
Introduction and Epidemiology
Distal radius fractures represent a formidable and ubiquitous challenge in orthopaedic trauma, necessitating a comprehensive understanding of osseous anatomy, wrist biomechanics, and modern fixation principles. These injuries are among the most common fractures of the upper extremity, with an estimated incidence of more than 650,000 occurring annually in the United States alone. The sheer volume of these injuries places a significant burden on the healthcare system; fractures of the distal radius represent approximately one-sixth of all fractures treated in emergency departments and account for about 16% of all fractures managed by orthopaedic surgeons.
Epidemiologically, distal radius fractures demonstrate a classic bimodal distribution. In younger demographics, these fractures are typically the result of high-energy trauma. Common mechanisms in younger individuals include falls from a height, motor vehicle accidents, or injuries sustained during athletic participation. High-energy injuries often result in significantly displaced, highly comminuted, and unstable fracture patterns with substantial articular surface involvement.
Conversely, in elderly individuals, distal radial fractures frequently arise from low-energy mechanisms, such as a simple fall from a standing height onto an outstretched hand. In this population, they are universally considered a fragility fracture. The incidence of distal radius fractures in the elderly correlates directly with osteopenia and osteoporosis, rising in incidence with increasing age, nearly in parallel with the increased incidence of proximal femur (hip) fractures.
Demographic data further highlights this disparity. In men aged 35 years and older, the incidence is approximately 90 per 100,000 population per year and remains relatively constant until the age of 70, where a slight increase is observed. However, the data for women is markedly different. In women less than age 40, the incidence is approximately 368 per 100,000 population; for women 40 years and older, this incidence rises precipitously to 1,150 per 100,000 population. Established risk factors for fractures of the distal radius in the elderly include decreased bone mineral density, female sex, white race, family history of fragility fractures, and early menopause.
Mechanism of Injury and Pathomechanics
The most common mechanism of injury across all demographics is a fall onto an outstretched hand (FOOSH) with the wrist locked in dorsiflexion. Biomechanical studies demonstrate that fractures of the distal radius are reliably produced when the dorsiflexion of the wrist varies between 40 and 90 degrees at the moment of impact.
During the loading phase of the injury, the radius initially fails in tension on the volar aspect. The fracture line then propagates dorsally. Concurrently, bending moment forces induce severe compression stresses on the dorsal cortex, resulting in characteristic dorsal comminution. Cancellous impaction of the metaphysis further compromises dorsal stability, creating a dorsal void once the fracture is reduced. Additionally, complex shearing forces influence the injury pattern, often resulting in intra-articular step-offs, gap formation, and multifragmentary articular surface involvement.
Surgical Anatomy and Biomechanics
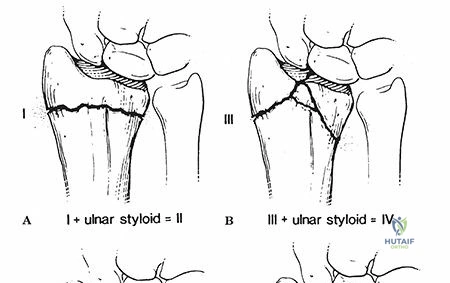
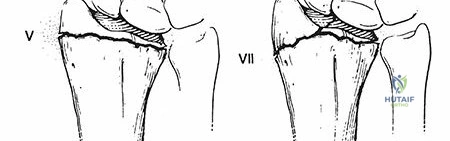
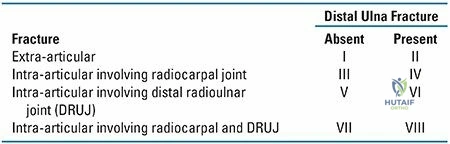
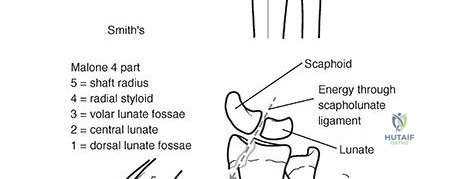
A rigorous command of distal radius anatomy is the foundation of successful surgical reconstruction. The metaphysis of the distal radius is composed primarily of cancellous bone with a relatively thin cortical shell, making it highly susceptible to impaction and comminution. The articular surface features a biconcave surface for articulation with the proximal carpal row—specifically, the scaphoid and lunate fossae—separated by the interfossal ridge. Medially, the radius features the sigmoid notch for articulation with the distal ulna, forming the distal radioulnar joint (DRUJ).
Normal Radiographic Parameters
Restoration of normal anatomy is the primary goal of operative intervention. The native distal radius exhibits the following standard radiographic parameters:
* Radial Inclination: Averages 22 to 24 degrees.
* Volar Tilt: Averages 11 to 12 degrees.
* Radial Height: Averages 11 to 12 mm.
* Ulnar Variance: Typically neutral, though it varies slightly with grip and forearm rotation.
Ligamentous Anatomy
Numerous stout ligamentous attachments exist to the distal radius. These soft tissue envelopes often remain intact during a distal radius fracture, facilitating indirect reduction techniques through the principle of “ligamentotaxis.” The volar radiocarpal ligaments (including the radioscaphocapitate, long radiolunate, and short radiolunate ligaments) are substantially stronger and confer more stability to the radiocarpal articulation than their dorsal counterparts.
The watershed line is a critical anatomic landmark on the volar distal radius. It is a transverse ridge that marks the distal margin of the pronator quadratus fossa and the proximal attachment of the volar radiocarpal ligaments. Hardware placed distal to this line significantly increases the risk of flexor tendon irritation and subsequent rupture, particularly the flexor pollicis longus (FPL).
Wrist Biomechanics and Load Transfer
In a structurally intact wrist, approximately 80 percent of the axial load is supported by the distal radius, while the remaining 20 percent is transmitted through the ulna and the triangular fibrocartilage complex (TFCC).

Alterations in the osseous anatomy drastically shift these biomechanical forces. Reversal of the normal palmar tilt (dorsal angulation) results in a pathologic load transfer onto the ulna and TFCC. The remaining load is then borne eccentrically by the distal radius and becomes highly concentrated on the dorsal aspect of the scaphoid fossa. This abnormal force distribution accelerates articular wear, decreases grip strength, restricts functional range of motion, and predisposes the patient to post-traumatic radiocarpal osteoarthritis and ulnocarpal abutment syndrome.
Indications and Contraindications
The decision algorithm for managing distal radius fractures relies heavily on fracture stability, articular congruity, patient physiologic age, and functional demands. Lafontaine’s criteria for instability (initial dorsal tilt >20 degrees, dorsal comminution, intra-articular involvement, associated ulnar fracture, and age >60 years) remain highly relevant in predicting which fractures will fail non-operative management.
Operative vs Non Operative Management Parameters
| Management Strategy | Primary Indications | Key Clinical and Radiographic Criteria |
|---|---|---|
| Non-Operative (Closed Reduction and Casting) | Stable, extra-articular fractures; Low-demand elderly patients | Radial shortening < 3mm; Dorsal tilt < 10 degrees past neutral; Intra-articular step-off < 2mm; No carpal malalignment. |
| Operative (Volar Locking Plate) | Unstable fractures failing closed reduction; Volar shear fractures (Smith/Reverse Barton) | Radial shortening > 3mm; Dorsal tilt > 10 degrees; Intra-articular step-off or gap > 2mm; Volar comminution. |
| Operative (Dorsal Plating) | Dorsal shear fractures (Barton); Complex dorsal comminution | Displaced dorsal rim fragments; Failure of volar fixed-angle constructs to capture dorsal articular fragments. |
| Operative (Fragment Specific Fixation) | Complex multi-fragmentary intra-articular fractures | Radial styloid fractures (Chauffeur); Lunate facet die-punch fragments requiring independent buttress fixation. |
| Operative (External Fixation/CRPP) | Severe soft tissue compromise; Polytrauma damage control | Open fractures with gross contamination; Highly comminuted fractures relying on ligamentotaxis. |
Contraindications to Surgical Fixation
Absolute contraindications to internal fixation include active local soft tissue infection, critically compromised soft tissue envelopes (excluding open fractures requiring stabilization), and patients who are medically unfit for anesthesia. Relative contraindications include severe baseline dementia or non-ambulatory status in elderly patients where the functional benefit of anatomic restoration is outweighed by surgical morbidity.
Pre Operative Planning and Patient Positioning
Thorough clinical and radiographic evaluation is paramount to execute an effective surgical plan.
Clinical Evaluation
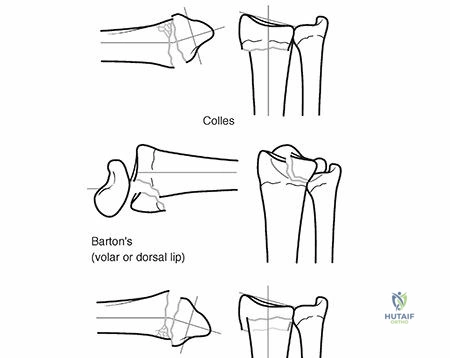
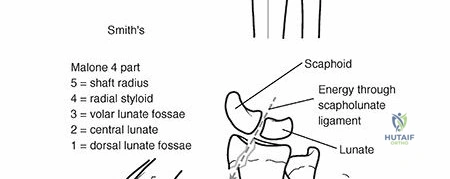
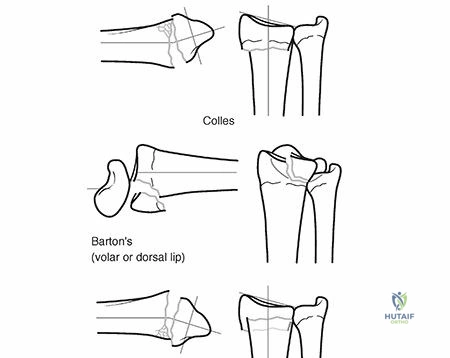
Patients typically present with variable wrist deformity and displacement of the hand in relation to the wrist. The deformity is classically dorsal in Colles or dorsal Barton fractures, and volar in Smith-type fractures or volar Bartons. The wrist is typically swollen with ecchymosis, exquisite tenderness, and painful, restricted range of motion.
The ipsilateral elbow and shoulder must be systematically examined to rule out associated injuries, such as Essex-Lopresti fracture-dislocations or concomitant radial head fractures. A careful neurovascular assessment should be performed immediately, with particular attention to median nerve function. Carpal tunnel compression symptoms are remarkably common, occurring in 13% to 23% of cases. This acute median neuropathy is typically owing to traction during forced hyperextension of the wrist, direct trauma from fracture fragments, hematoma formation within the canal, or increased volar compartment pressure.
Radiographic Evaluation
Standard posteroanterior (PA) and lateral views of the wrist are mandatory. The PA view assesses radial height, radial inclination, and ulnar variance, while the lateral view evaluates volar tilt and carpal alignment (assessing for dorsal intercalated segment instability or volar intercalated segment instability).
For intra-articular fractures, a non-contrast Computed Tomography (CT) scan is highly recommended. CT imaging provides orthogonal and 3D reconstructive views that are invaluable for identifying articular step-offs, gap formation, die-punch fragments, and the exact location of major fracture lines (e.g., separating the scaphoid and lunate facets).
Patient Positioning and Operating Room Setup
The patient is positioned supine on the operating table with the operative extremity extended onto a radiolucent hand table. A well-padded upper arm tourniquet is applied. The C-arm fluoroscopy unit is typically brought in parallel to the hand table or from the head of the bed, depending on surgeon preference and room configuration. The monitor should be placed directly across from the surgeon for optimal viewing ergonomics. Intravenous antibiotics are administered prior to tourniquet inflation.
Detailed Surgical Approach and Technique
The advent of fixed-angle volar locking plates has revolutionized the surgical management of distal radius fractures, making the volar approach the workhorse for most orthopaedic surgeons.
The Volar Approach Modified Henry
The modified Henry approach utilizes the internervous plane between the brachioradialis (innervated by the radial nerve) and the flexor carpi radialis (FCR, innervated by the median nerve).
An 8 to 10 cm longitudinal incision is made overlying the FCR tendon, extending proximally from the wrist crease. The superficial fascia is incised, and the FCR tendon sheath is opened. The FCR tendon is typically retracted ulnarly to protect the median nerve, which lies directly ulnar and deep to the FCR. Alternatively, radial retraction of the FCR can be utilized, though care must be taken to avoid traction injury to the palmar cutaneous branch of the median nerve.
Deep dissection reveals the flexor pollicis longus (FPL) muscle belly and tendon. The FPL is retracted ulnarly, exposing the pronator quadratus (PQ) muscle. The PQ is released from its radial and distal insertions leaving a small cuff of tissue for later repair, and elevated ulnarly to expose the volar radiocarpal ligaments and the volar metaphysis of the distal radius. The brachioradialis tendon insertion on the radial styloid may be fractionally lengthened or released to neutralize its deforming supinating and proximally displacing force on the radial styloid fragment.
Fracture Reduction Techniques
Anatomic reduction of the articular surface and restoration of radial length, inclination, and tilt are critical. Reduction is often achieved through longitudinal traction and ligamentotaxis. For impacted articular fragments (die-punch), a cortical window may be created in the metaphyseal defect to allow insertion of a periosteal elevator, elevating the articular fragments under fluoroscopic guidance.
Intrafocal pinning (Kapandji technique) or provisional fixation with 0.045 or 0.062-inch Kirschner wires can be utilized to hold the reduction while the plate is applied. The "volar cortical read" is a crucial concept; because the volar cortex of the radius is relatively flat and less prone to comminution than the dorsal cortex, anatomic reduction of the volar cortical line often dictates a correct reduction of the entire metaphysis.
Volar Plate Application and Fixation
Once provisional reduction is achieved, a volar locking plate is applied. The plate must be positioned proximal to the watershed line to prevent flexor tendon attrition.

The standard sequence of fixation involves placing a cortical screw in the oblong gliding hole of the proximal shaft to allow for proximal-distal adjustments. Once the plate position is optimized, distal locking screws are inserted into the subchondral bone to support the articular surface. Fluoroscopic evaluation with multi-planar views (including 20-degree elevated lateral and 10-degree tilted PA views) is mandatory to confirm that screws do not penetrate the radiocarpal or distal radioulnar joints. Dorsal cortical penetration by distal locking screws must be strictly avoided to prevent extensor tendon irritation or rupture.
Dorsal Approach and Fragment Specific Fixation
While volar plating is ubiquitous, certain fracture patterns—specifically isolated dorsal shear fractures (dorsal Barton), severe dorsal comminution not captured by volar screws, or combined radiocarpal fracture-dislocations—require a dorsal approach.
The dorsal approach typically utilizes a longitudinal incision centered over Lister's tubercle. The extensor retinaculum is incised, usually through the third dorsal compartment, transposing the extensor pollicis longus (EPL) tendon radially or ulnarly. Subperiosteal elevation of the second and fourth compartments exposes the dorsal radius. Low-profile dorsal plates are utilized to minimize extensor tendon irritation, and the extensor retinaculum is often repaired deep to the EPL to provide a soft tissue interposition layer.
Fragment-specific fixation involves the use of small, low-profile implants (pin-plates, hook plates, or wire forms) to independently address specific fracture components, such as the radial styloid, dorsal ulnar corner, or volar lunate facet, which may not be adequately stabilized by a single standard volar plate.
Complications and Management
Despite advances in implant technology and surgical technique, operative management of distal radius fractures carries a distinct complication profile. Strict adherence to anatomic landmarks and meticulous surgical technique are required to minimize these risks.
Table of Common Complications and Management Strategies
| Complication | Incidence / Risk Factors | Prevention and Management Strategy |
|---|---|---|
| Median Neuropathy (CTS) | 13-23% acute; highly associated with high-energy trauma and severe displacement. | Prophylactic carpal tunnel release is not routinely indicated unless symptoms are progressive or fail to resolve post-reduction. Acute, severe symptoms require urgent surgical decompression. |
| Extensor Pollicis Longus (EPL) Rupture | 1-5%; Associated with non-operative management (hematoma/ischemia) and prominent dorsal screws. | Meticulous fluoroscopic evaluation of screw length. Management of rupture typically involves extensor indicis proprius (EIP) to EPL tendon transfer. |
| Flexor Pollicis Longus (FPL) Rupture | 2-12% with volar plates; Caused by plate placement distal to the watershed line. | Ensure plate is seated proximal to the watershed line. If hardware prominence is noted post-operatively with tendon irritation, early hardware removal is indicated. |
| Complex Regional Pain Syndrome (CRPS) | 1-8%; Correlated with excessive traction, tight casts, and severe pain. | Early recognition, aggressive pain management, vitamin C supplementation (though controversial, some data supports 500mg daily), and immediate intensive hand therapy. |
| Malunion | Common in non-operative management of unstable fractures. | Corrective osteotomy (volar opening wedge or dorsal closing wedge) with structural bone grafting and rigid internal fixation if the patient is symptomatic. |
| Post-Traumatic Osteoarthritis | Correlates directly with residual intra-articular step-off > 2mm. | Anatomic articular reduction. Late management includes partial wrist fusion (e.g., scaphoid excision and four-corner fusion) or total wrist arthrodesis. |
Post Operative Rehabilitation Protocols
Post-operative rehabilitation is heavily dependent on the stability of the fracture fixation and bone quality. The primary goal is to prevent stiffness of the digits, wrist, elbow, and shoulder while protecting the osseous reconstruction.
Phase 1 Acute Post Operative Period Zero to Two Weeks
Immediately post-operatively, the wrist is immobilized in a bulky compressive dressing and a volar orthosis or sugar-tong splint. Strict elevation and active range of motion (ROM) of the digits, elbow, and shoulder are initiated immediately to control edema and prevent stiffness. Digital ROM is critical to prevent tendon adhesions.
Phase 2 Early Mobilization Two to Six Weeks
At the first post-operative visit (typically 10 to 14 days), sutures are removed. If rigid internal fixation with a volar locking plate was achieved, the bulky splint is transitioned to a removable custom thermoplastic wrist splint. Patients are instructed to remove the splint multiple times a day to perform active and active-assisted wrist flexion, extension, pronation, and supination. Passive stretching and forceful manipulation remain strictly contraindicated during this phase to prevent hardware failure or loss of reduction.
Phase 3 Strengthening and Maturation Six to Twelve Weeks
Radiographic evaluation at 6 weeks typically demonstrates early callus formation and obliteration of the fracture lines. At this juncture, the removable splint is discontinued. Progressive strengthening exercises, dynamic splinting (if significant stiffness persists), and passive ROM exercises are initiated. Full functional recovery, including maximum grip strength and terminal range of motion, may take up to 12 to 18 months post-injury.
Summary of Key Literature and Guidelines
The management of distal radius fractures is guided by a robust body of orthopaedic literature and clinical practice guidelines.
The American Academy of Orthopaedic Surgeons (AAOS) Clinical Practice Guidelines strongly recommend operative fixation for fractures with post-reduction radial shortening greater than 3 mm, dorsal tilt greater than 10 degrees, or intra-articular displacement or step-off greater than 2 mm. These guidelines are based on biomechanical data demonstrating exponential increases in radiocarpal contact pressures with persistent deformity.
However, the literature regarding the management of elderly patients is highly nuanced. Landmark prospective randomized controlled trials, notably by Arora et al., have demonstrated that while operative fixation (volar locking plates) in patients over the age of 65 yields superior radiographic outcomes compared to cast immobilization, there is no statistically significant difference in functional outcomes (DASH scores), grip strength, or pain levels at 12 months post-injury. This data strongly supports the use of non-operative management in low-demand elderly patients, even in the setting of radiographic malunion, to avoid the inherent surgical risks and complication profiles associated with internal fixation.
Furthermore, the concept of fracture instability, originally codified by Lafontaine, has been repeatedly validated. Surgeons must maintain a high index of suspicion for secondary displacement in non-operatively managed fractures that exhibit initial severe dorsal angulation, dorsal comminution, or occur in osteoporotic bone, necessitating close radiographic follow-up during the first three weeks of cast immobilization.
Clinical & Radiographic Imaging

Detailed Chapters & Topics
Dive deeper into specialized chapters regarding distal-radius-fractures