Medial Epicondylitis Release: An Intraoperative Masterclass in Flexor-Pronator Debridement and Ulnar Nerve Management
Key Takeaway
Join us in the OR for an in-depth masterclass on open medial epicondylitis release. We'll meticulously debride the flexor-pronator origin, address concurrent ulnar nerve pathology, and prepare the epicondyle for optimal healing. Learn crucial anatomical landmarks, avoid common pitfalls, and ensure excellent patient outcomes with precise technique and comprehensive postoperative care.
Comprehensive Introduction and Patho-Epidemiology
The Evolution of Medial Epicondylitis Understanding
Medial epicondylitis, historically and colloquially referred to as "golfer's elbow," represents a complex degenerative condition affecting the common flexor-pronator origin at the medial epicondyle of the humerus. While the moniker suggests an exclusive link to golf, the demographic reality is far more expansive, frequently encompassing racquet sports athletes, overhead throwing athletes, and manual laborers subjected to repetitive forearm pronation and wrist flexion. The evolution of our understanding of this disease process has fundamentally shifted from an acute inflammatory paradigm to a chronic degenerative model. This paradigm shift is critical for the orthopedic surgeon, as it dictates both non-operative algorithms and the precise nature of surgical intervention. The pathology is not driven by an influx of acute inflammatory cells, but rather by a failed healing response to repetitive microtrauma, necessitating a surgical approach focused on meticulous débridement rather than mere release.
Histopathologic Hallmarks: Angiofibroblastic Tendinosis
The fundamental histopathologic hallmark of medial epicondylitis is angiofibroblastic tendinosis, a term popularized by Nirschl to describe the specific degenerative cascade occurring within the tendinous architecture. Repetitive eccentric loading of the flexor-pronator mass exceeds the tendon's intrinsic reparative capacity, leading to microtearing of the collagen fibers. Instead of progressing through the normal phases of inflammation, proliferation, and remodeling, the tissue enters a state of arrested healing. Histological analysis consistently reveals a disorganized proliferation of fibroblasts, atypical vascular granulation tissue (neovascularization), and a profound absence of traditional inflammatory cells such as macrophages or neutrophils. The native highly organized Type I collagen is progressively replaced by weaker, disorganized Type III collagen and mucoid ground substance. This structurally inferior tissue lacks the tensile strength required for normal biomechanical function, perpetuating a cycle of recurrent microtrauma, pain, and functional limitation.
Epidemiological Profile and Occupational Hazards
Epidemiologically, medial epicondylitis is less prevalent than its lateral counterpart, accounting for approximately 10% to 20% of all epicondylitis cases. It typically presents in the fourth and fifth decades of life, with a relatively equal distribution between males and females, though some occupational cohorts show a male predominance due to heavy manual labor. The dominant arm is affected in over 75% of cases. Occupational hazards strongly associated with the development of medial epicondylitis include professions requiring repetitive forceful gripping, heavy lifting, or the use of vibratory tools. In the athletic population, the pathology is frequently observed in baseball pitchers (often concomitant with medial ulnar collateral ligament insufficiency), tennis players utilizing heavy topspin forehands, and golfers, particularly those who consistently strike the ground prior to the ball. Recognizing these epidemiological and biomechanical risk factors is essential for accurate diagnosis, comprehensive patient counseling, and the implementation of effective postoperative rehabilitation strategies.
Detailed Surgical Anatomy and Biomechanics
Osteology and the Medial Epicondylar Axis
A profound mastery of the regional anatomy is the absolute prerequisite for safe and effective surgical intervention in the medial elbow. The medial epicondyle serves as the primary osteological landmark and anchor point for the dynamic and static stabilizers of the medial elbow. It is a robust, non-articular prominence located proximal to the trochlea. The anterior facet of the medial epicondyle provides the broad footprint for the common flexor-pronator tendon. Distal and slightly posterior to the epicondyle lies the sublime tubercle of the proximal ulna, the critical insertion site for the anterior bundle of the medial collateral ligament (MCL). The spatial relationship between the medial epicondyle, the sublime tubercle, and the joint line dictates the complex biomechanics of valgus stability and flexor-pronator tensioning during the throwing motion or forceful grip.
The Common Flexor-Pronator Mass Architecture
The common flexor-pronator mass is a confluence of five distinct muscle-tendon units originating from the medial epicondyle and the adjacent medial supracondylar ridge. From proximal-anterior to distal-posterior, these include the pronator teres (PT), flexor carpi radialis (FCR), palmaris longus (PL), flexor digitorum superficialis (FDS), and flexor carpi ulnaris (FCU). The primary locus of pathology in medial epicondylitis is almost universally localized to the interface between the humeral head of the pronator teres and the origin of the flexor carpi radialis. The FDS and FCU are less frequently involved in the primary tendinotic process but are critical anatomic landmarks. The fascial confluence of these muscles creates a robust aponeurosis that must be carefully incised and later meticulously repaired to restore the dynamic buttress effect they provide to the medial elbow.
Neurovascular Topography: Ulnar Nerve and MACN
The neurovascular topography of the medial elbow is notoriously unforgiving, demanding meticulous surgical technique to avoid devastating iatrogenic complications. Superficial to the flexor-pronator fascia courses the medial antebrachial cutaneous nerve (MACN). The MACN typically divides into an anterior and posterior branch, both of which are highly variable in their trajectory and frequently cross the standard surgical incision for medial epicondylitis. Injury to the MACN can result in painful neuromas and debilitating dysesthesias. Deep to the flexor-pronator mass, and posterior to the medial epicondyle, lies the ulnar nerve within the cubital tunnel. The nerve is bounded by the medial epicondyle anteriorly, the olecranon posteriorly, and Osborne's fascia (the cubital tunnel retinaculum) superficially. As the nerve exits the cubital tunnel, it passes between the two heads of the FCU. The ulnar nerve is exquisitely vulnerable to compression, traction, and direct surgical trauma during medial elbow procedures, necessitating routine preoperative evaluation and, frequently, concurrent intraoperative management.
The Medial Collateral Ligament Complex
Lying immediately deep to the common flexor-pronator origin is the medial collateral ligament (MCL) complex, the primary static stabilizer against valgus stress at the elbow. The MCL consists of three bundles: the anterior, posterior, and transverse bundles. The anterior bundle is the most critical for valgus stability, originating from the anteroinferior surface of the medial epicondyle—directly deep to the FDS and FCR origins—and inserting onto the sublime tubercle. During the surgical débridement of the flexor-pronator mass, the surgeon must maintain a precise depth of resection. Overzealous débridement or failure to recognize the deep fascial boundary can result in iatrogenic violation of the anterior bundle of the MCL, leading to catastrophic postoperative valgus instability, particularly in overhead athletes.
Exhaustive Indications and Contraindications
Establishing Surgical Necessity
The decision to proceed with operative management for medial epicondylitis must be predicated on a rigorous, evidence-based algorithm. Medial epicondylitis is primarily a self-limiting condition, and the vast majority of patients will achieve symptomatic resolution with a comprehensive, well-structured non-operative regimen. Surgical intervention is strictly indicated only for patients who have demonstrated recalcitrant, functionally limiting pain that has failed to improve after a minimum of 6 to 12 months of dedicated conservative management. This management must include activity modification, targeted physical therapy (emphasizing eccentric strengthening of the flexor-pronator mass), judicious use of non-steroidal anti-inflammatory drugs (NSAIDs), and potentially biologic injections (such as Platelet-Rich Plasma). Furthermore, surgery is indicated when there is clear clinical and radiographic evidence of a high-grade partial tear or avulsion of the flexor-pronator origin, or when the tendinosis is accompanied by progressive, clinically significant ulnar neuropathy that demands concurrent decompression or transposition.
Absolute and Relative Contraindications
Contraindications to medial epicondylitis release must be carefully evaluated to prevent surgical failures and exacerbation of patient morbidity. Absolute contraindications include the presence of active local or systemic infection, severe medical comorbidities precluding safe anesthesia, and an inadequate trial of non-operative management (less than 6 months). Relative contraindications require nuanced clinical judgment. These include profound cervical radiculopathy mimicking medial elbow pain, severe concurrent glenohumeral pathology driving compensatory elbow overload, and unrecognized medial collateral ligament insufficiency. Operating on a patient with primary MCL instability under the guise of medial epicondylitis will uniformly fail and likely worsen the instability by compromising the dynamic flexor-pronator buttress. Additionally, patients with significant psychiatric overlays, secondary gain issues (such as active workers' compensation litigation), or an inability to comply with strict postoperative rehabilitation protocols should be approached with extreme caution.
| Category | Indications for Surgical Intervention | Contraindications (Absolute & Relative) |
|---|---|---|
| Clinical Timeline | Failure of 6-12 months of strict conservative care | Less than 6 months of conservative management |
| Pathology | Recalcitrant angiofibroblastic tendinosis | Active local or systemic infection (Absolute) |
| Structural | High-grade partial tear or chronic avulsion | Primary undiagnosed MCL instability (Relative) |
| Neurologic | Concomitant progressive ulnar neuropathy | Cervical radiculopathy mimicking elbow pain (Relative) |
| Patient Factors | Severe functional limitation affecting ADLs/Work | Inability to comply with postoperative rehab (Relative) |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical Assessment and Provocative Maneuvers
Preoperative planning is the foundation upon which surgical success is built. The clinical assessment must be exhaustive. The classic presentation involves insidious onset of medial elbow pain, exacerbated by gripping and pronation. On physical examination, the hallmark finding is pinpoint tenderness over the anterior aspect of the medial epicondyle and the proximal flexor-pronator mass. Provocative maneuvers are essential for confirming the diagnosis. The surgeon must elicit pain with resisted wrist flexion and, most sensitively, resisted forearm pronation with the elbow extended. A comprehensive neurological examination is non-negotiable. The ulnar nerve must be assessed for Tinel's sign at the cubital tunnel, subluxation during active elbow flexion and extension, and signs of advanced neuropathy such as intrinsic muscle wasting or sensory deficits in the ulnar digits. Furthermore, valgus stability testing, specifically the moving valgus stress test, must be performed to rule out concurrent MCL insufficiency, a critical masquerader of medial epicondylitis in the throwing athlete.
Advanced Imaging Modalities
While the diagnosis of medial epicondylitis is primarily clinical, advanced imaging is an indispensable tool for surgical planning, confirming the extent of pathology, and ruling out concomitant intra-articular or ligamentous lesions. Plain radiographs (anteroposterior, lateral, and oblique views) are obtained routinely to evaluate for medial epicondylar traction osteophytes, heterotopic ossification, or intra-articular loose bodies. Magnetic Resonance Imaging (MRI) is the gold standard advanced modality. A high-resolution MRI without contrast will reliably demonstrate the pathologic changes of tendinosis. The surgeon must look for increased signal intensity within the common flexor tendon on fluid-sensitive sequences (T2-weighted or STIR), indicating mucoid degeneration and edema. T1-weighted sequences often reveal thickening of the tendon origin. Crucially, the MRI allows for a detailed evaluation of the MCL complex to ensure its integrity prior to planned surgical débridement.
Operating Room Setup and Patient Positioning
Optimal patient positioning is critical for ensuring excellent surgical exposure, minimizing surgeon fatigue, and protecting vulnerable neurovascular structures. The patient is positioned supine on the operating table. A standard hand table or arm board is securely attached to the operative side. The operative extremity is prepped and draped in a standard sterile fashion, allowing for full mobility of the elbow, wrist, and hand. A sterile tourniquet is typically applied to the proximal arm to ensure a bloodless surgical field, though some surgeons prefer to operate without a tourniquet to continuously visualize the vascularity of the tissues. The arm is externally rotated at the shoulder and supinated at the forearm. Crucially, meticulous padding must be placed under the elbow and the ulnar nerve to prevent iatrogenic compression neurapraxia during the procedure. The arm should rest in a stable position, typically with the elbow flexed to approximately 45 to 60 degrees, providing unhindered access to the medial epicondyle.
Step-by-Step Surgical Approach and Fixation Technique
Incision and Superficial Dissection
The surgical procedure begins with precise anatomical marking. A 3 to 5 cm longitudinal incision is planned, centered slightly anterior to the medial epicondyle and extending distally along the anatomical axis of the flexor-pronator mass. This longitudinal orientation is preferred as it aligns favorably with Langer's lines, optimizing postoperative cosmesis, and allows for proximal or distal extension if concomitant ulnar nerve transposition is required.

Upon incising the skin, the superficial dissection must proceed with extreme caution. Utilizing blunt dissection with Metzenbaum scissors, the surgeon carefully sweeps through the subcutaneous adipose tissue. The primary objective during this phase is the meticulous identification, mobilization, and protection of the medial antebrachial cutaneous nerve (MACN) branches. These sensory branches frequently arborize across the surgical field. Failure to identify and protect the MACN is a leading cause of postoperative morbidity, resulting in painful neuromas or hyperesthesia. Once identified, the nerve branches are gently retracted using vessel loops.
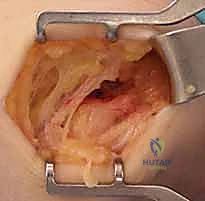
Deep Fascial Exposure and Interval Identification
With the subcutaneous tissues retracted and the MACN protected, the glistening fascia overlying the common flexor-pronator mass is exposed. Before proceeding deeper, the surgeon must palpate the ulnar nerve posterior to the medial epicondyle, confirming its location and assessing for any dynamic subluxation by ranging the elbow. Once the nerve is secure, attention is turned to the deep fascia. A longitudinal incision is made through the flexor-pronator fascia, precisely targeting the anatomical interval between the humeral head of the pronator teres (PT) anteriorly and the flexor carpi radialis (FCR) posteriorly.
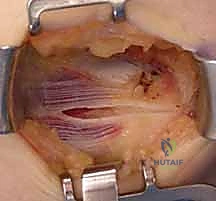
This specific interval is the most common locus of angiofibroblastic tendinosis. The fascial incision is made in line with the muscle fibers to minimize structural trauma and facilitate a robust closure. Using blunt retractors, the PT and FCR are gently separated and reflected, exposing the deeper, pathological tendinous tissue originating from the medial epicondyle.

In cases of advanced chronicity or acute-on-chronic trauma, the surgeon may encounter a frank rupture or avulsion of the flexor-pronator origin upon deep exposure. In such scenarios, the degenerative, retracted tissue must be identified and mobilized for subsequent repair.

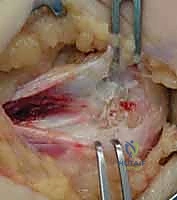
The Nirschl Scratch Test and Pathologic Debridement
The core of the procedure involves the precise identification and excision of the angiofibroblastic tissue. The pathologic tissue is visually distinct from normal tendon; it appears grayish, dull, friable, and unorganized, contrasting sharply with the glistening, white, longitudinally oriented fibers of healthy tendon. To definitively differentiate normal from abnormal tissue, the surgeon employs the "Nirschl scratch test." Using a No. 15 scalpel blade, the surgeon gently scrapes the tendinous origin. The pathologic, mucoid tissue is poorly adherent and will easily peel or scrape away, whereas healthy tendon tissue remains firmly attached to the bone and resists scraping.
Once the boundaries of the lesion are established, sharp excision is performed. The goal is an elliptical excision of the degenerative tissue, typically creating a defect approximately 1.0 to 1.5 cm in length and 3 to 5 mm in width, depending on the extent of the pathology.
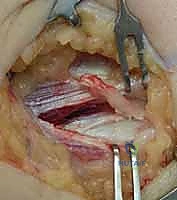
The débridement must be thorough, extending down to bleeding bone, but the surgeon must remain acutely aware of the depth of resection. The anterior bundle of the MCL lies immediately deep to this origin; violating this ligament is a catastrophic technical error that will result in iatrogenic valgus instability.
Cortical Decortication and Soft Tissue Repair
Following the complete excision of the tendinotic tissue, the exposed cortical bone of the medial epicondyle must be addressed to stimulate a robust healing response. Using a high-speed burr, an awl, or a small drill bit (e.g., 2.0 mm), the surgeon performs a partial decortication or microfracture of the epicondylar footprint. This critical step breaches the cortical bone to access the highly vascularized cancellous marrow elements. The release of marrow blood introduces mesenchymal stem cells, vascular endothelial growth factors, and other essential biologic mediators into the surgical bed, transforming a chronic, avascular, degenerative environment into an acute, highly vascularized healing milieu.

After decortication, the surgical site is thoroughly irrigated to remove any bone debris. The final major step is the secure repair and retensioning of the flexor-pronator mass. The healthy medial and lateral margins of the excised tendon defect are approximated. Using robust, non-absorbable or slowly absorbable sutures (e.g., No. 1 or 0 Vicryl or FiberWire) in a figure-of-eight or horizontal mattress configuration, the healthy tendon edges are firmly secured to each other and tied down over the decorticated bony footprint. This retensioning restores the dynamic structural integrity of the medial elbow.

Ulnar Nerve Management and Final Closure
Prior to final closure, the surgeon must definitively address the ulnar nerve, based on preoperative planning and intraoperative findings. If there is no evidence of neuropathy or subluxation, the nerve is left undisturbed in the cubital tunnel. However, if concurrent ulnar neuropathy is present, an in situ decompression is performed by releasing Osborne's fascia. If the nerve demonstrates dynamic subluxation, or in the setting of severe neuropathy, a subcutaneous or submuscular transposition is executed, securing the nerve anterior to the medial epicondyle.

Once neurovascular integrity is confirmed, the tourniquet is deflated, and meticulous hemostasis is achieved using electrocautery. The subcutaneous tissue is closed in layers using absorbable sutures, ensuring the MACN branches are not entrapped. The skin is closed with a running subcuticular suture or interrupted nylon sutures, depending on surgeon preference. A sterile, bulky, non-compressive dressing is applied, and the elbow is placed in a posterior splint at 90 degrees of flexion with the forearm in neutral rotation.
Complications, Incidence Rates, and Salvage Management
Iatrogenic Neurologic Injury
Surgical intervention for medial epicondylitis, while highly successful in carefully selected patients, carries a distinct risk profile, primarily due to the complex regional anatomy. The most frequent and often most debilitating complication is iatrogenic injury to the medial antebrachial cutaneous nerve (MACN). Occurring in approximately 2% to 5% of cases, injury to the anterior or posterior branches of the MACN can result in painful neuroma formation, hyperesthesia, or permanent numbness over the medial forearm. Meticulous superficial dissection and the use of loupe magnification are imperative to mitigate this risk. Furthermore, the ulnar nerve is at significant risk. Direct trauma, excessive traction, or failure to recognize and address a subluxating ulnar nerve can lead to severe postoperative ulnar neuropathy. If a patient develops new-onset ulnar nerve symptoms postoperatively, urgent clinical evaluation and potential electrodiagnostic testing are required to differentiate between transient neurapraxia and structural nerve injury requiring re-exploration.
Medial Collateral Ligament Insufficiency
A less common but biomechanically catastrophic complication is iatrogenic injury to the medial collateral ligament (MCL), specifically the anterior bundle. This occurs when the surgical débridement of the flexor-pronator origin is carried too deeply, violating the underlying capsuloligamentous structures. Patients will present with persistent medial elbow pain, subjective feelings of instability, and a positive moving valgus stress test. This complication is particularly devastating for overhead athletes. Prevention relies on a profound understanding of the 3-dimensional anatomy and strict adherence to the Nirschl scratch test to differentiate superficial tendinosis from deep ligamentous tissue. If iatrogenic MCL disruption occurs and is recognized intraoperatively, immediate primary repair is mandated. Delayed presentation typically requires formal MCL reconstruction (Tommy John surgery) using an autograft.
Recurrent Tendinosis and Surgical Failure
Despite meticulous surgical technique, a small percentage of patients (approximately 5% to 10%) will experience persistent or recurrent medial elbow pain, constituting a surgical failure. Recurrence is often multifactorial. It may stem from inadequate initial débridement of the angiofibroblastic tissue, failure to adequately decorticate the medial epicondyle to stimulate a healing response, or, very commonly, patient non-compliance with the postoperative rehabilitation protocol. Premature return to forceful gripping or overhead activities before the tendon has adequately remodeled can disrupt the repair and reignite the degenerative cascade. Salvage management for recurrent tendinosis is highly complex. It requires a comprehensive re-evaluation, including repeat MRI to assess the integrity of the repair and the MCL, and EMG/NCS to rule out delayed ulnar neuropathy. Revision surgery involves a more extensive débridement, potential augmentation with allograft or autograft tissue, and a highly conservative, prolonged rehabilitation phase.
| Complication | Incidence Rate | Preventive Strategy | Salvage / Management Protocol |
|---|---|---|---|
| MACN Neuroma / Injury | 2% - 5% | Meticulous blunt subcutaneous dissection; loupe magnification. | Gabapentinoids; localized nerve blocks; surgical excision of neuroma and burying into muscle belly. |
| Ulnar Neuropathy | 1% - 3% | Pre-op dynamic assessment; intra-op protection; concurrent transposition if indicated. | Observation for neurapraxia; EMG/NCS at 6 weeks; revision decompression or transposition if structural. |
| Iatrogenic MCL Injury | < 1% | Strict depth control during débridement; awareness of sublime tubercle anatomy. | Intra-op primary repair; delayed presentation requires formal autograft MCL reconstruction. |
| Recurrent Tendinosis | 5% - 10% | Complete excision of mucoid tissue; adequate cortical decortication; strict rehab compliance. | Prolonged conservative care; PRP injections; revision débridement with potential tissue augmentation. |
Phased Post-Operative Rehabilitation Protocols
Phase I: Immediate Post-Operative Protection
The postoperative rehabilitation following medial epicondylitis release is as critical to the final outcome as the surgical execution itself. The protocol is divided into distinct, biologically driven phases. Phase I (Weeks 0-2) is focused entirely on protecting the surgical repair, minimizing edema, and managing pain. The patient remains in the posterior splint applied in the operating room for the first 7 to 10 days. During this time, strict elevation and cryotherapy are employed. Active range of motion (ROM) of the shoulder, wrist, and digits is encouraged to prevent stiffness and promote venous return, provided these movements do not place tension on the flexor-pronator origin. At the first postoperative visit (typically day 10-14), the splint and sutures are removed. The patient is transitioned to a hinged elbow brace, initially locked at 90 degrees of flexion, to protect the healing tissue from sudden eccentric loads.
Phase II: Intermediate Motion and Early Strengthening
Phase II (Weeks 3-6) marks the transition from strict protection to the cautious restoration of elbow kinematics and early activation of the flexor-pronator mass. The hinged brace is gradually unlocked to allow progressive, pain-free active and active-assisted range of motion. The goal is to achieve full elbow extension and flexion by the end of week 6. Physical therapy is initiated, focusing initially on submaximal, pain-free isometric exercises for wrist flexion and forearm pronation. It is imperative that these exercises do not elicit pain at the medial epicondyle, as this indicates overloading of the immature repair tissue. Scapular stabilization and core strengthening exercises are also integrated during this phase to ensure the entire kinetic chain is optimized, particularly for athletic patients preparing for a return to sport.
Phase III: Advanced Strengthening and Return to Play
Phase III (Weeks 7-12+) represents the final stage of rehabilitation, focusing on tissue remodeling, advanced strengthening, and sport-specific functional training. The hallmark of this phase is the introduction of progressive eccentric strengthening of the flexor-pronator muscles. Eccentric loading is the most potent mechanical stimulus for collagen alignment and tendon hypertrophy. Patients utilize graded resistance bands and light dumbbells to perform controlled, lengthening contractions of the wrist flexors and pronators. As strength
