Anterior Instability: How Glenoid Bone Loss Shapes Treatment
Key Takeaway
This article provides essential research regarding Anterior Instability: How Glenoid Bone Loss Shapes Treatment. Glenoid bone loss refers to the reduction of bone from the glenoid, appearing as an identifiable fragment or attritional loss. It is a significant factor contributing to recurrent anterior shoulder instability. For substantial glenoid bone loss, typically over 20%, surgical interventions like a Latarjet procedure are often employed to stabilize the shoulder, influencing treatment decisions.
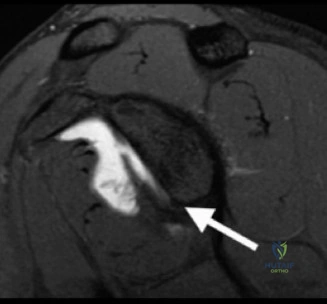
A 19-year-old rugby player presents with recurrent anterior shoulder instability. You are reviewing his imaging. Describe the pathomechanics of this "inverted pear" morphology shown in the radiograph and explain its clinical significance in your management planning.
Candidate: The "inverted pear" glenoid represents significant anteroinferior bone loss. This changes the glenoid from its natural shape to one where the inferior diameter is narrowed. It is clinically significant because it reduces the glenoid arc length, making the joint prone to recurrent dislocation even after soft-tissue repair. I would use the ISIS score to decide between a Bankart repair and a bony augmentation like a Latarjet.
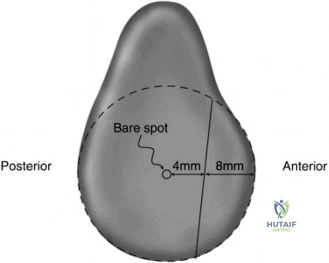
Failing to mention the "concavity-compression" mechanism or the "glenoid track." Candidates often focus only on the Bankart lesion and forget that bone loss is now recognized as a primary driver of surgical failure. They also often fail to mention quantifying the bone loss with 3D CT.
The "inverted pear" glenoid indicates a loss of the anteroinferior osseous buttress, which is the primary restraint to anterior translation in abduction and external rotation. This bone loss compromises the concavity-compression mechanism. Biomechanically, it narrows the 'Glenoid Track,' potentially rendering a Hill-Sachs lesion 'off-track.' I would quantify this using 3D CT en-face views (best-fit circle or Pico method). Given the patient is a young collision athlete, if bone loss exceeds 15-20% or if the lesion is 'off-track,' I would advocate for a Latarjet procedure rather than an isolated Bankart repair to restore the articular arc and provide the dynamic sling effect of the conjoined tendon.
You have decided to proceed with an open Latarjet procedure. Please detail the anatomical structures at risk during the approach and how you specifically protect them during the surgical steps.
Candidate: The main structures at risk are the musculocutaneous nerve and the axillary nerve. The musculocutaneous nerve is at risk during coracoid mobilization and retraction. The axillary nerve is at risk during capsular release. I would identify them carefully and retract gently.
Giving a generic description without mentioning the "safe zone" for the musculocutaneous nerve (3-8cm distal to the coracoid) or failing to explain the specific surgical steps where the risk is highest, such as the subscapularis split or the inferior capsular release.
The primary neurovascular risk is the musculocutaneous nerve, which typically enters the conjoined tendon 3-8cm distal to the coracoid tip. I protect it by staying strictly extra-articular and using blunt dissection during medial mobilization of the coracoid. I avoid excessive medial retraction on the conjoined tendon. During glenoid exposure, the axillary nerve is at risk inferiorly; I protect this by staying close to the glenoid neck and avoiding excessive inferior retraction. I also prefer a subscapularis splitting approach, which maintains the dynamic muscle function while allowing sufficient exposure without formal detachment.
Look at this intraoperative image. What is the critical error to avoid regarding graft positioning, and what are the long-term consequences if this is not achieved?
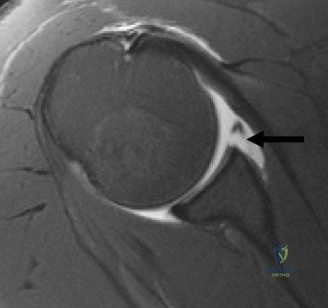
Candidate: The graft must not be placed too laterally. If it protrudes, it causes the humeral head to rub against the bone block, leading to early osteoarthritis.
Not mentioning the "flush" or "slightly medial" requirement. Simply saying "don't put it too far out" is insufficient. A high-level candidate must address the articular congruency.
The graft must be positioned flush with, or slightly medial to (within 1mm), the articular surface of the glenoid. If placed too laterally, it creates an intra-articular block that causes secondary glenohumeral osteoarthritis due to mechanical impingement. Conversely, if placed too medially, the bony blocking effect is lost. Additionally, the inferior surface of the graft must be decorticated to ensure bleeding cancellous bone contacts the glenoid to facilitate bony union. Rigid fixation with two screws is essential to prevent rotation.
