High-Pressure Injection Injuries of the Hand: An Operative Masterclass

Key Takeaway
This masterclass provides a comprehensive, immersive guide to managing high-pressure injection injuries of the hand. We delve into critical surgical anatomy, meticulous preoperative planning, and granular intraoperative execution using Bruner’s and midaxial incisions. Fellows will learn to identify and débride affected tissues, protect vital neurovascular structures, and manage potential complications. Postoperative care, including splinting and staged débridement, is emphasized to optimize patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
High-pressure injection injuries of the hand represent one of the most deceptive and devastating surgical emergencies encountered in orthopedic and hand surgery. To the uninitiated observer, the clinical presentation often appears remarkably benign—a pinpoint puncture wound, perhaps a drop of blood or a minor bead of grease, and a patient who may initially complain only of mild discomfort. However, this innocuous exterior masks a catastrophic internal environment characterized by profound mechanical disruption, severe chemical cytotoxicity, and rapidly escalating compartment pressures that threaten both limb viability and systemic health. This is not merely a laceration; it is an explosive internal trauma that demands immediate, aggressive, and meticulous surgical intervention to salvage the extremity and preserve function.

The biomechanics of these injuries are dictated by the immense forces generated by industrial equipment. While the human skin can be breached by pressures as low as 100 pounds per square inch (psi), modern industrial injectors—such as paint sprayers, grease guns, and hydraulic lines—routinely operate at pressures ranging from 2,000 to 12,000 psi (141 to 703 kg/cm²). When a nozzle is accidentally discharged in close proximity to or in direct contact with the skin, the kinetic energy transfer is massive. The fluid acts as a high-velocity projectile, overcoming tissue resistance and dissecting aggressively along paths of least resistance, which in the hand typically correspond to neurovascular bundles, fascial planes, and synovial sheaths.

The ultimate extent of tissue necrosis and the subsequent prognosis are multifactorial, driven primarily by the pressure of the injection, the volume of the injectate, and the specific chemical composition of the substance. Higher pressures correlate directly with wider and deeper anatomical dissemination, while larger volumes cause immediate tissue distention, mechanical compression of the microvasculature, and acute compartment syndrome. Landmark studies by Gelberman, Schoo, and Hayes have unequivocally demonstrated that higher-volume injections, combined with delayed surgical decompression, result in exponentially higher morbidity and amputation rates.
The chemical nature of the injected substance is perhaps the most critical determinant of limb survival. Paint solvents and thinners possess extremely low viscosity, allowing them to diffuse rapidly through soft tissues. Furthermore, these substances are highly cytotoxic, inducing immediate lipid dissolution of cell membranes and severe corrosive tissue necrosis. Consequently, paint and solvent injections carry an exceptionally high amputation rate, frequently approaching 80%. Conversely, grease injections, being highly viscous, tend to remain more localized but provoke a profound, chronic foreign-body inflammatory response, leading to progressive fibrosis and oleogranuloma formation. Hydraulic fluids and automotive greases occupy a middle ground, with reported amputation risks of 14% and 23%, respectively.
The natural history of an untreated or inadequately treated high-pressure injection injury progresses inexorably through three distinct pathophysiologic stages. The Acute Stage occurs immediately upon injection, characterized by direct mechanical tissue tearing, acute compartment distention, and profound vasospasm of the digital vessels. This manifests clinically as a pale, mottled, and exquisitely painful digit, often accompanied by paresthesias due to direct chemical irritation or mechanical compression of the digital nerves. The Intermediate Stage follows within days, marked by a fierce foreign-body reaction, intense macrophage infiltration, and the onset of oleogranuloma formation and progressive fibrosis. Finally, the Late Stage is defined by the breakdown of these granulomas, resulting in chronic draining sinuses, intractable pain, severe contractures, and secondary polymicrobial infections (commonly involving Staphylococcus aureus, Streptococcus epidermidis, and Pseudomonas spp.). In rare, chronic cases, these draining sinuses can undergo malignant transformation into squamous cell carcinoma.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the intricate, compartmentalized anatomy of the hand is absolute prerequisite for the operating surgeon. The anatomical architecture of the hand does not merely house the injury; it actively dictates the trajectory of the injected material. When fluid is injected at high pressure, it behaves according to fluid dynamics, seeking the path of least resistance. In the tightly packed confines of the hand and digits, these paths are defined by the unyielding fascial septa, the synovial sheaths, and the neurovascular canals.
Digital Anatomy and the Flexor Tendon Sheath
Within the digits, the flexor tendon sheath and its associated pulley system serve as the primary conduit for longitudinal spread. The sheath is a closed synovial system designed to reduce friction, but under high-pressure injection, it becomes a pressurized pipeline. The annular pulleys (A1 through A5) are thick, rigid, and unyielding, whereas the cruciate pulleys (C1 through C3) are thin and pliable. If the injection nozzle breaches the skin directly over a flexion crease (such as the proximal or distal interphalangeal joints), the injectate is frequently driven directly into the synovial sheath. Once inside, the fluid rapidly tracks proximally and distally along the tendons, constrained only by the anatomical limits of the bursa.
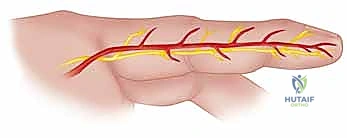
Conversely, if the injection occurs into the mid-substance of the phalangeal segments—away from the flexion creases and the immediate vicinity of the sheath—the fluid is often diverted by the rigid annular pulleys. In these instances, the injectate tends to spread laterally and circumferentially within the superficial subcutaneous tissues, tracking along the neurovascular bundles rather than entering the sheath directly. The digital neurovascular bundles, situated volar-laterally, are exquisitely vulnerable. Each bundle contains digital nerves and arteries that are highly susceptible to both the direct mechanical compression of the fluid volume and the intense chemical vasospasm induced by the injectate, leading to rapid digital ischemia.
Synovial Bursae and Proximal Dissemination
The anatomical configuration of the synovial sheaths is the most critical factor in predicting the proximal extent of the injury into the palm and forearm. The synovial sheaths of the index, long, and ring fingers typically terminate proximally at the level of the metacarpophalangeal (MCP) joints. Therefore, injections into these central digits are often contained within the digit itself or the immediate distal palm. However, the anatomy of the thumb and the little finger presents a significantly higher risk for catastrophic proximal spread.
The synovial sheath of the little finger is frequently continuous with the ulnar bursa, while the sheath of the thumb is continuous with the radial bursa. These bursae extend proximally through the carpal tunnel and into the distal forearm, terminating in Parona's space (the deep fascial space situated between the pronator quadratus and the deep flexor tendons). Consequently, a high-pressure injection into the pulp of the thumb or little finger can traverse the entire length of the hand in milliseconds, depositing highly toxic material into the deep spaces of the palm, the carpal tunnel, and the distal forearm, necessitating massive surgical exposure and decompression.
Palmar Spaces and Forearm Compartments
Injections occurring directly into the palm, thenar eminence, or hypothenar eminence are generally contained within their respective myofascial compartments (the thenar space, midpalmar space, and hypothenar space). While the larger, more compliant tissue planes of the palm allow for greater volume accommodation compared to the digits—often resulting in a slightly lower immediate risk of digital necrosis—the chemical toxicity remains profound. The surgeon must be acutely aware of the superficial and deep palmar arterial arches, the motor recurrent branch of the median nerve, and the deep motor branch of the ulnar nerve, all of which can be encased in toxic injectate.
If the injection breaches the boundaries of the hand and enters the forearm, the risk of acute compartment syndrome of the flexor, extensor, or mobile wad compartments becomes imminent. The fascial compartments of the forearm cannot accommodate sudden, high-volume fluid shifts without a catastrophic rise in intracompartmental pressure. This leads to microvascular collapse, muscle ischemia, and impending Volkmann's ischemic contracture. In such scenarios, the median, ulnar, and radial nerves, along with their accompanying major vascular axes, are at extreme risk, mandating emergent and wide-ranging fasciotomies extending from the wrist to the proximal forearm.
Exhaustive Indications and Contraindications
The management of high-pressure injection injuries is almost exclusively surgical. The fundamental principle is that these injuries represent an acute surgical emergency where "time is tissue." Delay in surgical decompression and radical debridement is directly correlated with an exponential increase in the rate of amputation and permanent functional loss. Non-operative management is universally condemned for almost all industrial injectates.
Indications for Emergent Surgery
The primary indication for emergent operative intervention is a confirmed or highly suspected high-pressure injection injury involving any chemical substance, including paint, solvents, oil, grease, hydraulic fluid, cement, or molten materials. Surgery is indicated regardless of the initial clinical appearance of the wound, which, as previously noted, is notoriously deceptive. The goals of surgery are tripartite: immediate decompression of all involved fascial compartments and tendon sheaths to restore microvascular perfusion; radical mechanical debridement of all foreign material and necrotic tissue to halt the cytotoxic cascade; and copious irrigation to dilute any remaining chemical residue.
Furthermore, the presence of severe pain disproportionate to the visible injury, pallor, diminished capillary refill, or sensory deficits in the affected digit are absolute indications for immediate exploration. Radiographic evidence of subcutaneous emphysema (air tracking along tissue planes) or radiopaque foreign material further confirms the need for urgent surgical tracking of the injectate's path. The optimal window for intervention is within 3 to 6 hours of the injury; interventions delayed beyond 10-12 hours are associated with dismal salvage rates, particularly with solvent-based injections.
Relative Contraindications and Non-Operative Scenarios
True absolute contraindications to surgery are exceedingly rare and generally limited to patients who are medically unstable to undergo anesthesia due to severe concomitant life-threatening trauma or profound medical comorbidities. In such extreme cases, life-saving measures take precedence over limb salvage.
Relative contraindications, or scenarios where a highly monitored non-operative approach might be cautiously considered by an experienced hand surgeon, are limited to very specific, low-pressure injections of benign substances. For example, a confirmed low-pressure injection of pure air or clean water, presenting with minimal swelling, normal perfusion, and no neurovascular compromise, may be managed with close inpatient observation, elevation, and broad-spectrum intravenous antibiotics. However, if there is any doubt regarding the pressure, the substance, or the clinical trajectory, surgical exploration is the safest and most appropriate course of action.
| Indication / Contraindication Category | Specific Clinical Scenarios | Rationale for Management |
|---|---|---|
| Absolute Indications | Injection of paint, solvents, thinners, oil, grease, hydraulic fluid, cement. | High cytotoxicity, rapid onset of compartment syndrome, high risk of necrosis. Requires emergent radical debridement. |
| Absolute Indications | Signs of ischemia (pallor, absent capillary refill), severe disproportionate pain, sensory loss. | Indicates neurovascular compromise and impending tissue death. Emergent decompression mandatory. |
| Absolute Indications | Radiographic evidence of extensive subcutaneous air or radiopaque tracking. | Confirms wide dissemination of injectate along fascial planes requiring extensive surgical exposure. |
| Relative Contraindications | Pure air or clean water injection at confirmed low pressure with normal neurovascular exam. | May be observed inpatient with IV antibiotics, elevation, and serial exams. Any deterioration mandates surgery. |
| Absolute Contraindications | Patient in extremis, medically unstable for anesthesia, life-threatening polytrauma. | "Life over limb" principle. Patient must be stabilized before extremity surgery can be safely undertaken. |
Pre-Operative Planning, Templating, and Patient Positioning
Successful surgical execution in the face of a high-pressure injection injury begins long before the patient enters the operating theater. The preoperative phase is a critical window for gathering intelligence about the "enemy" (the injectate) and meticulously planning the surgical approach to minimize collateral damage while maximizing exposure.
Detailed History and Physical Examination
The history is paramount. The surgeon must aggressively pursue the exact nature of the injected substance, the estimated pressure of the device, and the precise time of injury. Contacting the patient's employer to obtain the Material Safety Data Sheet (MSDS) is not optional; it is a critical step. The MSDS provides indispensable data regarding the chemical's pH, its lipid solubility, its systemic toxicity profile (e.g., risk of hydrocarbon pneumonitis or renal failure), and specific neutralizing agents, if any exist. The time elapsed since the injury dictates the urgency and heavily influences the preoperative counseling regarding the likelihood of amputation.
The physical examination must be systematic and thorough. The puncture site, often no larger than a pinhead, must be identified and marked. The surgeon must evaluate the resting cascade of the hand and perform a meticulous assessment of active and passive range of motion. Severe pain elicited by passive extension of the digit is a hallmark sign of flexor tenosynovitis and confirms that the injectate has breached the synovial sheath. A rigorous neurovascular examination, documenting two-point discrimination, light touch, and capillary refill, establishes a baseline against which postoperative recovery will be measured. Palpation of the entire upper extremity, searching for crepitus, induration, and tenderness, helps map the potential proximal spread of the substance.
Diagnostic Imaging and Anesthetic Considerations
While time should never be wasted on unnecessary diagnostics, standard plain radiographs in multiple orthogonal planes (anteroposterior, lateral, and oblique) of the hand, wrist, and forearm are mandatory. Even if the injected substance is radiolucent (as many paints and organic solvents are), radiographs frequently reveal subcutaneous emphysema—air driven into the tissues alongside the fluid—which acts as a reliable tracer for the extent of dissemination. Radiographs also rule out underlying fractures or pre-existing osseous pathology. Advanced imaging modalities, such as MRI or high-resolution ultrasound, are generally contraindicated in the acute setting due to the unacceptable delay they cause, though they hold value in the delayed management of chronic granulomas.
Anesthetic management requires careful coordination with the anesthesia team. Regional anesthesia, specifically a well-executed axillary or supraclavicular brachial plexus block, is highly advantageous. It provides excellent intraoperative operating conditions, profound muscle relaxation, and crucial postoperative sympathectomy, which aids in mitigating digital vasospasm and maximizing microvascular perfusion. However, it is a cardinal rule that local anesthetic blocks (e.g., digital blocks or local infiltration) must never be performed directly into the injured extremity. Injecting additional volume into an already compromised, tightly closed compartment will directly exacerbate the ischemia and mechanically drive the toxic injectate further into healthy tissues.
Patient Positioning and Strict Tourniquet Protocols
The patient is positioned supine on the operating table, with the injured upper extremity abducted and resting on a specialized radiolucent hand table. This setup provides the surgeon and the assistant with unobstructed, circumferential 360-degree access to the hand, wrist, and entire forearm, anticipating the potential need for extensive proximal dissection.
The management of the surgical tourniquet in these cases is governed by a strict, non-negotiable principle: Under no circumstances should the limb be exsanguinated using an Esmarch bandage or any other form of compressive elastic wrap. Applying external compression to the limb will inevitably act like a piston, forcing the highly toxic, pressurized injectate proximally along the tendon sheaths and neurovascular bundles, transforming a localized digital injury into a catastrophic pan-hand or forearm disaster.
Instead, the surgeon must rely exclusively on gravity exsanguination. The limb is elevated at a 45- to 60-degree angle for a minimum of 3 to 5 minutes to allow venous drainage before the pneumatic tourniquet is inflated to standard upper extremity pressures (typically 250 mm Hg). Often, the surgeon may elect to make the initial exploratory incisions without the tourniquet inflated to assess the baseline perfusion of the tissues, inflating it only when a bloodless field is strictly required for the meticulous dissection of the neurovascular bundles.
Step-by-Step Surgical Approach and Fixation Technique
The intraoperative philosophy for a high-pressure injection injury is one of radical, uncompromising debridement. There is absolutely no role for minimally invasive, percutaneous, or "keyhole" techniques. The surgeon must commit to wide, extensile exposures that allow for direct visualization of every potentially contaminated structure. The goal is to track the injectate to its absolute furthest anatomical extent, removing all foreign material and non-viable tissue until only pristine, healthy, bleeding tissue remains.

Approach 1: The Bruner Zig-Zag Incision
The Bruner (zig-zag) incision is the workhorse approach for the volar aspect of the digits and palm. Its primary advantage is that it provides exceptional, wide-angle exposure of the flexor tendon sheath and the neurovascular bundles while explicitly avoiding linear longitudinal scars that cross flexion creases, which would inevitably result in severe, function-limiting flexion contractures during the healing phase.
Using a #15 scalpel blade, the incision is initiated at the puncture site and extended proximally and distally in a zig-zag fashion. The apices of the triangular flaps must be carefully planned to lie along the mid-lateral lines of the digit, positioned over the non-crease areas of the phalangeal shafts. The transverse limbs of the incision must fall precisely within the natural volar flexion creases of the distal interphalangeal (DIP), proximal interphalangeal (PIP), and metacarpophalangeal (MCP) joints.

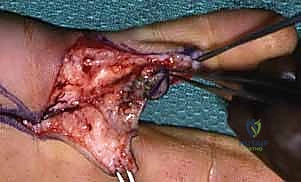
As the skin flaps are elevated, full-thickness dissection is maintained to preserve the subdermal vascular plexus and prevent flap necrosis. The immediate subcutaneous tissues are often heavily infiltrated with the injectate, appearing discolored, edematous, and necrotic. The first critical anatomical landmarks to identify are the digital neurovascular bundles.

Using operating loupe magnification (minimum 2.5x to 3.5x) and fine blunt dissection with tenotomy scissors, the neurovascular bundles are meticulously skeletonized and retracted volar-laterally. They are frequently found encased in the injected chemical, exhibiting severe vasospasm. Extreme care must be taken to avoid iatrogenic injury to these already compromised structures.
Once the bundles are secured, attention is turned to the flexor tendon sheath. If there is any visible injectate within the sheath, or if the sheath appears distended or inflamed, a formal tenosynovectomy is mandatory.

The sheath is opened longitudinally, carefully preserving the critical A2 and A4 annular pulleys to prevent postoperative tendon bowstringing, provided these pulleys are not irreversibly infiltrated with necrotic material. A fine curette, delicate forceps, and copious low-pressure pulsatile lavage with warm sterile saline are utilized to systematically eradicate all foreign material, chemical residue, and necrotic synovium. The debridement must continue proximally into the palm and, if necessary, through the carpal tunnel into the forearm, until the exact termination point of the injectate is identified and cleared.
Approach 2: The Mid-Axial Incision
While the Bruner incision is generally preferred for its versatility, the mid-axial approach serves as a critical alternative, particularly when the injection is localized to the lateral aspects of the digit or when there is profound dorsal and volar swelling where a volar incision might compromise the vascularity of the skin flaps.

The mid-axial line is determined by connecting the apices of the dorsal flexion creases when the finger is fully flexed. The incision is made precisely along this line, dorsal to the neurovascular bundle. This approach provides a direct, linear route to the flexor tendon sheath while keeping the neurovascular bundle safely protected in the volar flap.
The dissection proceeds volar to the extensor apparatus and dorsal to the neurovascular bundle. Cleland's ligaments must be divided to gain full access to the flexor sheath. The principles of debridement remain identical to the Bruner approach: meticulous identification of structures, radical excision of necrotic tissue, and exhaustive irrigation. The mid-axial approach is particularly useful for accessing the retrovascular spaces where injectate frequently pools.
Wound Management and Closure
Following exhaustive debridement, the management of the surgical wound is a critical decision point. Primary closure of a high-pressure injection wound is almost universally contraindicated. The risk of ongoing tissue necrosis, escalating postoperative edema, and secondary infection is simply too high.

The wounds must be left open to allow for continued drainage of residual chemical toxins, inflammatory exudate, and to accommodate the inevitable postoperative swelling without inducing a secondary iatrogenic compartment syndrome. The exposed tendons and neurovascular structures are protected with a non-adherent, moist dressing (such as Xeroform or a specialized silicone interface). The hand is immobilized in a bulky, non-compressive soft dressing with a volar plaster splint, positioning the hand in the intrinsic-plus (safe) position: wrist extended 20-30 degrees, MCP joints flexed 70-90 degrees, and PIP/DIP joints in full extension. The patient is scheduled for a mandatory planned "second-look" debridement in the operating room 48 to 72 hours later to assess tissue viability and perform further debridement as necessary.
Complications, Incidence Rates, and Salvage Management
The complication profile for high-pressure injection injuries is formidable, reflecting the devastating nature of the initial trauma. Even with prompt, expert surgical intervention, patients frequently face significant long-term morbidity. The surgeon must comprehensively counsel the patient and family regarding these risks during the preoperative phase.
Ischemic Necrosis and Amputation
The most catastrophic and immediate complication is irreversible ischemic necrosis of the digit or limb, culminating in amputation. This is primarily driven by the chemical cytotoxicity of the injectate, compounded by the mechanical pressure of the fluid and the secondary microvascular thrombosis.
As previously emphasized, the amputation rate is highly dependent on the injected substance. Paint, paint thinners, and industrial solvents are the most lethal, with amputation rates frequently cited between 50% and 80%. These substances cause rapid lipid dissolution and irreversible cellular death.

When amputation becomes inevitable due to demarcated necrosis, the surgical principle is to preserve as much functional length as possible while ensuring all non-viable and contaminated tissue is resected. Transphalangeal amputations or formal ray resections may be required, depending on the proximal extent of the necrosis.
Oleogranuloma Formation and Chronic Infection
Injections of more viscous, less acutely cytotoxic substances, such as grease or oil, frequently result in the formation of oleogranulomas. This is a chronic, severe foreign-body giant cell reaction where the body attempts to wall off the indigestible lipid material.

These granulomas present as hard, nodular, painful masses that severely restrict tendon gliding and joint motion. Over time, these granulomas can break down, leading to chronic, draining, fistulous tracts to the skin surface. Secondary bacterial colonization of these necrotic tracts is common, leading to deep space infections, osteomyelitis, and septic arthritis. Salvage management of established oleogranulomas requires aggressive, wide surgical excision of the granulomatous mass, which often necessitates complex soft tissue reconstruction, including local or regional flap coverage, to restore a functional gliding surface.
Stiffness, Contracture, and Chronic Pain
Even in cases where the limb is successfully salvaged without amputation, severe functional impairment is the rule rather than the exception. The intense inflammatory response, combined with the necessity for wide surgical dissection and potential excision of crucial pulleys or tendon segments, leads to profound scarring and fibrosis. Patients frequently develop severe flexion contractures of the PIP and DIP joints, and a significant loss of total active motion (TAM). Furthermore, injury to the digital nerves, either from direct chemical toxicity or surgical manipulation, can result in chronic neuropathic pain, hypersensitivity, and the development of Complex Regional Pain Syndrome (CRPS).
| Complication | Estimated Incidence | Primary Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Amputation | 15% - 80% (Substance dependent) | Solvents/Paint, delayed surgery (>6 hrs), high pressure, digital injection. | Ray resection, transphalangeal amputation, functional length preservation. |
| Oleogranuloma | High with grease/oil | Grease/Oil injection, incomplete initial debridement. | Radical excision of granuloma, tenolysis, potential flap coverage. |
| Severe Stiffness / Contracture | > 60% of salvaged digits | Extensive tenosynovectomy, pulley excision, prolonged immobilization. | Aggressive hand therapy, delayed tenolysis, capsulotomy, potential joint |
Clinical & Radiographic Imaging Archive