Recurrent Anterior Shoulder Instability in Elite Athletes: A Diagnostic Case Study
Key Takeaway
Diagnosing recurrent anterior shoulder instability, especially in athletes like rugby players, involves a thorough clinical exam, including apprehension and relocation tests. Crucial imaging includes CT for quantifying glenoid bone loss and Hill-Sachs lesions, and MRA to assess labral tears and capsular laxity. These findings guide precise surgical planning for return to sport.
A 28-year-old rugby player presents with a 18-month history of recurrent anterior shoulder instability, failing conservative management. He has had three dislocations since his initial injury. He is currently limited by apprehension and pain. How would you categorize his instability and what are the critical components of your clinical assessment?
Candidate: I would characterize this as chronic traumatic anterior instability. My assessment would start with a thorough history focusing on the number of dislocations and the demands of his sport. Examination would involve range of motion, neurovascular status, and provocative testing like the Apprehension, Relocation, and Load-and-Shift tests. I would also assess for hyperlaxity using the Beighton score.
The candidate focuses only on the shoulder exam. Failing to explicitly mention the neurovascular check (axillary/musculocutaneous nerve) or ignoring the distinction between traumatic (Bankart) and atraumatic (MDI/laxity) patterns marks a lack of clinical rigour.
I would approach this by confirming the "TUBS" (Traumatic, Unidirectional, Bankart, Surgery) classification. Key assessment components include: 1) Clinical history (injury mechanism, recurrence frequency). 2) Stability testing (Apprehension/Relocation/Surprise tests). 3) Laxity assessment (Beighton score to rule out MDI). 4) Strict neurovascular documentation (specifically axillary and musculocutaneous nerve integrity). 5) Assessing for apprehension at specific vectors to define the structural instability.
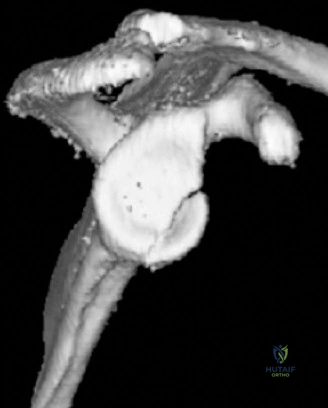
You have reviewed his imaging. This radiograph (Grashey/Axillary) shows signs of bone loss. How do you quantify this, and why is it pivotal for his surgical management?

Candidate: On the radiographs, I look for blunting of the anterior-inferior glenoid rim. I would order a CT scan with 3D reconstruction and use the 'best-fit circle' method to quantify bone loss. This is critical because if he has significant bone loss—usually cited as >15%—an arthroscopic Bankart repair will likely fail, and he would require a bone-block procedure.
Failing to mention the concept of "bipolar" bone loss (glenoid + humeral Hill-Sachs). Focusing solely on the glenoid while ignoring the Hill-Sachs lesion and the "Glenoid Track" paradigm will fail the candidate in the exam.
Quantification requires a CT with 3D reconstruction using the 'Pico' (best-fit circle) method. I must then evaluate the 'Glenoid Track' paradigm: I compare the functional glenoid track width against the Hill-Sachs interval. If the Hill-Sachs lesion is 'off-track,' it engages the anterior glenoid, acting as a fulcrum for re-dislocation. This dictates the shift from soft-tissue stabilization to bone-grafting augmentation (e.g., Latarjet) to restore the articular arc and the sling effect of the conjoint tendon.
Given the patient is a high-level rugby player with significant bone loss, explain the "Triple-Blocking Effect" of the Latarjet procedure and why it is superior to a soft-tissue Bankart repair in this context.
Candidate: The Latarjet procedure provides a bone block by increasing the glenoid surface area, which helps prevent dislocation. The conjoint tendon provides a sling effect when the arm is in abduction and external rotation. Finally, the capsule is repaired to the CA ligament stump, which stabilizes the joint further.
Describing the procedure vaguely without referencing the specific pathology of "engaging" lesions or failing to name the "Patte" triple-block classification. Not addressing why a standard soft-tissue repair is insufficient (ISIS score > 3).
The Latarjet procedure provides the triple-blocking effect: 1) Bone Block: Extending the glenoid articular arc, converting off-track lesions to on-track. 2) Sling Effect: The conjoint tendon (short head of biceps and coracobrachialis) creates a dynamic muscular barrier to anterior translation in abduction/external rotation. 3) Capsular Repair: Attaching the CA ligament stump to the anterior capsule reconstructs the capsulolabral complex. In a high-demand contact athlete with significant osseous deficiency (ISIS score of 7), isolated arthroscopic soft-tissue repair is biomechanically insufficient to handle the sport-specific loads.
