

Introduction and Epidemiology
Recurrent anterior shoulder instability remains one of the most challenging pathologies in orthopedic sports medicine, particularly in the young, athletic population. The glenohumeral joint, characterized by a large humeral head articulating with a relatively shallow and small glenoid fossa, sacrifices inherent osseous stability for a maximal functional arc of motion. Consequently, it is the most frequently dislocated major joint in the human body, with anterior dislocations accounting for approximately 95 percent of all glenohumeral instability events.
Epidemiological data indicates an incidence rate of primary shoulder dislocations ranging from 24 to 56 per 100,000 person-years, with a significant predilection for males in their second and third decades of life engaged in contact sports. The natural history of a primary anterior dislocation in this demographic is notoriously associated with a high rate of recurrence. Studies have demonstrated that patients under the age of 20 face a recurrence rate approaching 90 percent with non-operative management.
Recurrent instability inevitably leads to progressive structural damage, most notably bipolar bone loss. Each subsequent dislocation event exacerbates capsuloligamentous attenuation, anterior glenoid rim erosion, and impaction fracturing of the posterosuperior humeral head. The recognition and accurate quantification of this combined osseous deficiency—the Hill-Sachs lesion and anterior glenoid bone loss—are paramount. Failure to address bipolar bone loss is the leading cause of surgical failure following isolated arthroscopic soft-tissue stabilization. Therefore, a comprehensive diagnostic approach and a tailored surgical strategy are essential to restore joint kinematics, prevent recurrent instability, and mitigate the onset of dislocation arthropathy.
Clinical Presentation and Diagnostic Evaluation
Patient Presentation and History
A 28-year-old right-hand dominant male presented to the emergency department following a high-energy fall during a rugby match. The mechanism of injury involved direct impact to the posterior aspect of the shoulder while the arm was abducted and externally rotated, resulting in a forceful anterior dislocation. He reported immediate, severe pain in the left shoulder, complete loss of function, and a visible deformity. This was his third episode of anterior glenohumeral dislocation on the left side within 18 months, with the previous two occurring during sports activities and successfully reduced in the emergency department. He denied any significant pre-existing shoulder pathology, systemic diseases, or bleeding diatheses. His medical history was otherwise unremarkable, with no known allergies and no regular medications. Social history included active participation in competitive contact sports and no tobacco or illicit drug use.
Clinical Examination
Upon initial assessment, the patient was in acute distress, cradling his left arm.
* Inspection: Marked deformity of the left shoulder was evident, characterized by a flattened deltoid contour anteriorly and laterally, with a prominent acromion. There was a palpable sulcus beneath the acromion anteriorly, and the humeral head was palpable anteriorly beneath the coracoid process, consistent with an anterior glenohumeral dislocation. No open wounds or ecchymoses were noted initially, though mild swelling was present.
* Palpation: Tenderness was localized globally around the shoulder joint, with exquisite pain upon any attempted movement. The humeral head was distinctly palpable in the anterior subcoracoid position. Crepitus was not elicited.
* Range of Motion: Actively, the patient had zero range of motion due to pain. Passively, any attempt to move the glenohumeral joint was met with significant resistance and severe pain, confirming a locked dislocation.
* Neurological Assessment: A thorough neurovascular examination was performed prior to any reduction attempts. Axillary nerve function was assessed by sensation over the regimental badge area and deltoid contraction (if possible), which was diminished but not absent. Musculocutaneous, median, ulnar, radial, and suprascapular nerve functions were intact distally.
* Vascular Assessment: Distal pulses (radial, ulnar) were strong and symmetric bilaterally. Capillary refill was brisk in all digits. No pallor or paresthesias were present in the hand or forearm.
Given the history of recurrent dislocations and the mechanism of injury, a high index of suspicion for associated bony and soft tissue lesions, including a critical Hill-Sachs lesion and anterior glenoid bone loss, was established.
Imaging and Diagnostics
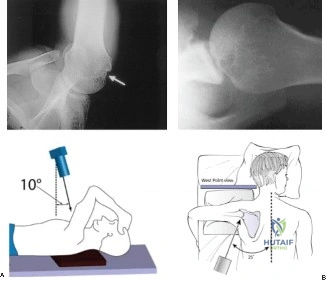
Initial imaging in the emergency department confirmed an anterior glenohumeral dislocation and allowed for assessment of associated bony pathology.
- X-rays: A standard shoulder series including AP, Y-scapular, and axillary views was obtained.
- The AP view demonstrated the humeral head dislocated inferior and medial to the glenoid, lying beneath the coracoid.
- The Y-scapular view unequivocally confirmed the anterior displacement of the humeral head relative to the glenoid and coracoid.
- The axillary view (or a Velpeau view if an axillary view was too painful or difficult to obtain) provided crucial information regarding the presence and extent of bony defects.

Initial AP radiograph demonstrating an anterior glenohumeral dislocation of the left shoulder.
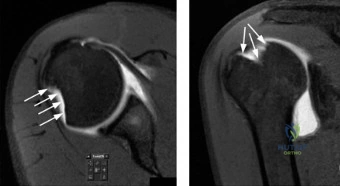
Following successful closed reduction under conscious sedation, post-reduction X-rays were obtained to confirm concentric reduction and re-evaluate for occult fractures or persistent bony defects. A large, impression fracture on the posterosuperior aspect of the humeral head—a Hill-Sachs lesion—was clearly delineated, prompting further advanced imaging to quantify bipolar bone loss.
Surgical Anatomy and Biomechanics
Osseous Anatomy of the Glenohumeral Joint
The glenohumeral joint is a multiaxial ball-and-socket synovial joint. The glenoid fossa is pear-shaped, being wider inferiorly than superiorly. The articular surface of the glenoid covers only approximately one-third of the humeral head articular surface at any given time. The osseous anatomy provides minimal inherent constraint, relying heavily on dynamic and static soft-tissue stabilizers. The anterior rim of the glenoid is particularly susceptible to attritional bone loss or acute fracture (bony Bankart lesion) during an anterior dislocation event.
Capsuloligamentous Stabilizers
The static stabilizers include the glenoid labrum, the joint capsule, and the glenohumeral ligaments (superior, middle, and inferior). The labrum deepens the glenoid socket by approximately 50 percent, increasing the contact area and providing a crucial bumper against humeral head translation. The inferior glenohumeral ligament (IGHL) complex, consisting of an anterior band, a posterior band, and an axillary pouch, is the primary static restraint to anterior translation when the arm is in the vulnerable position of abduction and external rotation. Avulsion of the anterior-inferior labrum and the attached anterior band of the IGHL from the glenoid rim constitutes the classic Bankart lesion.
Dynamic Muscle Stabilizers
Dynamic stability is conferred by the rotator cuff musculature, the long head of the biceps tendon, and the periscapular muscles. The rotator cuff compresses the humeral head into the glenoid concavity throughout the arc of motion, a mechanism known as concavity compression. In the setting of structural capsulolabral deficiency, the dynamic stabilizers are easily overwhelmed, leading to recurrent subluxation or dislocation.
Biomechanics of Bipolar Bone Loss
The biomechanical interaction between a Hill-Sachs lesion and anterior glenoid bone loss is best conceptualized through the "glenoid track" paradigm. The glenoid track is the zone of contact between the humeral head and the glenoid during maximum abduction and external rotation. Its width is calculated as 83 percent of the intact inferior glenoid width.
When anterior glenoid bone loss occurs, the width of the glenoid track decreases proportionally. If a Hill-Sachs lesion extends medially beyond the medial margin of this narrowed glenoid track, it is classified as an "off-track" lesion. An off-track Hill-Sachs lesion will engage the anterior rim of the glenoid during abduction and external rotation, levering the humeral head out of the socket and causing a dislocation. Conversely, an "on-track" lesion remains contained within the articular surface contact zone and does not engage. Understanding this biomechanical interplay is the cornerstone of contemporary surgical decision-making.
Indications and Contraindications
The decision-making process for managing recurrent anterior shoulder instability hinges on patient-specific factors, activity level, and the precise quantification of structural damage. The Instability Severity Index Score (ISIS) is frequently utilized to predict the risk of recurrence following arthroscopic Bankart repair, factoring in age, sport type, competitive level, hyperlaxity, and bone loss.
Operative Versus Non Operative Management
| Management Strategy | Indications | Contraindications |
|---|---|---|
| Non-Operative Management | First-time dislocation in older, low-demand patients; In-season athletes requiring immediate return to play (with brace); Patients with unacceptable surgical risk. | Recurrent instability with significant bone loss; Young, competitive contact athletes (relative contraindication for non-operative approach). |
| Arthroscopic Bankart Repair | On-track Hill-Sachs lesions; Glenoid bone loss < 13.5%; First-time dislocators in high-demand sports; Intact capsular tissue. | Off-track Hill-Sachs lesions; Glenoid bone loss > 13.5-15%; Poor tissue quality (e.g., Ehlers-Danlos syndrome); High ISIS score (>6). |
| Arthroscopic Bankart with Remplissage | Off-track Hill-Sachs lesions with minimal glenoid bone loss (< 13.5%); Revision stabilization without critical glenoid bone loss. | Critical glenoid bone loss (> 13.5-15%); Overhead throwing athletes (due to potential loss of external rotation). |
| Open Latarjet Procedure | Critical glenoid bone loss (> 15%); Off-track Hill-Sachs lesions; Revision of failed arthroscopic stabilization; High-demand contact athletes (e.g., rugby, martial arts). | Advanced glenohumeral osteoarthritis; Active joint infection; Coracoid hypoplasia or prior coracoid resection. |
| Distal Tibial Allograft Reconstruction | Massive glenoid bone loss (> 25-30%); Failed Latarjet procedure; Chronic locked anterior dislocations. | Active infection; Severe neurovascular compromise; Uncorrectable rotator cuff arthropathy. |
Pre Operative Planning and Patient Positioning
Advanced Imaging and Bone Loss Quantification
Accurate preoperative planning necessitates advanced imaging to quantify bone loss. While plain radiographs provide an initial assessment, non-contrast Computed Tomography (CT) with 3D reconstructions is the gold standard for evaluating osseous architecture.
The Pico method is widely employed to measure anterior glenoid bone loss on en face 3D CT views. A best-fit circle is drawn over the inferior portion of the intact glenoid (or the contralateral normal glenoid for comparison), and the area or width of the missing anterior bone is calculated as a percentage of the total circle.
Magnetic Resonance Imaging (MRI) or MR arthrography is essential for evaluating soft tissue structures, including the labrum, capsule, rotator cuff, and articular cartilage. MRI also allows for the measurement of the Hill-Sachs interval and the application of the glenoid track concept.
Patient Positioning and Anesthesia
Surgical intervention is typically performed under general anesthesia, often supplemented with an interscalene regional nerve block to minimize volatile anesthetic requirements and optimize postoperative pain control.
Positioning depends on the planned procedure and surgeon preference.
* Beach Chair Position: Preferred by many for open procedures (Latarjet) and arthroscopic Bankart repairs. It allows for an anatomical view of the shoulder, easy conversion from arthroscopy to an open approach, and excellent access to the anterior structures.
* Lateral Decubitus Position: Frequently utilized for arthroscopic procedures. It provides excellent joint distraction via longitudinal and lateral traction, facilitating access to the inferior capsule and labrum. However, it requires careful padding of all bony prominences to prevent neuropraxia.
Detailed Surgical Approach and Technique
Arthroscopic Bankart Repair and Remplissage
For patients with an off-track Hill-Sachs lesion but subcritical glenoid bone loss (< 13.5%), an arthroscopic Bankart repair combined with a remplissage procedure is highly effective.
Diagnostic Arthroscopy and Preparation:
Standard posterior, anterior-inferior, and anterior-superior portals are established. A thorough diagnostic arthroscopy is performed to assess the extent of the capsulolabral tear (Bankart lesion) and evaluate the Hill-Sachs defect.
The anterior labrum and capsule are meticulously mobilized from the anterior glenoid neck using an elevator and electrocautery. It is critical to release the tissue inferiorly to the 6 o'clock position to allow for adequate superior shift during repair. The anterior glenoid neck is decorticated using a motorized burr to create a bleeding bone bed, optimizing biological healing of the repaired labrum.
The Remplissage Procedure:
Before tying the anterior Bankart anchors, the remplissage is addressed. Viewing from the anterior-superior portal, the arthroscope is directed posteriorly to visualize the Hill-Sachs lesion. The defect is debrided of fibrous tissue. One or two suture anchors (depending on the size of the defect) are percutaneously placed into the depth of the Hill-Sachs lesion via a posterolateral accessory portal. The sutures are passed through the overlying infraspinatus tendon and posterior capsule. These sutures are left untied until the anterior repair is complete.
Anterior Bankart Repair:
Suture anchors (typically 2.4mm to 3.0mm in diameter) are placed sequentially along the anterior glenoid rim, starting inferiorly at the 5:30 position and progressing superiorly to the 3:00 position. Sutures are passed through the capsulolabral complex using a suture-passing device, ensuring a healthy bite of the inferior glenohumeral ligament to achieve a superior and lateral capsular shift. The knots are tied, restoring the anterior bumper.
Finally, the arm is placed in neutral rotation, and the posterior remplissage sutures are tied blindly in the subdeltoid space. This tenodesis of the infraspinatus and posterior capsule into the defect converts an off-track lesion into an extra-articular on-track lesion, preventing engagement.
Open Latarjet Procedure
The Latarjet procedure is the workhorse for recurrent instability associated with critical glenoid bone loss (> 15%) or in high-demand contact athletes. It relies on a triple-blocking effect: the osseous augmentation of the glenoid, the dynamic sling effect of the conjoint tendon traversing the subscapularis, and the capsular repair to the coracoacromial ligament stump.
Approach and Coracoid Harvest:
A 5 to 7 cm deltopectoral incision is made, extending distally from the tip of the coracoid process. The cephalic vein is identified and retracted laterally with the deltoid. The clavipectoral fascia is incised, exposing the coracoid and the conjoint tendon. The coracoacromial ligament is sharply released from the lateral aspect of the coracoid, leaving a 1 cm stump for later capsular repair. The pectoralis minor tendon is released from the medial aspect of the coracoid.
An angled osteotomy is performed at the base of the coracoid process using an oscillating saw or curved osteotome, yielding a bone graft approximately 2.5 to 3 cm in length. The inferior surface of the coracoid graft is decorticated to expose bleeding cancellous bone. Two drill holes are created centrally in the graft to accommodate the fixation screws.
Subscapularis Split and Glenoid Preparation:
The subscapularis is exposed. A longitudinal split is created in the subscapularis tendon, typically at the junction of the superior two-thirds and inferior one-third, to protect the axillary nerve traversing inferiorly. The underlying capsule is incised vertically, exposing the anterior glenoid. A Fukuda retractor is placed to displace the humeral head posteriorly. The anterior glenoid neck is aggressively decorticated to flat, bleeding bone to ensure maximal graft-to-host bone contact.
Graft Fixation:
The prepared coracoid graft is passed through the subscapularis split. It is positioned flush with, or slightly medial (1-2 mm) to, the articular cartilage of the anterior glenoid rim. Positioning the graft lateral to the cartilage risks severe osteoarthritis, while placing it too medial negates the osseous blocking effect.
The graft is provisionally fixed with K-wires. Two 3.75 mm or 4.0 mm partially threaded cannulated screws are inserted over the K-wires to achieve rigid bicortical compression. Finally, the native capsule is repaired to the stump of the coracoacromial ligament, rendering the graft extra-articular.
Distal Tibial Allograft Reconstruction
In cases of massive glenoid bone loss (> 25%) or failed Latarjet procedures, a structural distal tibial allograft is indicated. The lateral aspect of the distal tibia provides a highly congruent articular match for the glenoid.
The approach is identical to the Latarjet. The allograft is fashioned to match the precise dimensions of the glenoid defect based on preoperative 3D CT planning. The graft is positioned to restore the anatomic contour of the glenoid and fixed with two bicortical screws. Because there is no conjoint tendon transfer, this procedure relies entirely on the restoration of the articular arc and the static capsular repair.
Complications and Management
Surgical management of recurrent anterior instability carries inherent risks. The incidence and type of complications vary significantly between arthroscopic soft-tissue procedures and open osseous augmentations.
Intraoperative Complications
Intraoperative complications during arthroscopy include anchor pullout, poor tissue quality precluding adequate repair, and iatrogenic cartilage damage. During open procedures like the Latarjet, neurovascular injury is a paramount concern. The musculocutaneous nerve enters the conjoint tendon as proximally as 3 to 5 cm distal to the coracoid tip and is at risk during graft harvest and retraction. The axillary nerve is at risk during the inferior capsular release and subscapularis split.
Postoperative Complications
| Complication | Estimated Incidence | Etiology / Risk Factors | Management / Salvage Strategy |
|---|---|---|---|
| Recurrent Instability | 5-15% (Bankart); 2-5% (Latarjet) | Unrecognized bone loss; technical failure; non-compliance; high-energy trauma. | Revision to Latarjet (if failed Bankart); Distal Tibial Allograft or Eden-Hybinette (if failed Latarjet). |
| Hardware Failure / Non-union | 2-7% (Latarjet) | Poor graft preparation; inadequate compression; smoking; over-tightening of screws. | Conservative management if stable; Revision fixation with bone grafting if symptomatic non-union. |
| Neurologic Injury | 1-3% | Traction neuropraxia (musculocutaneous, axillary); direct laceration. | Observation and EMG at 3 months; Surgical nerve exploration if no recovery and confirmed complete lesion. |
| Glenohumeral Osteoarthritis | 10-20% (Long-term) | Lateral graft overhang (Latarjet); over-tightening of capsule; natural history of trauma. | NSAIDs, intra-articular injections; Total Shoulder Arthroplasty in older patients with advanced disease. |
| Infection | < 1% | Prolonged surgical time; open procedures; poor host factors. | Prompt surgical debridement (I&D); culture-specific intravenous antibiotics; hardware retention if early. |
Post Operative Rehabilitation Protocols
Successful outcomes rely heavily on strict adherence to a phased postoperative rehabilitation protocol. The goals are to protect the surgical repair, gradually restore range of motion, and progressively strengthen the dynamic stabilizers.
Early Protective Phase
Weeks 0 to 4: The patient is immobilized in a sling with an abduction pillow. For arthroscopic Bankart repairs, the arm is kept in slight internal rotation. For Latarjet procedures, neutral rotation is maintained to relieve tension on the conjoint tendon. Cryotherapy is utilized for pain and edema control. Rehabilitation is limited to active range of motion of the elbow, wrist, and hand. Passive forward elevation is permitted up to 90 degrees, and external rotation is strictly limited to 0 degrees to protect the anterior capsular repair and the subscapularis split.
Intermediate Mobilization Phase
Weeks 4 to 8: The sling is discontinued. The primary goal is the gradual restoration of passive and active-assisted range of motion. Forward elevation is progressed to full as tolerated. External rotation is gradually increased by 10 to 15 degrees per week, aiming for 45 degrees by week 6. Submaximal isometric strengthening of the rotator cuff and deltoid is initiated. Scapular stabilization exercises (retraction, depression) are emphasized to prevent compensatory dyskinesia.
Advanced Strengthening and Return to Play
Weeks 8 to 16: Active range of motion is normalized. Isotonic strengthening of the rotator cuff, periscapular musculature, and conjoint tendon (in Latarjet patients) is progressed. Proprioceptive training and closed kinetic chain exercises are introduced.
Months 4 to 6: Sport-specific training begins. Return to competitive contact sports is generally permitted between 5 to 6 months postoperatively, contingent upon achieving full, painless range of motion, symmetrical strength (at least 90% of the contralateral limb on isokinetic testing), and radiographic evidence of coracoid graft union in Latarjet patients.
Summary of Key Literature and Guidelines
The evolution of surgical management for anterior shoulder instability is deeply rooted in landmark orthopedic literature.
Burkhart and De Beer's seminal work introduced the concept of the "inverted pear" glenoid, demonstrating that arthroscopic Bankart repair in the presence of significant anterior glenoid bone loss results in an unacceptably high recurrence rate (up to 67%). This established the absolute necessity of evaluating osseous defects prior to soft-tissue stabilization.
Itoi et al. revolutionized the biomechanical understanding of bipolar bone loss by describing the "glenoid track." Their research provided a reproducible, quantitative method to determine whether a Hill-Sachs lesion will engage the glenoid rim, fundamentally shifting the paradigm from measuring isolated defects to assessing the interaction between the humeral head and glenoid.
Boileau et al. popularized the Instability Severity Index Score (ISIS), providing a validated preoperative tool to guide surgical decision-making. Furthermore, their work on the arthroscopic remplissage technique demonstrated excellent clinical outcomes and low recurrence rates for patients with off-track Hill-Sachs lesions and subcritical glenoid bone loss, offering a viable alternative to open osseous augmentation in appropriately selected patients.
Recent consensus guidelines emphasize that the threshold for "critical" bone loss is lowering. While historically defined as > 20% to 25%, modern literature suggests that "subcritical" bone loss between 13.
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding shoulder-and-elbow-cases-hillsachs-lesion