, particularly in complex fractures extending into the diaphysis or when applying medial-based plates. Routine transposition of the ulnar nerve is not required unless there is preoperative neuropathy, the nerve is subluxating, or the hardware placement directly impinges upon the cubital tunnel.

The fracture site is exposed by incising the triceps fascia and periosteum. Hematoma and debris are meticulously cleared from the greater sigmoid notch. The articular surface must be visualized; this can often be achieved by supinating and pronating the forearm or by gently distracting the fracture fragments.
Tension Band Wiring Principles
Tension band wiring (TBW) is the gold standard for simple, transverse, non-comminuted olecranon fractures (Mayo Type IIA). The biomechanical principle relies on converting the tensile forces generated by the triceps on the dorsal cortex into compressive forces at the articular surface during elbow flexion.

The fracture is anatomically reduced and held with reduction forceps. Two parallel Kirschner wires (typically 1.6mm or 2.0mm) are introduced from the tip of the olecranon, directed distally and slightly anteriorly. Biomechanical studies suggest that transcortical K-wire placement (engaging the anterior cortex of the ulna distal to the coronoid) provides superior pull-out strength compared to intramedullary placement, though it carries a slight risk of neurovascular injury if over-penetrated.

A transverse drill hole is made in the ulnar diaphysis, approximately 2 to 3 centimeters distal to the fracture line. An 18-gauge or 20-gauge orthopedic wire is passed through this hole and crossed in a figure-of-eight fashion over the dorsal surface of the olecranon, passing deep to the triceps insertion. The wire is tensioned symmetrically using two knots to ensure uniform compression across the fracture site. The proximal K-wires are bent, cut short, and impacted deep into the triceps tendon to minimize postoperative prominence.

Plate Osteosynthesis Strategies
Plate osteosynthesis is indicated for comminuted fractures (Mayo Type IIB, IIIB), oblique fractures where a tension band would cause shearing, fractures extending distal to the coronoid, and all Monteggia fracture-dislocations.

Pre-contoured proximal ulna locking plates are typically applied to the dorsal surface of the ulna. The triceps tendon can be split longitudinally to allow the plate to sit flush against the proximal pole of the olecranon. In cases of severe proximal comminution, an intramedullary "home run" screw can be directed from the proximal aspect of the plate, down the medullary canal of the ulna, providing excellent axial stability.

For fractures involving the coronoid process, specific attention must be paid to capturing this critical anterior stabilizer. This may require the use of lateral or medial specific plates, or the placement of anterior-to-posterior lag screws. In highly comminuted transolecranon fracture-dislocations, the primary goal is restoring the contour of the greater sigmoid notch and the relationship between the olecranon and the coronoid.

Management of Monteggia Fracture Dislocations
The surgical management of Monteggia lesions hinges on the anatomic reduction and rigid fixation of the ulnar shaft. The Bado classification dictates the approach. For anterior Monteggia lesions (Bado I), dorsal plating of the ulna typically restores length and alignment, which indirectly reduces the radial head. If the radial head remains subluxated after rigid ulnar fixation, the surgeon must suspect soft tissue interposition (e.g., annular ligament or capsule) within the radiocapitellar joint, necessitating an open reduction of the PRUJ.

Posterior Monteggia lesions (Bado II) are notoriously complex and are prone to failure if not managed aggressively. The Jupiter subclassification guides fixation. These fractures often feature significant comminution of the dorsal ulnar cortex and marginal impaction of the radiocapitellar joint. Rigid dorsal plating, often supplemented with lag screws and bone grafting, is mandatory. The radial head frequently requires separate fixation or arthroplasty if severely comminuted.

Complications and Management
Despite meticulous surgical technique, complications following internal fixation of the proximal ulna are common, largely due to the subcutaneous nature of the bone and the complex biomechanics of the elbow joint.
| Complication | Estimated Incidence | Etiology and Salvage Strategy |
|---|---|---|
| Symptomatic Hardware Prominence | 40% - 80% (TBW) 10% - 20% (Plating) |
The most frequent complication. K-wires back out or knots irritate the bursa. Management consists of hardware removal after radiographic union (typically > |
Clinical & Radiographic Imaging
