Mastering Distal Radius Dorsal Plate Fixation: An Intraoperative Guide

Key Takeaway
Welcome to the OR, fellows. Today, we're tackling a dorsally displaced distal radius fracture with dorsal plate fixation. We'll meticulously review surgical anatomy, patient positioning, and a granular, real-time breakdown of the incision, dissection, reduction, and hardware application. Expect critical insights into neurovascular protection, articular fragment management, and essential pearls to optimize outcomes and avoid common pitfalls.
Comprehensive Introduction and Patho-Epidemiology
Alright, fellows, gather around. Let's scrub in. Today, we are addressing a ubiquitous yet perpetually challenging orthopedic injury: a dorsally displaced, highly unstable distal radius fracture. Our primary surgical objective is precise anatomical reduction and rigid internal fixation utilizing a dorsal plate construct, thereby restoring the critical biomechanics of the radiocarpal and distal radioulnar joints. This procedure transcends the simple act of applying metal to bone; it demands a profound mastery of the intricate regional anatomy, the ability to anticipate intraoperative complexities, and the execution of each technical step with meticulous, uncompromising precision.
Distal radius fractures represent one of the most frequently encountered fractures in orthopedic trauma, accounting for up to one-sixth of all fractures treated in emergency departments. These injuries typically originate within the radial metaphysis, frequently extending intra-articularly into the radiocarpal joint and, with concerning regularity, into the distal radioulnar joint (DRUJ). The pathomorphology of these fractures spans a vast spectrum, presenting as stable or unstable, intra-articular or extra-articular, and they are often complicated by a constellation of associated osseous, ligamentous, and neurovascular injuries. The classical pattern we are confronting today—a dorsally displaced and angulated fracture—is characterized by the apex of the deformity pointing volarly, a configuration that inherently disrupts the delicate load-bearing mechanics of the wrist.
The pathogenesis of this specific fracture pattern is inextricably linked to its mechanism of injury: the classic fall on an outstretched hand (FOOSH). When the hand impacts the ground, it is typically in a position of forced extension and varying degrees of radial or ulnar deviation. The resulting force vector generates a massive axial load combined with a bending moment. When this applied kinetic energy exceeds the ultimate failure strength of the metaphyseal cortical shell and the underlying cancellous trabecular network, catastrophic structural failure occurs. The specific fracture morphology—whether it manifests as a simple transverse break, a complex multi-fragmentary comminution, or a die-punch articular depression—is directly dictated by the magnitude, velocity, and precise direction of this applied force vector, as well as the intrinsic bone mineral density of the patient.
Historically, the dorsal approach to the distal radius was fraught with significant complications, most notably extensor tendon irritation, tenosynovitis, and delayed rupture. This was largely attributable to the thick, prominent profile of early-generation implants. Consequently, the pendulum of orthopedic preference swung heavily toward volar locked plating. However, the evolution of modern osteosynthesis has yielded ultra-low-profile, anatomically contoured dorsal plates and fragment-specific fixation systems. This technological renaissance has resurrected the dorsal approach, making it an indispensable technique in the modern orthopedic surgeon's armamentarium, particularly for fractures characterized by severe dorsal comminution, displaced dorsal ulnar corner fragments, or complex intra-articular disruptions that simply cannot be adequately visualized or buttressed from a volar approach.
Detailed Surgical Anatomy and Biomechanics
Osteology and Articular Geometry
Before a scalpel even touches the skin, an absolute, three-dimensional spatial awareness of the distal radius anatomy is mandatory. The distal radius is the foundational keystone of the wrist, articulating distally with the scaphoid and lunate to form the radiocarpal joint, and proximally with the ulnar head at the sigmoid notch to constitute the DRUJ. The articular surface is biconcave, featuring a distinct scaphoid fossa and lunate fossa, separated by a subtle interfossal ridge.

We must remain acutely cognizant of our critical radiographic and anatomic parameters. Normal volar tilt averages approximately 11 degrees (range 0-22 degrees). This tilt is essential for normal kinematics; a loss of volar tilt, particularly dorsal angulation exceeding 20 degrees, shifts the physiological load-bearing axis dorsally and ulnarly, leading to accelerated radiocarpal arthrosis, profound loss of flexion, and significantly diminished grip strength. Radial height, averaging 11 mm (range 8-15 mm), and radial inclination, averaging 22 degrees (range 15-30 degrees), must be meticulously restored. Failure to restore radial length results in a positive ulnar variance, precipitating ulnar impaction syndrome and devastating disruption of the triangular fibrocartilage complex (TFCC) kinematics.
Lister's tubercle, a prominent osseous protuberance located on the dorsal aspect of the distal radius, serves as the critical anatomical lighthouse for our surgical approach. It functions as a biomechanical pulley for the extensor pollicis longus (EPL) tendon, redirecting its vector of pull toward the thumb. Identifying and protecting this structure, and understanding its relationship to the surrounding extensor compartments, is the first crucial step in navigating the dorsal wrist.
Ligamentous Stabilizers and the TFCC
The osseous architecture of the wrist is inherently unstable without the robust support of its intricate ligamentous network. While volar locked plating often avoids direct interaction with the dorsal capsuloligamentous structures, the dorsal approach requires deliberate and careful management of these tissues. The dorsal radiocarpal ligament, originating from the dorsal rim of the radius and inserting onto the triquetrum and lunate, provides critical secondary stabilization to the radiocarpal joint. During our approach, we may need to elevate this ligament as a continuous flap with the joint capsule to directly visualize and anatomically reduce impacted intra-articular fragments.
The volar extrinsic ligaments, including the radioscaphocapitate, long radiolunate, and short radiolunate ligaments, are the primary stabilizers of the carpus. While we do not directly visualize them during a dorsal approach, we must understand that severe dorsal displacement of the distal radius inherently stretches and damages these volar structures. Restoring the bony anatomy dorsally is the first step in allowing these volar ligaments to heal at their proper resting length.
Furthermore, the Triangular Fibrocartilage Complex (TFCC) is intimately associated with the distal radius. The superficial and deep fibers of the dorsal and volar radioulnar ligaments originate from the margins of the sigmoid notch and insert onto the ulnar styloid and fovea. If a fracture line propagates through the sigmoid notch, or if there is an associated ulnar styloid base fracture, the integrity of the DRUJ is compromised. Intraoperative assessment of DRUJ stability after radius fixation is an absolute requirement, not an optional afterthought.
Extensor Compartments and Retinacular Anatomy
The dorsal aspect of the wrist is organized into six distinct extensor compartments, defined by the septations of the extensor retinaculum. Intimate familiarity with this topography is non-negotiable, as our surgical dissection will proceed directly through and around these structures.
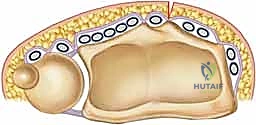
The first compartment, housing the abductor pollicis longus (APL) and extensor pollicis brevis (EPB), lies over the radial styloid. The second compartment, positioned just radial to Lister's tubercle, contains the extensor carpi radialis longus (ECRL) and brevis (ECRB). The third compartment, containing the EPL tendon, courses obliquely around Lister's tubercle. This third compartment is the primary gateway for our standard dorsal approach.
Moving ulnarly, the fourth compartment contains the extensor digitorum communis (EDC) and extensor indicis proprius (EIP). The fifth compartment, situated over the DRUJ, houses the extensor digiti minimi (EDM). Finally, the sixth compartment, located over the ulnar head, contains the extensor carpi ulnaris (ECU). During our exposure, we will meticulously elevate the second and fourth compartments subperiosteally to expose the broad dorsal metaphysis of the radius, while entirely mobilizing and protecting the EPL tendon.
Neurovascular Topography
Iatrogenic injury to the neurovascular structures of the dorsal wrist is a devastating complication that must be avoided through meticulous surgical technique. The radial sensory nerve (RSN), a branch of the superficial radial nerve, emerges from beneath the brachioradialis in the distal third of the forearm and arborizes extensively over the radial and dorsal aspects of the hand. Its branches are highly susceptible to traction injury or direct laceration during skin incision and subcutaneous dissection, particularly if the approach strays too far radially.
The posterior interosseous nerve (PIN) resides deeper within the forearm. While its main trunk is generally proximal to our standard dissection field, its terminal articular branches descend along the interosseous membrane to innervate the dorsal wrist capsule. Aggressive proximal dissection or the careless placement of retractors deep within the fourth compartment can result in neuropraxia. Furthermore, while the radial artery is primarily a volar structure, its dorsal carpal branch courses through the anatomic snuffbox; extreme vigilance is required when addressing radial styloid fragments to prevent catastrophic vascular injury.
Exhaustive Indications and Contraindications
Determining the necessity for operative intervention, and specifically selecting a dorsal approach, requires a nuanced synthesis of the patient's physiological profile, functional demands, and the specific geometric derangements of the fracture. The fundamental question is one of stability: can this fracture be reduced closed, and more importantly, will it maintain that reduction in a cast? If the answer to either is negative, surgical fixation is indicated.

The primary indication for dorsal plate osteosynthesis is a fracture pattern exhibiting severe dorsal comminution that cannot be adequately buttressed from a volar approach. When the dorsal cortex is effectively pulverized, a volar plate, even with locking screws, may fail to prevent dorsal collapse during the healing phase. Dorsal plating acts as a direct structural buttress against this specific vector of failure. Furthermore, dorsal plating is the gold standard for specific intra-articular fracture patterns, such as a dorsal Barton's fracture (a dorsal shear fracture of the articular margin) or complex die-punch fractures where the dorsal lunate facet is depressed and requires direct visualization for elevation and grafting.

Conversely, dorsal plating is generally contraindicated in the setting of volar shear fractures (volar Barton's), where the biomechanical forces dictate volar buttressing. It is also relatively contraindicated in patients with profound osteopenia or osteoporosis. In severely osteoporotic bone, the dorsal cortex is often too thin and brittle to provide adequate screw purchase, making a volar locked plate—which relies on subchondral support in the denser epiphyseal bone—a biomechanically superior choice. Active local soft tissue infection or critically compromised dorsal soft tissue envelopes are absolute contraindications to any internal fixation.
| Parameter | Indications for Dorsal Plating | Contraindications for Dorsal Plating |
|---|---|---|
| Fracture Morphology | Severe dorsal comminution (>50% shaft diameter) | Volar shear fractures (Volar Barton's) |
| Articular Involvement | Displaced dorsal intra-articular fragments (>1mm step-off) | Isolated radial styloid fractures (better treated percutaneously) |
| Reduction Status | Failure of closed reduction (residual dorsal tilt >10°) | Stable extra-articular fractures amenable to casting |
| Bone Quality | Adequate cortical density for screw purchase | Severe osteoporosis (volar locked plating preferred) |
| Soft Tissue Status | Intact dorsal soft tissue envelope | Active local infection, severe traumatic soft tissue compromise |
Pre-Operative Planning, Templating, and Patient Positioning
Advanced Imaging Modalities
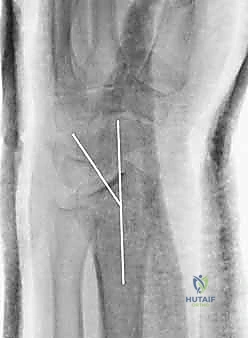
Exceptional surgical execution is predicated upon exhaustive preoperative planning. We do not simply look at an x-ray and head to the OR; we meticulously deconstruct the fracture anatomy using multiple imaging modalities. Standard posteroanterior (PA), lateral, and oblique radiographs are our baseline. On the PA view, we rigorously quantify radial inclination, radial length, and ulnar variance. On the lateral view, we assess the critical volar tilt and the degree of dorsal cortical comminution.

However, plain radiographs are often insufficient for complex intra-articular fractures. A non-contrast Computed Tomography (CT) scan with 2D and 3D reconstructions is practically mandatory in my practice for any intra-articular involvement. The CT scan maps the exact topography of the articular step-offs, identifies occult die-punch fragments, and reveals coronal split fractures that plain films obscure. This 3D understanding directly dictates our surgical approach, allowing us to anticipate whether a single dorsal plate, dual orthogonal plates, or a combination of fragment-specific implants will be required.
Digital Templating and Implant Selection
Once the fracture morphology is completely understood, we proceed to digital templating. Using the contralateral, uninjured wrist as a radiographic baseline is an invaluable technique for establishing the patient's native ulnar variance and radial height. We overlay digital templates of various dorsal plates to determine the optimal implant length and contour.
Templating allows us to anticipate the trajectory of our locking screws, ensuring they will adequately capture the critical subchondral bone of the distal fragments without penetrating the radiocarpal joint or the DRUJ. We must also ensure that our chosen plate is sufficiently long to span the metaphyseal comminution and achieve robust bicortical purchase in the intact radial diaphysis proximally. Having a comprehensive array of low-profile, anatomically contoured dorsal plates, including T-plates, L-plates, and straight plates, readily available in the operating room is crucial.
Patient Positioning and Operating Room Setup
The patient is positioned supine on the operating table with the operative extremity extended onto a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. Proper positioning of the fluoroscopy unit (C-arm) is critical for intraoperative efficiency. The C-arm should be brought in perpendicular to the patient, with the monitor positioned directly across from the surgeon to allow for effortless viewing without breaking scrub or turning the head awkwardly.


We prep and drape the arm to above the elbow to allow for unrestricted manipulation of the limb. Prior to exsanguination and tourniquet inflation, a final time-out is performed, and prophylactic intravenous antibiotics are administered. The arm is then elevated, exsanguinated with an Esmarch bandage, and the tourniquet is inflated to 250 mmHg (or 100 mmHg above systolic pressure). We are now ready to proceed with the surgical approach.
Step-by-Step Surgical Approach and Fixation Technique
Incision and Superficial Dissection
We begin with a longitudinal dorsal incision, approximately 6 to 8 centimeters in length, centered precisely over Lister's tubercle. The incision should be perfectly straight; zigzag incisions on the dorsal wrist can lead to unsightly, contracted scars.


Skin and subcutaneous tissues are sharply incised. Meticulous hemostasis is achieved using bipolar electrocautery to avoid thermal injury to the superficial nerves. We perform blunt dissection through the subcutaneous fat, remaining acutely vigilant for the crossing branches of the radial sensory nerve radially and the dorsal sensory branch of the ulnar nerve ulnarly. These sensory branches must be gently mobilized and protected with soft vessel loops if they cross our surgical field. Deepening the dissection, we expose the thick, transverse fibers of the extensor retinaculum.
Extensor Retinaculum Management and Deep Exposure
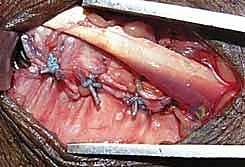
The key to the dorsal approach is the strategic management of the extensor compartments. We identify the third extensor compartment by palpating Lister's tubercle. Using a #15 blade, we longitudinally incise the roof of the third compartment, completely releasing the extensor pollicis longus (EPL) tendon. The EPL is then carefully transposed radially or ulnarly and protected with a Penrose drain.


Clinical & Radiographic Imaging Archive