Regain Stability: Anterior Shoulder Instability Arthroscopic Fix

Key Takeaway
Looking for accurate information on Regain Stability: Anterior Shoulder Instability Arthroscopic Fix? Anterior shoulder instability is a pathological state where the humeral head abnormally translates on the glenoid, commonly anteroinferiorly, leading to dislocation, impairment, or pain. **Anterior shoulder instability arthroscopic** treatment aims to restore stability by repairing or tightening the damaged capsuloligamentous structures. This minimally invasive surgical approach addresses various causes, including traumatic events, to prevent recurrence.
Comprehensive Introduction and Patho-Epidemiology
Glenohumeral stability is an evolutionary marvel, relying on a sophisticated, synergistic interplay between static and dynamic restraints to permit a globally unparalleled, unconstrained range of motion while resisting pathological translation. Laxity is defined as a strictly physiologic term denoting the asymptomatic, passive translation of the humeral head on the glenoid surface. Conversely, instability represents a pathologic, symptomatic state characterized by abnormal translation of the humeral head on or over the glenoid rim. This pathologic translation inevitably leads to frank dislocation, debilitating functional impairments, or profound pain that precludes athletic or daily activities. The vast majority of glenohumeral instability events occur in the anteroinferior direction, dictated by the inherent biomechanical vulnerabilities of the abducted and externally rotated upper extremity.
The pathogenesis of anterior instability is broadly categorized into traumatic, acquired, and atraumatic etiologies, each demanding a nuanced diagnostic and therapeutic approach. Traumatic anterior instability typically occurs secondary to a discrete, high-energy event with the arm forced into extreme abduction and external rotation, thereby levering the humeral head out of the glenoid fossa. Acquired instability manifests as a more insidious, subtle pathology frequently observed in overhead athletes; it is driven by repetitive microtrauma that progressively attenuates the anterior capsuloligamentous restraints, leading to pathologic subluxation. Atraumatic instability is classically multidirectional, underpinned by generalized ligamentous hyperlaxity, collagen connective tissue disorders, and inherent anatomic variations such as glenoid hypoplasia or excessive retroversion.



The natural history of glenohumeral dislocation underscores the critical necessity of timely and appropriate intervention, as the condition affects approximately 2% of the general population, with a striking 9:1 male-to-female ratio in the 21- to 30-year-old demographic. Long-term natural history studies elucidate a grim prognosis for young patients treated nonoperatively following a primary traumatic dislocation. A seminal 10-year review of nonoperatively managed dislocations revealed a redislocation rate of approximately 66% for patients presenting under the age of 22. Subsequent 25-year longitudinal follow-up data corroborated these findings, demonstrating an overall recurrence rate of 50% in patients under 40, which surged to over 60% in the adolescent and young adult cohorts. Age at the time of initial dislocation remains the single most robust predictor of recurrence, heavily influenced by the patient's baseline activity level and participation in collision or contact sports.
The fundamental pathoanatomic lesion driving traumatic anteroinferior instability is the Bankart lesion, defined as the traumatic avulsion of the anteroinferior labrum and its attached capsule from the anterior glenoid rim. This lesion is ubiquitous, present in approximately 90% of all traumatic glenohumeral dislocations. Recurrent dislocation episodes invariably lead to progressive plastic deformation of the middle and inferior glenohumeral ligaments, exacerbating capsular redundancy and compromising the critical "sling" mechanism designed to restrict anterior translation. Furthermore, recurrent instability drastically increases the incidence of secondary osseous injuries, including the Hill-Sachs lesion (a posterosuperior humeral head impaction fracture) and the bony Bankart lesion (attritional bone loss or fracture of the anterior glenoid rim). In older demographics, the pathoanatomic profile shifts; a traumatic dislocation in a patient over the age of 40 must be viewed with a high index of suspicion for concomitant rotator cuff pathology, necessitating a meticulous strength examination and advanced soft-tissue imaging.
Detailed Surgical Anatomy and Biomechanics
The osteology of the glenohumeral joint is inherently unstable, often analogized to a golf ball sitting on a tee. The normal glenoid is distinctly pear-shaped, being broader inferiorly than superiorly, providing a minimal bony buttress against translation. The articulating surface of the humeral head is approximately three to four times the size of the corresponding glenoid cavity, resulting in limited osseous congruency. To compensate for this profound bony mismatch, the shallow glenoid vault is deepened by thicker articular cartilage on its periphery and the critical presence of the fibrocartilaginous labrum. This ring-like labral structure effectively increases the depth of the socket by 50% and serves as a vital "chock-block," preventing the humeral head from rolling anteriorly over the glenoid rim during physiologic motion.



The capsuloligamentous complex represents the primary static restraint of the shoulder, with different geographic areas contributing to stability based on the precise anatomic position of the arm. The inferior glenohumeral ligament (IGHL) complex is the paramount static restraint against anteroinferior instability, particularly when the arm is placed in abduction angles of 45 to 90 degrees. This complex is composed of an anterior band, a posterior band, and an interposed axillary pouch, functioning as a dynamic hammock that shifts to support the humeral head. The anterior band of the IGHL is unequivocally the most critical static stabilizer against anterior translation in the classic position of apprehension (abduction and external rotation). Conversely, the superior glenohumeral ligament (SGHL) and the middle glenohumeral ligament (MGHL) play distinct roles, primarily limiting inferior translation and anteroposterior translation when the arm is in adduction and lower degrees of elevation.
Dynamic stability is seamlessly orchestrated by the complex interaction of the rotator cuff musculature, the long head of the biceps brachii, and the periscapular stabilizers. The rotator cuff muscles (subscapularis, supraspinatus, infraspinatus, and teres minor) provide critical dynamic stability via concavity compression, forcefully driving the convex humeral head into the concave glenoid socket during active motion. The long head of the biceps brachii further augments anterior and superior stability, acting as a depressor of the humeral head. The superior labrum serves as the robust anchor point for the biceps tendon, while the inferior labrum functions as the foundational attachment for the glenohumeral ligaments.
Secondary and tertiary contributors to glenohumeral joint stability include negative intra-articular joint pressure, articular version, and adhesion-cohesion forces of the synovial fluid. The negative intra-articular pressure creates a vacuum effect that resists inferior subluxation of the humeral head, a mechanism that is immediately lost upon capsular venting during arthroscopy or traumatic capsular tearing. Furthermore, the precise orientation of the glenoid (typically demonstrating slight retroversion) and the humeral head (retroverted approximately 30 degrees) dictates the baseline biomechanical vectors of the joint. Disruption of any single component—be it the labral chock-block, the capsuloligamentous tension, or the dynamic concavity compression—precipitates a cascading failure of the entire stabilizing mechanism, culminating in recurrent clinical instability.
Exhaustive Indications and Contraindications
The decision to proceed with arthroscopic stabilization of anterior shoulder instability hinges upon a multifaceted evaluation of patient-specific variables, including chronological age, athletic demands, chronicity of symptoms, and meticulous quantification of osseous defects. Primary indications for arthroscopic Bankart repair include recurrent, symptomatic unidirectional anteroinferior instability in patients who have failed a comprehensive trial of nonoperative management. Furthermore, there is a growing, evidence-based consensus advocating for early, primary arthroscopic stabilization in young (under 25 years), high-demand collision or overhead athletes following a first-time traumatic dislocation. Multiple landmark studies have unequivocally demonstrated that early surgical reconstruction in this specific demographic drastically decreases the risk of recurrence, mitigates the progression of secondary intra-articular damage, and significantly improves long-term quality of life compared to conservative immobilization.



Contraindications to purely arthroscopic soft-tissue stabilization are primarily dictated by the presence and magnitude of bipolar bone loss. Critical glenoid bone loss—historically defined as >20-25% of the inferior glenoid width, resulting in the pathognomonic "inverted pear" appearance—represents an absolute contraindication to isolated arthroscopic Bankart repair. Attempting a soft-tissue repair in the face of such osseous deficiency invariably leads to unacceptable failure rates, necessitating bony augmentation procedures such as the Latarjet or distal tibial allograft reconstruction. Similarly, massive, "engaging" Hill-Sachs lesions that lever over the anterior glenoid rim during functional ranges of motion contraindicate isolated capsulolabral repair. In these scenarios, the arthroscopic surgeon must consider concomitant procedures such as a remplissage (capsulotenodesis of the infraspinatus into the humeral defect) to convert an engaging lesion into a non-engaging one.
Other relative contraindications to arthroscopic stabilization include patients with profound, uncorrected multidirectional instability driven by connective tissue disorders (e.g., Ehlers-Danlos or Marfan syndrome), where tissue quality is inherently compromised. Furthermore, the presence of a Humeral Avulsion of the Glenohumeral Ligament (HAGL) lesion historically pushed surgeons toward open repair, although advanced arthroscopic techniques have made arthroscopic HAGL repair feasible in the hands of master-level arthroscopists. Severe capsular deficiency, often seen in the setting of prior failed thermal capsulorrhaphy, also represents a strict contraindication to arthroscopic revision, as the necrotic, attenuated capsule cannot hold suture tension and mandates an open capsular reconstruction with allograft.
| Clinical Variable | Arthroscopic Soft-Tissue Repair | Open / Bony Augmentation Procedure |
|---|---|---|
| Glenoid Bone Loss | Minimal to none (< 15%) | Significant (> 20%), "Inverted Pear" |
| Humeral Bone Loss | Small, non-engaging Hill-Sachs | Large, engaging Hill-Sachs (> 25% articular surface) |
| Tissue Quality | Robust, distinct capsulolabral tissue | Attenuated, thermal necrosis, prior multiple failures |
| Instability Direction | Unidirectional anteroinferior | Multidirectional with severe hyperlaxity (relative) |
| Patient Profile | Standard athletic or recreational demand | Elite collision athletes with borderline bone loss |
| Specific Lesions | Bankart, ALPSA, SLAP | Large HAGL (if not amenable to scope), bony Bankart >25% |
Pre-Operative Planning, Templating, and Patient Positioning
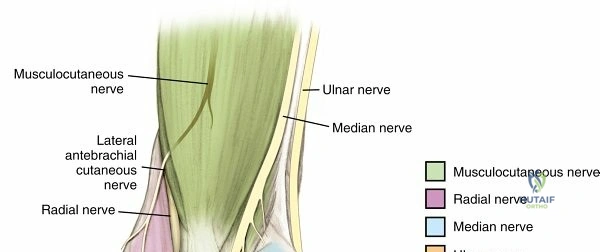
A meticulous patient history and comprehensive physical examination form the bedrock of successful pre-operative planning for anterior shoulder instability. The clinician must systematically address five critical historical questions: Did the initial episode require formal reduction? What was the exact arm position during the primary and subsequent dislocations? What was the magnitude of disability following the initial event? How many subsequent episodes have occurred, and were they frank dislocations or transient subluxations? Finally, what was the magnitude of trauma associated with the initial event versus subsequent episodes? A progression from high-energy initial trauma to low-energy recurrent subluxations strongly suggests progressive capsular attenuation and expanding osseous defects. The physical examination must begin with a posterior inspection to assess for muscular atrophy, particularly of the deltoid and rotator cuff, which may indicate concomitant axillary or suprascapular nerve injury.




Provocative maneuvers are essential to accurately diagnose and quantify the direction and severity of instability. The apprehension test, performed with the arm in 90 degrees of abduction and progressive external rotation, is highly sensitive for anterior instability. It is critical to differentiate true apprehension (a subjective feeling of impending dislocation) from mere pain. The Jobe relocation test, applying a posteriorly directed force on the proximal humerus, should alleviate apprehension, confirming the diagnosis. The load and shift test must be performed bilaterally to grade anterior, posterior, and inferior translation, providing a baseline of the patient's innate ligamentous laxity. Furthermore, the sulcus sign must be evaluated; failure of external rotation to obliterate the sulcus strongly indicates a compromised rotator interval and multidirectional laxity, necessitating a more comprehensive capsular plication during surgery.
Advanced imaging is non-negotiable in the modern era of instability surgery. Standard radiographic series must include an AP view in internal rotation (to assess for Hill-Sachs lesions and greater tuberosity fractures), a true AP of the glenohumeral joint (Grashey view), and a West Point axillary view to critically evaluate the anteroinferior glenoid rim for bony avulsions or attritional wear. When bony deficiencies are suspected based on plain films or clinical history (e.g., instability during sleep, apprehension at low abduction angles), a 3D reconstructed Computed Tomography (CT) scan with humeral head subtraction is the gold standard. This allows for precise, volumetric quantification of glenoid bone loss utilizing the best-fit circle method. Magnetic Resonance Imaging (MRI), preferably with intra-articular gadolinium arthrography (MRA), is indispensable for evaluating the integrity of the labrum, identifying ALPSA (Anterior Labroligamentous Periosteal Sleeve Avulsion) or GLAD (Glenolabral Articular Disruption) lesions, and ruling out concomitant rotator cuff tears or capsular ruptures.




Patient positioning in the operating room is a matter of surgeon preference, with both the beach chair and lateral decubitus positions offering distinct advantages. The lateral decubitus position, utilizing 10 to 15 pounds of balanced suspension traction, provides unparalleled joint distraction, expanding the axillary pouch and facilitating excellent visualization of the inferior glenoid and IGHL complex. This position is highly advantageous for complex capsular shifts and inferior anchor placement. Conversely, the beach chair position offers a more anatomic orientation of the shoulder girdle, facilitates seamless conversion to an open procedure if necessary, and eliminates the risk of traction-related neurapraxia. Regardless of the chosen position, a thorough Examination Under Anesthesia (EUA) is mandatory prior to prepping and draping. The EUA allows the surgeon to assess the true magnitude of translation without muscle guarding, confirming the operative plan and identifying any unrecognized multidirectional components.
Step-by-Step Surgical Approach and Fixation Technique
Diagnostic Arthroscopy and Glenoid Preparation
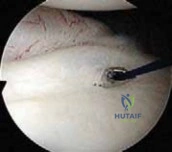
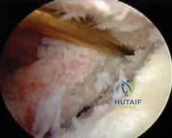
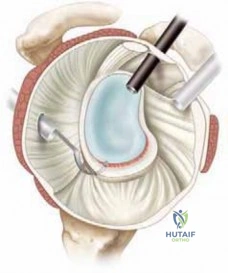
The surgical approach begins with the establishment of a standard posterior viewing portal, placed approximately 2 cm inferior and 1 cm medial to the posterolateral corner of the acromion. Upon entering the joint, a meticulous diagnostic sweep is performed. The surgeon must systematically evaluate the biceps anchor, the superior labrum, the articular surfaces of the humerus and glenoid, the rotator cuff footprint, and the entire capsulolabral complex. Particular attention is directed to the anteroinferior quadrant to confirm the presence of a Bankart or ALPSA lesion. The size and depth of any Hill-Sachs lesion are evaluated dynamically by taking the arm through a range of motion to assess for "engagement" over the anterior glenoid track.


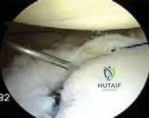
Following the diagnostic sweep, two anterior working portals are established using an outside-in spinal needle localization technique. The anterosuperior portal is typically placed just anterior to the acromioclavicular joint, entering the joint through the rotator interval superior to the biceps tendon; this serves primarily for fluid management and suture retrieval. The critical anteroinferior working portal is placed just superior to the upper border of the subscapularis tendon, ensuring an optimal trajectory (approximately 45 degrees to the glenoid face) for anchor insertion along the anteroinferior glenoid rim. A clear cannula (typically 5.5 mm or 8.25 mm) is introduced to facilitate smooth instrument passage and suture management.
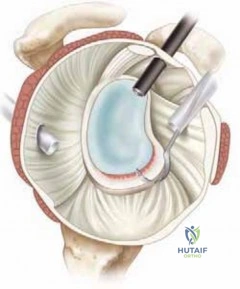
The foundation of a successful arthroscopic stabilization is the meticulous mobilization of the capsulolabral complex. In chronic cases, the torn labrum and IGHL frequently heal in a medially displaced position along the anterior glenoid neck (the ALPSA lesion). Using a combination of arthroscopic elevators, rasps, and electrocautery, the surgeon must aggressively liberate this tissue from the scapular neck. The release must extend inferiorly to the 6 o'clock position to adequately mobilize the inferior capsule. Once the tissue is freed and can be easily reduced to the articular margin, the anterior glenoid neck is lightly decorticated using a motorized burr or rasp. This critical step removes fibrous tissue and exposes bleeding cancellous bone, creating an optimal biological environment for robust soft-tissue healing.
Anchor Placement and Capsulolabral Plication
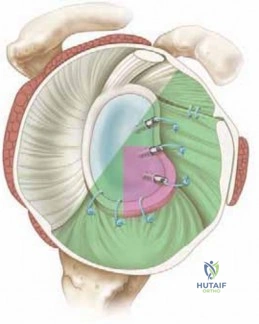
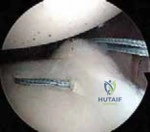
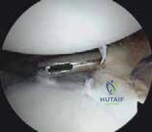
With the glenoid prepared and the tissue mobilized, fixation begins at the most inferior aspect of the lesion, typically at the 5:30 or 6 o'clock position. Modern fixation relies on either biocomposite or all-suture anchors, typically 1.5 mm to 2.9 mm in diameter. The drill guide is introduced through the anteroinferior portal, and the anchor is deployed on the articular margin (1-2 mm onto the articular cartilage face) to recreate the anatomical labral bumper. The trajectory of the drill is paramount; it must be directed slightly medially to avoid penetrating the articular surface of the glenoid vault.