Arthroscopic Solutions for Traumatic Anterior Instability

Key Takeaway
Looking for accurate information on Arthroscopic Solutions for Traumatic Anterior Instability? Traumatic anterior instability is a pathologic condition of the glenohumeral joint where the humeral head abnormally translates on or over the glenoid, often resulting in dislocation or pain. This common form of anterior instability typically occurs with the arm in abduction and external rotation, frequently initiated by trauma, especially athletic incidents, and can lead to recurrent instability.
Comprehensive Introduction and Patho-Epidemiology
Glenohumeral stability is a highly orchestrated biomechanical phenomenon dependent on a delicate equilibrium between static and dynamic restraints, ensuring a stable yet exceptionally unconstrained range of motion. In orthopedic terminology, it is critical to differentiate between "laxity" and "instability." Laxity is a purely physiologic term used to describe the passive, asymptomatic translation of the humeral head on the glenoid surface. Conversely, instability represents a pathologic state characterized by abnormal, symptomatic translation of the humeral head on or over the glenoid rim. This pathologic translation clinically manifests as frank dislocation, subluxation, profound functional impairments, or debilitating pain. The glenohumeral joint is the most frequently dislocated major joint in the human body, with the vast majority of these dislocations occurring in the anteroinferior direction.
Anterior instability exists on a broad spectrum and is traditionally categorized into traumatic, acquired, or atraumatic etiologies. Traumatic instability, historically summarized by the acronym TUBS (Traumatic, Unidirectional, Bankart lesion, Surgery), typically occurs when a profound force is applied to the arm positioned in vulnerable abduction and external rotation. Acquired instability is frequently observed in overhead athletes; it presents as a more subtle clinical entity stemming from repetitive microtrauma that gradually attenuates the anterior capsuloligamentous restraints, ultimately contributing to the development of pathologic subluxation. Atraumatic instability, often associated with the AMBRI acronym (Atraumatic, Multidirectional, Bilateral, Rehabilitation, Inferior capsular shift), involves underlying anatomic contributions such as generalized ligamentous hyperlaxity, connective tissue disorders, or glenoid dysplasia.
The pathogenesis of traumatic anterior instability is fundamentally linked to the Bankart lesion, which is defined as the traumatic detachment of the anteroinferior labrum and its attached capsule from the anterior glenoid rim. This hallmark pathoanatomic lesion is present in approximately 90% of all traumatic glenohumeral dislocations. Beyond the structural avulsion of the labrum, recurrent dislocations invariably lead to the plastic deformation of the middle and inferior glenohumeral ligaments. This attenuation contributes to a profound laxity in the capsular "sling" that is biomechanically designed to restrict anterior translation of the humeral head during abduction. Furthermore, extensive soft tissue damage, while less common, can include the Humeral Avulsion of the Glenohumeral Ligaments (HAGL lesion) or mid-substance capsular tears. In chronic cases, the injured labral tissue may heal medially on the glenoid neck—the Anterior Labroligamentous Periosteal Sleeve Avulsion (ALPSA) lesion—leading to chronic insufficiency of the inferior glenohumeral ligament complex.
The natural history of traumatic anterior instability is heavily dictated by patient age and activity level at the time of the initial dislocation. Glenohumeral dislocation affects approximately 2% of the general population, but the recurrence rates are alarmingly high in the young, athletic demographic. Long-term natural history studies demonstrate that nonoperative management of primary dislocations in patients under the age of 22 yields a redislocation rate exceeding 66%. Other comprehensive longitudinal reviews indicate that patients under the age of 20 face recurrence rates upwards of 80% to 90% when treated conservatively. Conversely, older patients (typically over age 40) exhibit significantly lower redislocation rates (approximately 14%), though they are at a markedly increased risk for concomitant rotator cuff pathology following a traumatic dislocation. Given these epidemiologic realities, modern orthopedic consensus strongly supports early surgical intervention for young, high-demand athletes to mitigate the risk of recurrent instability and subsequent joint degeneration.


Detailed Surgical Anatomy and Biomechanics
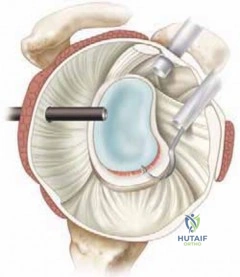
A profound understanding of glenohumeral anatomy is the cornerstone of successful arthroscopic stabilization. The normal bony glenoid is distinctly pear-shaped, being significantly broader inferiorly than superiorly. This osseous articulation is inherently shallow and provides minimal inherent bony stability; the articulating surface of the humeral head is approximately three times the size of the corresponding glenoid cavity. To compensate for this profound osseous mismatch, the shallow bony glenoid is functionally deepened by two primary mechanisms: the presence of thicker articular cartilage on the periphery compared to the center, and the attachment of the fibrocartilaginous labrum. The labrum effectively increases the depth of the socket by 50% and acts as a critical "chock-block," preventing the humeral head from rolling anteriorly over the glenoid rim during extreme ranges of motion.
The capsuloligamentous structures are intimately related to the labrum and provide geographic stability based on the specific anatomic position of the arm. The inferior glenohumeral ligament (IGHL) complex is the most robust and critical static restraint against anterior instability. It functions as a hammock-like sling, consisting of an anterior band, a posterior band, and an interposed axillary pouch. The anterior band of the IGHL is the primary static restraint against anterior translation when the arm is in the high-risk position of 45 to 90 degrees of abduction and external rotation. The superior glenohumeral ligament (SGHL) and the middle glenohumeral ligament (MGHL) play secondary roles; the SGHL limits inferior translation with the arm in adduction, while the MGHL primarily limits anteroposterior translation in the mid-ranges of abduction (approximately 45 degrees).
Dynamic stability is seamlessly integrated with these static restraints through the complex interaction of the rotator cuff, the long head of the biceps brachii, and the periscapular musculature. The rotator cuff muscles (supraspinatus, infraspinatus, teres minor, and subscapularis) provide critical dynamic stability by generating a concavity-compression force. By actively compressing the convex humeral head into the concave glenoid fossa, the rotator cuff dynamically centralizes the joint during complex multidirectional movements. The long head of the biceps brachii further contributes to anterior and superior stability, particularly when the arm is abducted and externally rotated. The scapular stabilizers ensure that the glenoid platform is optimally positioned in three-dimensional space to maximize bony congruence with the humeral head during upper extremity kinematics.
Beyond the macroscopic anatomical structures, several micro-biomechanical factors contribute significantly to joint stability. Negative intra-articular joint pressure creates a vacuum effect that resists inferior subluxation, particularly in the adducted arm. Adhesion-cohesion forces, mediated by the thin film of synovial fluid between the congruent articular surfaces, further resist distracting forces. Articular version also plays a role; the normal glenoid is typically retroverted approximately 1 to 2 degrees, and any pathologic alteration in this version (such as excessive anterior tilt due to dysplasia or wear) can predispose the joint to anterior translation. Disruption of any of these static, dynamic, or micro-biomechanical factors—whether through an acute traumatic Bankart lesion or chronic capsular attenuation—precipitates the pathologic cascade of recurrent anterior instability.


Exhaustive Indications and Contraindications
Patient selection is arguably the most critical determinant of success in the surgical management of traumatic anterior instability. The evolution of arthroscopic techniques and instrumentation has dramatically expanded the indications for minimally invasive stabilization; however, open surgical approaches remain the gold standard for specific, high-risk pathoanatomic profiles. Arthroscopic stabilization is primarily indicated for patients with recurrent, unidirectional anteroinferior instability who possess discrete soft-tissue lesions—such as a classic Bankart tear or an ALPSA lesion—in the absence of critical bone loss. It is the preferred modality for young athletes experiencing recurrent subluxations or dislocations who have failed a dedicated trial of nonoperative management, as well as for first-time dislocators in high-demand sporting populations where the statistical risk of recurrence is unacceptably high.
The primary contraindication to isolated arthroscopic soft-tissue stabilization is the presence of critical glenohumeral bone loss. The concept of the "glenoid track" is paramount in this decision-making process. If a patient possesses an "engaging" Hill-Sachs lesion (an osteochondral defect of the posterosuperior humeral head that engages the anterior glenoid rim during abduction and external rotation) combined with significant anterior glenoid bone loss (typically defined as >20% to 25% of the inferior glenoid width, creating an "inverted pear" appearance), an isolated arthroscopic Bankart repair is doomed to biomechanical failure. In these scenarios of bipolar bone loss, bony augmentation procedures, such as the Latarjet procedure (coracoid transfer) or iliac crest bone grafting, are strictly indicated.
Other relative and absolute contraindications for standard arthroscopic repair include severe capsular deficiency, which may be the result of multiple prior failed surgeries, thermal capsulorrhaphy ablation (a historical technique now largely abandoned due to catastrophic capsular necrosis), or underlying collagen vascular disorders (e.g., Ehlers-Danlos or Marfan syndrome). Furthermore, the presence of a Humeral Avulsion of the Glenohumeral Ligament (HAGL) lesion, while technically repairable via arthroscopy in the hands of master surgeons, is often considered an indication for an open approach due to the technical complexity of achieving adequate tissue mobilization and secure fixation at the humeral neck. High-demand collision athletes (e.g., rugby players, American football linebackers) with borderline bone loss also represent a controversial demographic where open stabilization may provide a more robust, durable construct.
Table: Arthroscopic Versus Open Treatment of Anterior Instability
| Variable | Arthroscopic Stabilization | Open Stabilization / Bony Augmentation |
|---|---|---|
| Bone Defects | Minimal to no bone defects; Small, non-engaging Hill-Sachs; Intact glenoid rim. | Large Hill-Sachs (>25% articular surface); Glenoid deficiency >20% ("inverted pear"). |
| Pathoanatomy | Classic Bankart lesion; ALPSA lesion; Capsular laxity amenable to plication. | Large HAGL lesion; Severe capsular deficiency; Thermal ablation history. |
| Instability Pattern | Unidirectional anteroinferior dislocators. | Recurrent failures of previous arthroscopic procedures. |
| Patient Profile | Standard athletic or recreational population; First-time young dislocators. | High-demand collision athletes (relative); Severe hyperlaxity syndromes (relative). |
| Surgical Morbidity | Lower morbidity, improved cosmesis, less subscapularis violation. | Higher morbidity, requires subscapularis tenotomy/split, potential hardware complications. |

Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning begins with a comprehensive history and a targeted physical examination. The surgeon must ascertain the mechanism of the initial dislocation, the position of the arm during subsequent events, and the magnitude of trauma required to elicit instability. A progression from high-energy initial trauma to low-energy recurrent subluxations is highly suggestive of progressive capsular attenuation and expanding bone loss. Physical examination must include an assessment of generalized ligamentous laxity (Beighton score), active and passive range of motion, and focused provocative testing. The Apprehension test, Jobe Relocation test, and anterior Release (Surprise) test are highly sensitive and specific for anterior instability. The Load and Shift test is utilized to grade the magnitude of anterior translation. Crucially, in older patients, weakness in external rotation or elevation should raise immediate suspicion for a concomitant rotator cuff tear, while sensory deficits over the lateral deltoid necessitate evaluation of the axillary nerve.
Advanced imaging is non-negotiable in the modern surgical planning for instability. Standard radiographic series must include a true anteroposterior (Grashey) view, a scapular Y view, and an axillary lateral view. Specialized views such as the West Point axillary view are excellent for identifying bony Bankart lesions, while the Stryker Notch view is optimal for quantifying Hill-Sachs defects. However, Computed Tomography (CT), specifically with 3D reconstructions and digital subtraction of the humeral head, is the definitive gold standard for quantifying glenoid bone loss. The "best-fit circle" method is applied to the inferior glenoid to calculate the percentage of missing anterior bone. Magnetic Resonance Imaging (MRI), preferably an MR Arthrogram (MRA) with intra-articular gadolinium, is essential for evaluating the integrity of the labrum, identifying ALPSA or HAGL lesions, and assessing the volume and quality of the capsular tissue.
Patient positioning is a matter of surgeon preference, with both the lateral decubitus and beach chair positions offering distinct advantages and disadvantages. The lateral decubitus position utilizes longitudinal and lateral traction (typically 10-15 lbs) with the arm suspended in approximately 45 degrees of abduction and 15 degrees of forward flexion. This position provides unparalleled visualization of the anteroinferior glenoid and naturally distracts the joint space, making inferior anchor placement and capsular shifting technically easier. Conversely, the beach chair position places the patient in a semi-seated posture (approximately 45-60 degrees). This position allows for a more anatomic orientation of the shoulder girdle, facilitates easy conversion to an open approach if necessary, and simplifies the assessment of the glenoid track dynamically during the procedure. However, it requires an assistant or a mechanical arm holder to manipulate the extremity and can be associated with rare but severe cerebral hypoperfusion events if blood pressure is not strictly monitored.
Regardless of the chosen position, precise portal placement is critical for the success of the arthroscopic repair. A standard posterior viewing portal is established first, typically 2 cm inferior and 1 cm medial to the posterolateral acromial corner. Following a thorough diagnostic sweep of the joint, an anterosuperior portal is established via an outside-in spinal needle localization, entering the joint through the rotator interval just anterior to the biceps tendon. This portal serves as the primary viewing portal for anterior work and for suture management. Finally, an anteroinferior (or 5 o'clock) portal is established just superior to the subscapularis tendon. This is the primary working portal; its trajectory must allow for a "deadman's angle" (typically 45 degrees to the glenoid face) for optimal suture anchor insertion along the anteroinferior glenoid rim.



Step-by-Step Surgical Approach and Fixation Technique
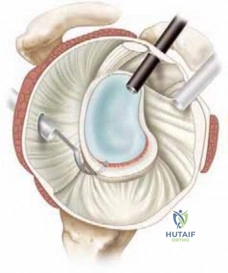
The arthroscopic procedure commences with a systematic diagnostic evaluation of the glenohumeral joint. The surgeon meticulously inspects the articular surfaces for chondral damage, evaluates the biceps anchor and superior labrum for SLAP lesions, and probes the anterior labrum to define the extent of the Bankart tear. The humeral head is examined for a Hill-Sachs lesion, and its engagement with the anterior glenoid is dynamically tested by bringing the arm into abduction and external rotation. If the lesion engages the glenoid rim, an adjunctive procedure such as a remplissage (insetting the infraspinatus and posterior capsule into the defect) must be planned. The inferior capsule and axillary recess are inspected to assess tissue volume and to rule out a HAGL lesion.
The most critical, yet frequently under-executed, step of the procedure is the mobilization of the capsulolabral complex. In chronic instability, the avulsed labrum and capsule often scar down medially along the anterior glenoid neck (the ALPSA configuration). Using a combination of arthroscopic elevators, rasps, and electrocautery, the surgeon must completely release this tissue from the bony neck. The release must extend inferiorly to at least the 6 o'clock position (the absolute bottom of the glenoid) to allow the inferior glenohumeral ligament to be adequately shifted superiorly. Once the tissue is fully mobilized and floats freely, the anterior glenoid neck is decorticated using a motorized burr or rasp. This creates a bleeding cancellous bone bed, which is biologically imperative for robust soft-tissue-to-bone healing.
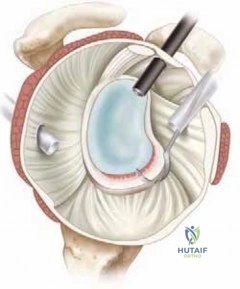
Following preparation of the bony bed, suture anchor fixation is initiated. The first anchor is the most critical and the most technically demanding; it must be placed at the 5:30 or 6 o'clock position to appropriately tension the inferior sling. The anchor is inserted via the anteroinferior portal, ensuring a trajectory that avoids penetrating the articular cartilage while maximizing purchase in the dense subchondral bone of the glenoid rim. Modern techniques predominantly utilize biocomposite or all-suture anchors (typically 1.5 mm to 2.9 mm in diameter) double-loaded with high-strength ultra-high-molecular-weight polyethylene (UHMWPE) suture. Subsequent anchors are placed sequentially moving superiorly along the anterior rim, typically at the 4:30 and 3 o'clock positions, ensuring a minimum of three anchors for a standard Bankart repair.
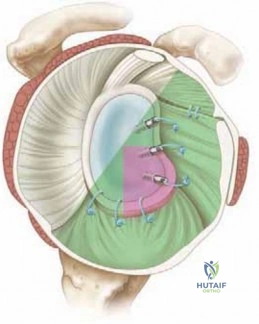
Suture passing and capsular plication require meticulous technique to restore the anatomic bumper and retension the IGHL. Using a curved suture passing device (e.g., a spectrum hook or specialized jawed passer), the surgeon takes a substantial bite of the capsule inferior and lateral to the anchor site, incorporating the labral tissue. By passing the suture through this tissue and tying it (or utilizing knotless anchor technology), the capsule is shifted superiorly and medially back onto the glenoid rim. This "south-to-north" and "west-to-east" shift eliminates the pathologic capsular redundancy and recreates the labral chock-block effect. The knots are tied securely, ensuring the knots rest on the capsular side away from the articular cartilage to prevent iatrogenic chondral abrasion. The final construct is dynamically tested under direct arthroscopic visualization to confirm the restoration of stability and the elimination of abnormal humeral head translation.



Complications, Incidence Rates, and Salvage Management
Despite advancements in arthroscopic techniques, complications following anterior stabilization remain a significant clinical challenge. The most devastating and frequent complication is recurrent instability, with modern literature reporting failure rates ranging from 5% to 15% in optimally selected patients, but soaring to over 30% in high-risk cohorts (e.g., teenage collision athletes). Recurrence is almost invariably multifactorial. Technical errors—such as inadequate labral mobilization, failure to place the most inferior anchor at the 6 o'clock position, or insufficient capsular plication—are common culprits. However, the most profound driver of failure is the unrecognized or underappreciated presence of bipolar bone loss. When arthroscopic soft-tissue repairs are erroneously applied to patients with engaging Hill-Sachs lesions or glenoid defects exceeding 20%, the biomechanical forces across the joint rapidly overwhelm the suture anchors, leading to catastrophic construct failure.
Post-operative stiffness, particularly a profound loss of external rotation, is another notable complication. While a mild loss of terminal external rotation (5 to 10 degrees) is an expected and often protective outcome of a successful capsulorrhaphy, severe restriction can cause significant functional impairment and secondary pain. This stiffness is typically the result of iatrogenic overtensioning of the anterior capsule, non-anatomic medialization of the labrum during repair, or prolonged, overly conservative post-operative immobilization. Management initially consists of aggressive, directed physical therapy; however, refractory cases may necessitate arthroscopic capsular release. Conversely, hardware-related complications have decreased with the advent of all-suture and biocomposite anchors, but prominent knots or anchors placed too close to the articular margin can cause devastating iatrogenic chondrolysis and early-onset osteoarthritis.
Neurologic injury during arthroscopic stabilization is rare but carries severe medicolegal and functional implications. The axillary nerve is at greatest risk during the establishment of the anteroinferior portal and during capsular plication at the 6 o'clock position. The nerve lies in close proximity (often within 10-15 mm) to the inferior capsule. Similarly, the musculocutaneous nerve can be compromised by overzealous medial retraction or errant portal placement through the conjoined tendon. A thorough post-operative neurologic examination is mandatory, and any deficits require immediate evaluation, potentially including electromyography (EMG) if recovery is not observed within the first several weeks.
When primary arthroscopic stabilization fails, salvage management requires a paradigm shift toward open, bony reconstructive procedures. Revision arthroscopy yields notoriously poor results, with failure rates exceeding 40%. The gold standard for salvage is the Latarjet procedure, which involves osteotomizing the coracoid process and transferring it, along with the attached conjoined tendon, to the anterior glenoid defect. This procedure provides a "triple effect": a bony augmentation to increase the glenoid arc, a dynamic sling effect from the conjoined tendon crossing the inferior capsule, and a capsular repair utilizing the coracoacromial ligament stump. In cases of massive humeral head defects, an open remplissage or structural osteochondral allografting of the Hill-Sachs lesion may be required to restore the glenoid track and prevent recurrent engagement.
Table: Complications and Incidence Rates
| Complication | Estimated Incidence | Primary Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Recurrent Instability | 5% - 15% (Standard) >30% (High-risk) |
Unrecognized bone loss; Technical error; Non-compliance; High-impact trauma. | Latarjet procedure; Iliac crest bone graft; Open capsular shift. |
| Loss of External Rotation | 10% - 20% | Overtensioning of anterior capsule; Prolonged immobilization. | Aggressive physical therapy; Arthroscopic capsular release. |
| Hardware Complications | < 2% | Prominent anchors; Intra-articular knots; Osteolysis from biocomposites. | Hardware removal; Chondroplasty; Conversion to arthroplasty if severe OA. |
| Neurologic Injury | < 1% | Axillary nerve traction/suture entrapment at 6 o'clock position. | Observation; EMG at 6 weeks; Nerve exploration/grafting if no recovery. |
| Infection | < 0.5% | Cutaneous flora (C. acnes); Poor sterile technique. | Arthroscopic I&D; Targeted intravenous antibiotic therapy. |
Phased Post-Operative Rehabilitation Protocols
The success of an arthroscopic Bankart repair is inextricably linked to a meticulously structured, phased post-operative rehabilitation protocol. The delicate biological healing process of the labrum to the glenoid bone bed requires a minimum of 6 to 8 weeks; therefore, the initial phases of rehabilitation must strictly prioritize tissue protection over the restoration of motion. Phase I (Weeks 0-4) is characterized by strict immobilization in a sling, with the arm typically positioned in neutral or slight internal rotation. Active range of motion of the elbow, wrist, and hand is encouraged immediately to prevent distal stiffness and mitigate the risk of complex regional pain syndrome. Passive forward flexion is generally limited to 90 degrees, and passive external rotation is strictly restricted to neutral (0 degrees) to prevent catastrophic
Clinical & Radiographic Imaging Archive