Mastering Percutaneous K-Wire Fixation for Distal Radius Fractures: An Intraoperative Guide

Key Takeaway
This comprehensive masterclass guides fellows through percutaneous K-wire fixation for distal radius fractures. We cover essential anatomy, detailed preoperative planning, and step-by-step intraoperative execution of Kapandji and alternative techniques. Learn critical pearls for nerve protection, reduction, and hardware placement, along with managing potential pitfalls and ensuring optimal postoperative recovery.
Comprehensive Introduction and Patho-Epidemiology
Welcome to the operating theater, colleagues. Today, we are undertaking a meticulous exploration of one of the most ubiquitous yet deceptively nuanced injuries encountered in orthopedic traumatology: the distal radius fracture. While the advent of volar locking plate technology has revolutionized the management of these injuries over the past two decades, percutaneous Kirschner wire (K-wire) fixation remains an absolutely indispensable technique in the armamentarium of the modern orthopedic surgeon. Whether utilized as a standalone modality for extra-articular or simple intra-articular fractures, or deployed as a crucial adjunct to external fixation and spanning constructs, K-wire fixation demands a rigorous understanding of three-dimensional carpal kinematics and precise spatial awareness.
The epidemiology of distal radius fractures demonstrates a classic bimodal distribution. In the younger, high-energy trauma demographic, these fractures often present with significant comminution, profound soft tissue compromise, and severe intra-articular disruption resulting from axial loading and sheer forces. Conversely, the elderly, osteopenic population typically sustains these injuries via low-energy mechanisms, such as a fall on an outstretched hand (FOOSH). In this latter group, the metaphyseal bone yields under bending moments, frequently resulting in dorsal angulation, dorsal displacement, and radial shortening—the classic Colles-type deformity. Understanding the distinct patho-mechanical forces at play in these two demographics is the first step in formulating a rational, patient-specific surgical plan.
The enduring relevance of percutaneous K-wire fixation lies in its adherence to the principles of biological osteosynthesis. By avoiding extensive surgical exposures, periosteal stripping, and the placement of bulky hardware beneath the fragile flexor or extensor tendon compartments, we preserve the fracture hematoma and optimize the local vascular environment for secondary bone healing. Furthermore, in the setting of severe soft tissue compromise, open fractures, or polytrauma (Damage Control Orthopedics), percutaneous pinning offers a rapid, definitive, or provisional means of stabilizing the skeletal architecture while minimizing additional iatrogenic trauma.
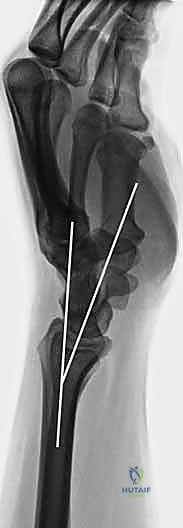
Our ultimate surgical objective, regardless of the chosen fixation modality, is the restoration of native distal radius anatomy to optimize functional outcomes and mitigate the risk of post-traumatic osteoarthritis. This requires the meticulous restoration of articular congruity (tolerating no more than 1 to 2 millimeters of step-off), the re-establishment of radial inclination (normally averaging 22 degrees), the correction of volar tilt (normally averaging 11 degrees), and the normalization of ulnar variance. Achieving these parameters percutaneously requires not only technical dexterity but also an intimate familiarity with the complex neurovascular and tendinous anatomy of the distal forearm.
Detailed Surgical Anatomy and Biomechanics
Before a single incision is made or a wire driver is engaged, we must cognitively map the critical anatomy of the distal forearm and wrist. This region represents a highly congested, complex interplay of tendons, nerves, and vessels that must be respected and protected throughout the percutaneous pinning process. The distal radius itself is a complex architectural structure, expanding from the dense diaphyseal cortical bone into a broad, cancellous metaphyseal flare that supports three distinct articular facets: the scaphoid fossa, the lunate fossa, and the sigmoid notch.
Neurovascular Structures at Risk
The primary neurovascular structure at risk during radial-sided percutaneous pinning is the Distal Radial Sensory Nerve (DRSN). The terminal branches of the radial sensory nerve emerge from beneath the brachioradialis tendon approximately 9 centimeters proximal to the radial styloid. They then fan out superficially in the subcutaneous tissues over the radial aspect of the distal radius, lying directly in the path of standard radial styloid K-wire trajectories.
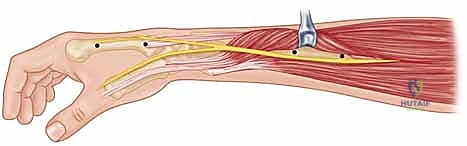
It is a non-negotiable clinical mandate to anticipate the presence of these nerve branches. Blind percutaneous drilling in this region is strictly contraindicated. A meticulous approach utilizing a longitudinal stab incision, followed by blunt dissection down to the bony cortex using fine hemostats, is required to create a safe soft-tissue corridor. Iatrogenic injury to the DRSN, whether through direct transection, thermal necrosis from the drill, or tethering by the K-wire, frequently results in debilitating neuromas or persistent dysesthesias, which can severely compromise an otherwise radiographically perfect surgical outcome.
Furthermore, the Lateral Antebrachial Cutaneous Nerve, while less frequently discussed, possesses terminal branches that lie superficial to the forearm fascia at the radial wrist and can also be inadvertently injured. On the volar aspect, the median nerve must be carefully monitored. While not directly in the trajectory of standard dorsal or radial K-wires, acute carpal tunnel syndrome is a well-documented complication of distal radius fractures, driven by fracture hematoma, significant volar displacement, or aggressive reduction maneuvers. Continuous assessment of median nerve function and a low threshold for prophylactic or therapeutic carpal tunnel release are essential components of comprehensive management.
Muscular Intervals and Tendon Compartments
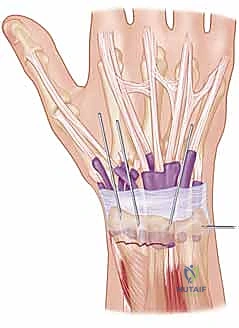
The dorsal aspect of the wrist is meticulously organized into six distinct extensor compartments, separated by septa from the extensor retinaculum. Safe percutaneous pinning relies on utilizing specific internervous and intertendinous intervals. The first dorsal compartment (containing the abductor pollicis longus and extensor pollicis brevis) and the second dorsal compartment (containing the extensor carpi radialis longus and brevis) are critical landmarks.
Importantly, there exists a relatively avascular and tendon-free "bare spot" of bone located between the first and second dorsal compartments in the region of the radial styloid. This bare spot serves as the optimal entry portal for radial K-wires, minimizing the risk of tendon irritation or subsequent rupture. Moving ulnarly, Lister's tubercle acts as a primary pulley for the extensor pollicis longus (EPL) tendon within the third dorsal compartment. Pin placement in the vicinity of Lister's tubercle must be executed with extreme caution, as the EPL is highly susceptible to attrition and delayed rupture if it continuously rubs against a prominent K-wire.
Ligamentous Anatomy and the Principle of Ligamentotaxis
The stability of the carpus and the distal radius is heavily reliant on a robust complex of extrinsic and intrinsic ligaments. The volar radiocarpal ligaments, specifically the radioscaphocapitate, long radiolunate, and short radiolunate ligaments, are particularly stout. These ligaments form the biomechanical foundation for the concept of "ligamentotaxis."
During closed reduction, the application of longitudinal traction utilizes these intact volar ligaments to transmit tension to the distal fracture fragments. This tension effectively pulls the displaced fragments out of their impacted, shortened positions and helps realign them with the intact radial diaphysis. Understanding ligamentotaxis is crucial; it explains why traction alone can often restore radial length and inclination, although it is frequently insufficient to fully correct dorsal tilt without the addition of a palmar-directed translation force.
Exhaustive Indications and Contraindications
The decision to employ percutaneous K-wire fixation must be predicated on a careful analysis of the fracture morphology, the patient's physiological bone quality, and their functional demands. While versatile, K-wire fixation is not a panacea and possesses distinct biomechanical limitations that must be respected to avoid catastrophic loss of reduction.
K-wire fixation is most ideally suited for extra-articular fractures (AO Type A) or simple intra-articular fractures (AO Type C1) that exhibit minimal comminution and occur in patients with robust bone mineral density. In these scenarios, the K-wires function effectively to hold the reduced fragments in place, acting as internal splints while secondary bone healing occurs. Furthermore, in the pediatric population, smooth K-wires are the gold standard for stabilizing displaced physeal fractures of the distal radius, as they can cross the growth plate without causing premature physeal closure or growth arrest.
Conversely, significant comminution, particularly involving the volar cortex, represents a major contraindication to standalone K-wire fixation. K-wires lack the structural rigidity to buttress against axial collapse in the absence of intact cortical contact. Similarly, volar shear fractures (Barton's fractures) are inherently unstable and have a high propensity to displace volarly along with the carpus; these injuries almost universally mandate open reduction and stable internal fixation with a volar buttress plate.
| Parameter | Indications for K-Wire Fixation | Contraindications for Standalone K-Wires |
|---|---|---|
| Fracture Pattern | Extra-articular (AO Type A), Simple Intra-articular (AO Type C1) | Volar shear (Barton's), Complex multi-fragmentary intra-articular (AO Type C3) |
| Bone Quality | Good bone stock (typically younger patients) | Severe osteoporosis (high risk of wire cut-out and axial collapse) |
| Comminution | Minimal to moderate (intact volar cortical hinge) | Extensive metaphyseal comminution, loss of volar cortical support |
| Pediatric Use | Displaced physeal fractures (Salter-Harris I, II) | N/A (Highly indicated in pediatrics) |
| Soft Tissue Status | Severe soft tissue injury precluding open approaches | Massive open wounds requiring rigid spanning external fixation |
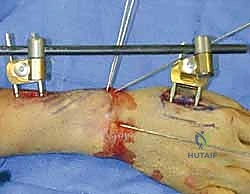
When facing a fracture with significant comminution or osteopenic bone where K-wires alone are deemed insufficient, the surgeon must be prepared to augment the construct. This is most commonly achieved by combining percutaneous pinning with a bridging external fixator. The external fixator neutralizes axial loading and bending forces, maintaining radial length through ligamentotaxis, while the K-wires are utilized to fine-tune and stabilize specific articular fragments or correct residual dorsal tilt.
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the blueprint for intraoperative success. It begins with a comprehensive clinical evaluation, assessing not only the osseous deformity but also the integrity of the soft tissue envelope and the neurovascular status of the extremity. A thorough physical examination must document two-point discrimination in the median and ulnar nerve distributions, as well as the active function of all digital flexors and extensors, establishing a baseline prior to any intervention.
Radiographic evaluation is paramount. Standard posteroanterior (PA), lateral, and oblique radiographs provide the foundational understanding of the fracture geometry. On the PA view, we meticulously measure radial inclination and ulnar variance. On the lateral view, we assess the degree of dorsal or volar tilt and the extent of dorsal comminution. In complex intra-articular fractures, a non-contrast Computed Tomography (CT) scan is highly recommended. A CT scan, particularly with 3D reconstructions, provides invaluable insight into the exact location and size of articular step-offs, the presence of a "die-punch" fragment, and the integrity of the sigmoid notch, allowing the surgeon to mentally template the exact trajectory required for each K-wire.

Patient positioning and operating room setup must be optimized to facilitate unhindered access and flawless fluoroscopic imaging. The patient is positioned supine with the affected extremity extended onto a radiolucent hand table. It is critical to ensure that the C-arm can easily arc 90 degrees to provide perfect orthogonal PA and lateral views without requiring the surgeon to awkwardly manipulate the fracture site.
A sterile pneumatic tourniquet is applied to the proximal arm. While some surgeons prefer to perform percutaneous pinning without a tourniquet to avoid ischemic pain, utilizing a tourniquet after thorough exsanguination provides a bloodless field. This is particularly advantageous when making the small stab incisions and performing the blunt dissection necessary to protect the dorsal sensory branches of the radial nerve. The entire upper extremity is prepped and draped in a standard sterile fashion, allowing for full manipulation of the elbow, wrist, and digits.
Step-by-Step Surgical Approach and Fixation Technique
With the patient prepped, the tourniquet inflated, and the fluoroscopy unit positioned, we commence the operative intervention. The foundation of successful K-wire fixation relies entirely on achieving an anatomical closed reduction prior to the introduction of any hardware.
The Closed Reduction Maneuver
We begin by applying sustained longitudinal traction to the digits, utilizing either sterile finger traps or manual traction provided by an assistant, while counter-traction is applied proximal to the elbow. This traction harnesses the power of ligamentotaxis to disimpact the fracture fragments and restore radial length.

Crucially, to correct the typical dorsal angulation, we place a tightly rolled, padded bump transversely beneath the volar aspect of the distal forearm, directly proximal to the fracture line. This bump acts as a mechanical fulcrum. By applying a volarly directed force to the distal carpal row and the distal radial fragment, while simultaneously flexing the wrist over the fulcrum, we can effectively lever the distal fragment out of dorsal extension and restore the native volar tilt.
Once the reduction maneuver is complete, it is provisionally held in place by the assistant while we bring in the C-arm to verify our parameters. We must confirm the restoration of radial length, inclination, and volar tilt on orthogonal views.



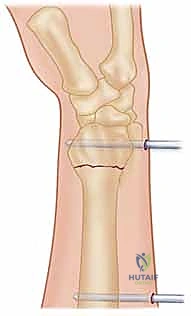
Radial Styloid Pinning
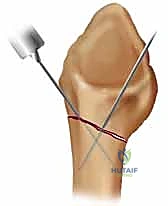
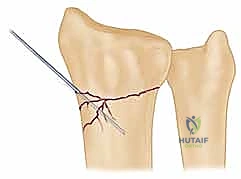
With a satisfactory reduction confirmed, we proceed to secure the radial column. We typically utilize 0.062-inch (1.6 mm) or 0.045-inch (1.1 mm) smooth K-wires. The entry point is the "bare spot" on the radial styloid, between the first and second dorsal compartments.



A 1 cm longitudinal stab incision is made through the skin only. Using a fine hemostat, we bluntly dissect down to the bone, carefully spreading parallel to the anticipated course of the DRSN branches. A tissue protector or drill guide is inserted down to the bone to prevent the wire from winding up soft tissues. The first wire is driven from the radial styloid, directed proximally, ulnarly, and slightly dorsally, aiming to cross the fracture site and engage the dense cortical bone of the proximal ulnar diaphysis of the radius.



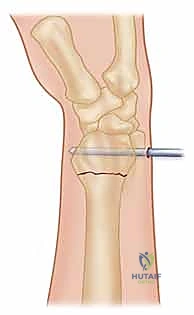
Dorsal Ulnar and Intrafocal Pinning
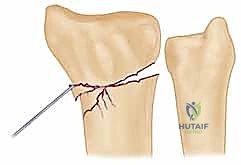
Depending on the fracture configuration, a second or third wire is required to provide rotational stability and support the lunate fossa. This can be achieved via a crossed-pin configuration, driving a wire from the dorsal-ulnar corner of the distal radius (between the 4th and 5th compartments) directing it proximally and radially.


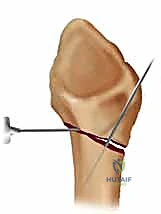
Alternatively, the Kapandji intrafocal pinning technique is highly effective for buttressing dorsal comminution. In this technique, K-wires are introduced directly into the fracture line dorsally. Once the wire engages the volar cortex of the proximal fragment, it is levered distally, effectively pushing the distal fragment into volar flexion to restore tilt. The wire is then driven across the volar cortex to lock the reduction in place.



Final Assessment and Wire Management
Following the placement of all planned K-wires, a meticulous final fluoroscopic assessment is mandatory. We must scrutinize the PA, lateral, and oblique views to ensure anatomical reduction, confirm that no wires have inadvertently penetrated the radiocarpal or distal radioulnar joints, and verify bi-cortical purchase.



Once satisfied, the wires are managed. The decision to bury the wires beneath the skin or leave them exposed is surgeon-dependent. Burying wires theoretically reduces the risk of pin tract infections but requires a secondary minor procedure for removal. Leaving them exposed facilitates easy removal in the clinic but necessitates meticulous pin site care. If left exposed, the wires are bent at a 90-degree angle, cut short, and capped to prevent snagging and limit migration.
The procedure concludes with the application of sterile dressings and a well-padded, custom-molded short arm sugar-tong splint or a volar-dorsal bivalved cast, ensuring the wrist is immobilized in a neutral or slightly extended position to optimize functional recovery.
Complications, Incidence Rates, and Salvage Management
While percutaneous pinning is minimally invasive, it is not devoid of complications. A thorough understanding of potential pitfalls is essential for both preoperative patient counseling and prompt postoperative management.
Pin tract infection is the most frequently encountered complication, with superficial infections occurring in up to 10-15% of cases where wires are left exposed. These typically present as localized erythema and serous drainage at the pin-skin interface. The vast majority resolve rapidly with a short course of oral antibiotics (e.g., first-generation cephalosporins) and enhanced local pin site hygiene. Deep infections or
