Arthroscopic Bankart Repair: A Masterclass in Anterior Shoulder Stabilization

Key Takeaway
Welcome, fellows, to an immersive masterclass in arthroscopic Bankart repair for anterior shoulder instability. We'll meticulously cover patient selection, preoperative planning, precise intraoperative techniques including portal placement, diagnostic arthroscopy, labral repair, and suture management. Learn critical anatomy, avoid pitfalls, and ensure optimal outcomes for your patients. This session provides a granular, surgeon's-eye view from incision to closure.
Comprehensive Introduction and Patho-Epidemiology
Welcome to the operating theater, colleagues. Today, we confront one of the most ubiquitous yet biomechanically complex challenges in sports medicine: anterior glenohumeral instability. The evolution of anterior shoulder stabilization has transitioned dramatically from the open procedures pioneered by Bankart and Rowe to the sophisticated, minimally invasive arthroscopic techniques we employ today. However, this transition is not merely a change in surgical approach; it demands a profound, three-dimensional understanding of the intricate balance between mobility and stability that defines the human shoulder. The goal in the modern era is no longer simply to prevent dislocation through non-anatomic constraint, but to restore precise anatomic kinematics, optimize joint proprioception, and facilitate a reliable return to elite-level function without sacrificing critical ranges of motion.
Anterior glenohumeral instability represents a wide spectrum of pathology, ranging from subtle, activity-limiting microinstability in the overhead athlete to frank, recurrent dislocations in the collision athlete. To navigate this successfully, the orthopedic surgeon must first rigorously differentiate between physiologic laxity and pathologic instability. Laxity is a physiologic, asymptomatic translation of the humeral head on the glenoid, often symmetric and inherently linked to the patient's individual collagen makeup and genetics. Instability, conversely, is a pathologic state where this translation becomes symptomatic, leading to pain, apprehension, subluxation, or complete dislocation. The epidemiological burden of this pathology is substantial, particularly among young, active males. The recurrence rate following a primary traumatic dislocation in a patient under the age of twenty approaches 90% if treated non-operatively. This unacceptably high failure rate underscores the absolute imperative for early, definitive surgical intervention in the appropriate demographic to prevent progressive chondral damage and irreversible bone loss.
The classic mechanism of injury involves a forceful, catastrophic application of an external rotation and abduction moment to the arm. This leverages the humeral head out of the shallow glenoid concavity, violently loading the anterior capsuloligamentous restraints. This trauma predictably yields the Bankart lesion, the fundamental pathoanatomic hallmark of anterior instability. Originally described by Arthur Sydney Blundell Bankart, this lesion is defined as the avulsion of the anteroinferior labrum and its attached inferior glenohumeral ligament (IGHL) complex from the anterior glenoid rim. Present in up to 90% of traumatic anterior dislocations, the Bankart lesion destroys the essential "bumper" or "chock-block" effect of the labrum and abolishes the critical hammock-like restraint of the IGHL, rendering the joint incompetent.

However, the Bankart lesion rarely exists in a vacuum. The kinetic energy of a dislocation is frequently dissipated through adjacent osseous and soft tissue structures, leading to a constellation of associated pathologies that must be meticulously identified prior to any surgical intervention. The Hill-Sachs lesion, an impaction fracture of the posterosuperior humeral head created as it levers against the hard, dense anterior glenoid rim during dislocation, is present in the vast majority of recurrent cases.

Furthermore, the anterior glenoid rim itself may fracture or chronically erode, resulting in a bony Bankart lesion and transforming the normal pear-shaped glenoid into an "inverted pear" morphology. Other vital pathoanatomic variants include the ALPSA (Anterior Labroligamentous Periosteal Sleeve Avulsion) lesion, where the torn labrum heals medially and inferiorly along the glenoid neck, and the elusive HAGL (Humeral Avulsion of the Glenohumeral Ligaments) lesion. If a HAGL lesion is missed during diagnostic arthroscopy, it represents a guaranteed source of surgical failure, as the capsular hammock remains detached from its humeral insertion.

Detailed Surgical Anatomy and Biomechanics
Mastery of arthroscopic stabilization is entirely predicated upon an intimate, three-dimensional comprehension of shoulder anatomy and biomechanics. The glenohumeral joint is inherently unstable, often likened to a golf ball sitting on a tee, or a seal balancing a ball on its nose. The articular surface of the humeral head is roughly three to four times the surface area of the shallow glenoid fossa. This profound osseous mismatch permits an unparalleled global range of motion, essential for human upper extremity function, but mandates a heavy, continuous reliance on both dynamic and static soft tissue restraints to maintain concavity compression.
The osteology of the glenoid is a critical factor in the stability equation. The normal glenoid is pear-shaped, being broader inferiorly than superiorly. The concavity of the bare bone is minimal; it is the fibrocartilaginous labrum that deepens the socket by up to 50%, creating a critical "chock-block" effect that resists shear forces. When glenoid bone loss occurs, whether through acute impaction fracture or chronic attritional wear from recurrent subluxations, the track upon which the humeral head articulates is dangerously narrowed. If this bone loss exceeds critical thresholds—historically cited as 20-25%, though recent literature suggests even 13.5% can be subcritical but highly relevant in certain populations—an isolated soft tissue Bankart repair will predictably fail due to the loss of the underlying osseous foundation.

The capsuloligamentous structures serve as the primary static restraints of the shoulder. The most critical of these is the Inferior Glenohumeral Ligament (IGHL) complex. Composed of a distinct anterior band, a posterior band, and an intervening axillary pouch, the IGHL functions as a reciprocal hammock. In the provocative position of abduction and external rotation, the anterior band becomes taut, acting as the primary restraint to anterior translation.

The superior and middle glenohumeral ligaments play secondary, yet important, roles. The SGHL primarily resists inferior translation in adduction, while the MGHL resists anterior translation in the mid-ranges of elevation. The labrum itself not only deepens the socket but serves as the robust, continuous attachment site for these ligaments. Disruption of this labral-ligamentous complex destroys the joint's negative intra-articular pressure (the "suction cup" effect) and allows obligate, pathologic translation of the humeral head.
Dynamic stability is orchestrated by the rotator cuff musculature and the long head of the biceps tendon. The subscapularis anteriorly, and the infraspinatus and teres minor posteriorly, act as a transverse force couple, dynamically compressing the humeral head into the glenoid concavity throughout the arc of motion. Scapular dyskinesia, often secondary to the instability itself or chronic guarding, alters the orientation of the glenoid in space, further compromising stability by uncoupling this dynamic compression. Finally, one must maintain a healthy respect for the neurovascular anatomy. The axillary nerve is the structure at greatest risk during anterior stabilization. It courses inferior to the glenohumeral joint capsule, resting approximately 10 to 12 millimeters from the inferior glenoid rim at the 6 o'clock position. Deep, aggressive capsular releases or errant inferior anchor placement can result in catastrophic iatrogenic injury to this nerve.
Exhaustive Indications and Contraindications
Patient selection is the absolute cornerstone of a successful arthroscopic Bankart repair. The decision to proceed arthroscopically versus utilizing an open approach or a bone-block augmentation (such as a Latarjet procedure or iliac crest bone graft) relies on a complex synthesis of patient demographics, physiological age, activity level, sport-specific demands, and precise quantification of the pathoanatomy. The Instability Severity Index Score (ISIS), originally popularized by Boileau, remains a valuable, albeit evolving, heuristic tool in this decision-making process. It incorporates factors like age under 20, competitive sports participation, contact sports, hyperlaxity, and radiographic evidence of bone loss to predict the risk of recurrence.
The ideal candidate for an arthroscopic Bankart repair is a young patient with a clear history of traumatic anterior dislocation, demonstrating a distinct Bankart or ALPSA lesion on MRI, and possessing intact, robust capsuloligamentous tissue without significant osseous defects. Overhead athletes, such as baseball pitchers, tennis players, or volleyball attackers, are particularly strong candidates for the arthroscopic approach. Open procedures inherently risk a greater loss of external rotation due to the necessary subscapularis management (takedown or split) and the aggressive capsular scarring that inevitably follows open dissection. Preserving the precise micro-kinematics of the throwing shoulder is paramount, making arthroscopy the gold standard in this specific demographic.
Conversely, we must rigorously identify contraindications to the arthroscopic approach to prevent unacceptable failure rates. The primary reason for failure of an arthroscopic Bankart repair is the failure of the surgeon to recognize and adequately address critical bone loss. The concept of the "Glenoid Track," pioneered by Yamamoto and Itoi, is paramount here. If a Hill-Sachs lesion engages the anterior glenoid rim during functional ranges of motion (an "off-track" lesion), a soft-tissue repair alone will predictably fail, as the humeral head will lever out of the joint. In these scenarios, the surgeon must be prepared to augment the repair with an arthroscopic Remplissage (insetting the infraspinatus tendon and posterior capsule into the Hill-Sachs defect to render it extra-articular) or abandon the arthroscopic soft-tissue repair entirely in favor of a coracoid transfer (Latarjet).
Indications and Contraindications Table
| Parameter | Arthroscopic Bankart Repair | Open Bankart / Bone Block (e.g., Latarjet) |
|---|---|---|
| Primary Indications | Traumatic anterior instability in young athletes; Recurrent instability with minimal bone loss; ALPSA/Bankart lesions. | Recurrent instability with critical bone loss; Failed prior arthroscopic stabilization; HAGL lesions (often easier open). |
| Bone Loss (Glenoid) | Subcritical (< 13.5% - 15% of glenoid width). | Critical (> 15-20% of glenoid width) or "Inverted Pear" morphology. |
| Humeral Head (Hill-Sachs) | Non-engaging, off-track lesions; or engaging lesions manageable with arthroscopic Remplissage. | Deep, engaging, "off-track" lesions requiring structural grafting or bone block. |
| Patient Demographics | Overhead athletes (throwers) where preserving maximum external rotation is paramount. | High-demand collision athletes (rugby, American football linemen) with hyperlaxity. |
| Soft Tissue Status | Robust, healthy capsulolabral tissue available for plication. | Poor tissue quality, severe capsular deficiency, or profound multidirectional hyperlaxity. |
| Contraindications | Critical glenoid bone loss; Large engaging Hill-Sachs without Remplissage; Uncontrolled seizure disorder. | Active infection; Medically unfit for surgery; Severe glenohumeral osteoarthritis. |
Pre-Operative Planning, Templating, and Patient Positioning
Surgical excellence is achieved long before the first incision is made, through exhaustive pre-operative planning and templating. The clinical examination must be meticulous and systematic. We look for the classic positive Apprehension and Relocation tests, which are highly specific for anterior instability. The Surprise test (anterior release) further confirms the diagnosis. The Load and Shift test, performed supine to relax the patient, allows the surgeon to grade the degree of translation and assess for concomitant multidirectional laxity. A thorough neurovascular exam is mandatory, specifically documenting axillary and musculocutaneous nerve function prior to any surgical intervention to establish a baseline.
Imaging is the foundation of our surgical templating. Standard radiographs must include a true AP (Grashey) of the glenohumeral joint, a scapular Y view, and an axillary lateral. The West Point axillary view is particularly useful for identifying subtle bony Bankart lesions or attritional anterior rim wear, while the Stryker Notch view profiles the posterolateral humeral head to quantify the Hill-Sachs lesion. However, advanced imaging is non-negotiable in the modern era. Magnetic Resonance Arthrography (MRA) is the gold standard for evaluating the soft tissues, allowing us to identify Bankart, ALPSA, GLAD (Glenolabral Articular Disruption), and HAGL lesions, as well as assessing capsular volume, tissue quality, and concomitant rotator cuff pathology.
If there is any suspicion of bone loss on plain films or MRI, a 3D reconstructed Computed Tomography (CT) scan is mandatory. We utilize the en face view of the glenoid with the humeral head digitally subtracted to precisely calculate the percentage of glenoid bone loss. We typically employ the best-fit circle method over the inferior two-thirds of the glenoid. We then calculate the glenoid track by measuring the width of the Hill-Sachs lesion and comparing it to the remaining intact anterior glenoid bone. This determines if the Hill-Sachs lesion is "on-track" or "off-track," which definitively dictates our surgical algorithm.
Patient positioning is a matter of surgeon preference, with both the lateral decubitus and beach chair positions offering distinct biomechanical and logistical advantages. The lateral decubitus position, utilizing balanced suspension traction (typically 10-15 lbs applied to the operative arm), provides unparalleled distraction of the glenohumeral joint. This offers exceptionally clear visualization of the anteroinferior glenoid and facilitates the crucial inferior-to-superior capsular shift necessary for a robust repair.

Conversely, the beach chair position offers a more anatomic, upright orientation, easier management of the airway by the anesthesia team, and seamless conversion to an open procedure (like a Latarjet) if intraoperative findings necessitate a change in plan. Regardless of the chosen position, meticulous padding of all bony prominences, careful management of traction vectors, and strict avoidance of extreme neck extension or lateral flexion are critical to prevent devastating neuropraxic injuries to the brachial plexus.
Step-by-Step Surgical Approach and Fixation Technique
The arthroscopic Bankart repair is a procedure of millimeters. Precision in portal placement, tissue mobilization, anchor trajectory, and knot security dictates the biomechanical success and longevity of the construct. A poorly executed soft tissue repair will fail regardless of the patient's underlying anatomy.
Diagnostic Arthroscopy and Portal Placement
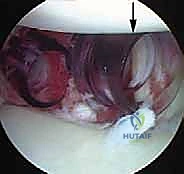
We begin with a standard posterior viewing portal, established approximately 2 cm inferior and 1 cm medial to the posterolateral acromial angle. A thorough, systematic diagnostic sweep is performed. We meticulously document the integrity of the biceps anchor (assessing for SLAP tears), the articular surface of the rotator cuff, the bare area of the humeral head, and the entire 360-degree labral circumference. We specifically probe the anteroinferior labrum to assess the extent of the Bankart detachment and evaluate the volume and patulousness of the axillary pouch.

The establishment of the anterior working portals is arguably the most critical step of the setup; poor portal placement condemns the surgeon to a difficult, compromised repair. Utilizing an outside-in spinal needle localization technique, an anterosuperior portal is created high in the rotator interval, just anterior to the biceps tendon. This serves primarily as a viewing portal for the inferior work and for suture management. The anteroinferior (5 o'clock) portal is then established just superior to the subscapularis tendon. This portal must be placed low enough to allow a 45-degree "deadman's angle" approach to the 5:30 position on the glenoid rim for the foundational inferior anchor.
Tissue Mobilization and Glenoid Preparation
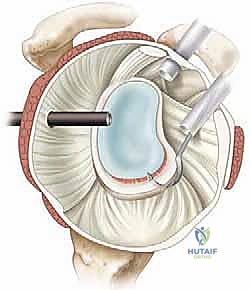
There is an old orthopedic adage: "If it doesn't bleed, it doesn't heal." The fundamental error in novice Bankart repairs is inadequate tissue mobilization. The labrum and capsule are often scarred medially down the glenoid neck, a classic ALPSA variant. Using an arthroscopic elevator, rasp, or radiofrequency ablation wand, the capsulolabral complex must be aggressively elevated off the anterior glenoid neck.


This release must extend inferiorly past the 6 o'clock position (often requiring a switch of the viewing portal to the anterosuperior portal for adequate visualization) and medially until the red muscle belly of the subscapularis is clearly visualized. The tissue must "float" freely, allowing it to be shifted superiorly and laterally onto the glenoid face without any resting tension.
Once mobilized, the anterior glenoid rim is meticulously decorticated using a motorized burr or aggressive rasp. The goal is to remove the eburnated, sclerotic bone and create a bleeding, cancellous bone bed. This optimizes the biological healing environment, allowing the shifted capsulolabral complex to integrate solidly with the osseous glenoid.

Anchor Placement and Suture Passing
Anchor placement begins at the most inferior aspect of the tear, typically at the 5:30 position for a right shoulder. This foundational anchor is the most critical; it dictates the tension of the inferior glenohumeral ligament and the success of the entire shift. The drill guide is introduced through the anteroinferior portal, ensuring a trajectory that bisects the glenoid face to avoid joint penetration (the "deadman's angle"). We utilize modern biocomposite or all-suture anchors, typically 2.4mm to 3.0mm in diameter, to minimize bone removal while maximizing pull-out strength.
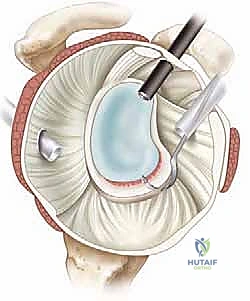
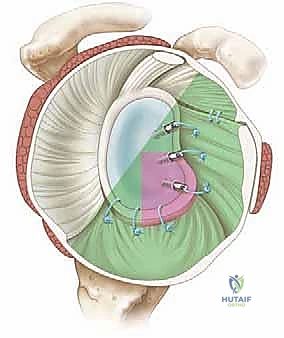
Once the anchor is deployed, suture passing is executed to achieve a distinct inferior-to-superior and medial-to-lateral shift of the capsulolabral tissue. Various passing devices can be utilized, including curved suture lassos or direct penetrating devices. The device is passed through the capsule first, inferior and medial to the anchor, and then through the labrum.


This "pinch" of tissue ensures that when the knot is tied (or the knotless mechanism is tensioned), the capsule is plicated and drawn up onto the articular margin, recreating the essential bumper effect. Subsequent anchors are placed sequentially moving superiorly along the anterior rim, typically at the 4 o'clock and 3 o'clock positions, depending on the extent of the lesion.

Knot Tying, Capsular Plication, and Construct Finalization
If utilizing knotted anchors, arthroscopic knot tying must be precise to avoid creating prominent knot stacks that can abrade the articular cartilage of the humeral head. We typically utilize a sliding, locking knot (such as a Weston or SMC knot) followed by three alternating half-hitches on alternating posts. The post limb must be the one that exits the anchor directly, ensuring the knot sits securely on the labral tissue, compressing it against the decorticated bone bed.


As each knot is tied, the surgeon must visually confirm the restoration of capsular tension and the recreation of the labral bumper. The axillary pouch should appear visibly reduced in volume, and the humeral head should be centralized within the glenoid fossa.


Following the completion of the anterior repair, the joint is re-evaluated. If a significant, engaging Hill-Sachs lesion is present (off-track), an arthroscopic Remplissage is performed concurrently. This involves viewing from the anterior portal, placing 1 or 2 anchors into the Hill-Sachs defect via a posterior portal, and passing the sutures through the infraspinatus tendon and posterior capsule.



Tying these sutures effectively fills the defect, preventing it from engaging the anterior glenoid rim during external rotation and abduction. The final construct is then probed to ensure absolute stability, confirming that the humeral head can no longer be subluxated anteriorly over the newly reconstructed bumper.



Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following arthroscopic Bankart repair can and do occur. The most devastating complication is recurrent instability. Historically, recurrence rates for arthroscopic repairs were higher than open
