Crack the Case: Bony Bankart Hillsachs Shoulder Injuries
Key Takeaway
Your ultimate guide to Crack the Case: Bony Bankart Hillsachs Shoulder Injuries starts here. Traumatic anterior shoulder instability is common in young athletes, carrying a high recurrence risk. Recurrent episodes significantly increase arthritis risk, mandating aggressive treatment. Comprehensive evaluation for persistent instability often includes assessing for critical bony defects, such as a **bony bankart hillsachs** lesion, which are key determinants for effective management and preventing future dislocations.
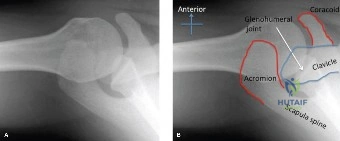
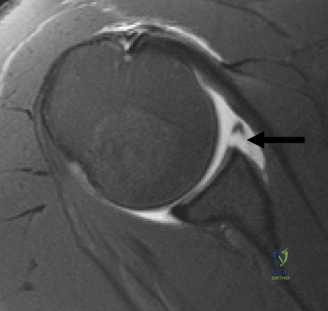
A 28-year-old rugby player presents with a traumatic anterior shoulder dislocation. Following reduction, radiographs show a bony Bankart lesion and a Hill-Sachs impaction. Given the patient’s demographic and high-demand sporting goals, what is your approach to assessing the risk of recurrent instability, and what specific clinical decision-making tool do you use to guide your management?
Candidate: I would perform a thorough clinical exam, including apprehension and relocation tests. Given his high-energy trauma and collision sport participation, I would calculate the Instability Severity Index Score (ISIS). Factors include age, sporting level, hyperlaxity, and radiographic signs of bone loss. A score over 6 typically indicates that an arthroscopic soft-tissue repair is insufficient, and a bony procedure, like a Latarjet, is preferred.
Candidates often fail to explicitly mention the "Glenoid Track" concept. Relying solely on the ISIS score without mentioning the biomechanical interaction of the humeral head defect (Hill-Sachs) with the glenoid (Glenoid Track) is considered an incomplete answer for an elite-level exam.
The candidate must define the risk using a dual approach: 1) The ISIS Score to predict the risk of failure for soft-tissue repair (Age, Contact Sport, Hyperlaxity, Hill-Sachs, Bony Bankart). 2) The Glenoid Track Paradigm: Calculating the track width and determining if the Hill-Sachs lesion is "on-track" or "off-track." If the lesion is off-track, the humeral head engages the glenoid, necessitating a bony augmentation (e.g., Latarjet) to restore the anterior glenoid arc.
The decision is made to proceed with a Latarjet procedure. During the intraoperative exposure and coracoid preparation, what are the critical anatomical landmarks and safety steps required to ensure a successful graft placement and avoid iatrogenic injury?
Candidate: I would perform a deltopectoral approach, identify the cephalic vein, and expose the coracoid. I need to preserve the CA ligament for later capsular repair. The coracoid must be decorticated. During subscapularis splitting, I must protect the axillary nerve. The graft should be fixed flush to the glenoid surface to avoid arthritis.
Neglecting to mention the Musculocutaneous nerve. Candidates often focus on the graft but forget that the nerve enters the coracobrachialis 3-5cm distal to the coracoid tip, making it highly vulnerable to retraction injury during the procedure.
A structured surgical response: 1) Exposure: Protect cephalic vein, identify conjoint tendon, release pectoralis minor. 2) Safety: Be aware of the musculocutaneous nerve 3-5cm distal to the coracoid. 3) Graft Prep: Decorticate the undersurface to ensure union. 4) Fixation: Use the "triple-blocking" effect (Bone block, Sling effect, Capsular repair). 5) Critical technical point: Ensure the graft is flush with the cartilage; if "proud," it will cause catastrophic chondrolysis.
Post-operatively, the patient is progressing well. However, you must explain to him why he cannot return to full contact rugby immediately, even if he feels strong. What is your rationalization based on the pathophysiology of the bone graft union and the "Sling Effect"?

Candidate: I would explain that the bone graft needs time to unite with the glenoid neck. Until it is osseously integrated, the construct is fragile. The "Sling Effect" provided by the conjoint tendon also needs the subscapularis and surrounding soft tissues to heal to provide dynamic stability.
Providing a vague timeframe (e.g., "6 months") without explaining the *reasoning*—specifically, the need for radiographic confirmation of graft union and the risk of stress shielding or hardware failure during high-impact loading before biological healing occurs.
The candidate should synthesize the biological and mechanical requirements: 1) Biological: Osseous union is mandatory; return to play requires radiographic proof of graft integration to avoid non-union. 2) Mechanical: The "Sling Effect" requires the conjoint tendon to be under proper tension; early aggressive loading can stretch or disrupt the repair. 3) Functional: Must meet strict criteria: 90% strength recovery in rotator cuff/deltoid and successful functional sport-specific testing to minimize the risk of recurrent dislocation in a high-risk collision environment.
