Anterior Glenohumeral Instability: A Masterclass in Bankart Repair and Inferior Capsular Shift

Key Takeaway
This masterclass provides an exhaustive, real-time guide to Bankart repair and inferior capsular shift for anterior glenohumeral instability. Fellows will learn intricate surgical anatomy, precise intraoperative techniques, and critical pearls to optimize outcomes. We cover patient positioning, detailed dissection, anchor placement, labral repair, capsular shift, and comprehensive postoperative management, preparing you for successful shoulder stabilization.
Comprehensive Introduction and Patho-Epidemiology
Anterior glenohumeral instability represents one of the most ubiquitous and biomechanically complex pathologies encountered in orthopedic sports medicine and shoulder surgery. The glenohumeral joint, inherently designed for unparalleled global mobility, sacrifices intrinsic osseous stability to achieve this vast range of motion. Consequently, it relies heavily on an intricate, highly coordinated network of static capsuloligamentous restraints and dynamic musculotendinous stabilizers. When this delicate equilibrium is disrupted—whether through an acute, high-energy traumatic dislocation or via repetitive, insidious microtrauma in the overhead athlete—the resulting instability can severely compromise upper extremity function, leading to recurrent subluxations, dislocations, and profound disability.
The patho-epidemiology of anterior shoulder instability demonstrates a distinct bimodal distribution, though it predominantly afflicts the young, active demographic. In patients under the age of 25 who sustain a primary traumatic anterior dislocation, the natural history without surgical intervention is notoriously grim, with recurrence rates historically reported between 70% and 90%. This high propensity for recurrence is driven by the failure of the anterior inferior capsulolabral complex to heal anatomically to the glenoid rim—the classic "essential lesion" first articulated by A. Blundell Bankart. Conversely, in patients over the age of 40, recurrent instability is less common, but primary dislocations are frequently complicated by concomitant rotator cuff tears or axillary nerve neuropraxias, necessitating a high index of clinical suspicion and a different treatment paradigm.
Historically, the surgical management of anterior instability has evolved from non-anatomic tenodesis procedures (such as the Putti-Platt or Magnuson-Stack), which reliably prevented dislocation but universally sacrificed external rotation and precipitated early-onset osteoarthritis. The paradigm shifted dramatically toward anatomic reconstruction with the popularization of the open Bankart repair, and subsequently, Charles Neer’s introduction of the inferior capsular shift. This procedure was revolutionary, addressing not just the focal labral detachment, but the global capsular redundancy and plastic deformation that inevitably accompany recurrent instability.
Today, while arthroscopic techniques have largely supplanted open surgery for isolated Bankart lesions, the open Bankart repair combined with an inferior capsular shift remains the undisputed gold standard—a true masterclass procedure—for patients with complex instability, profound capsular laxity, failed prior arthroscopic stabilization, or those engaged in high-demand collision sports. This chapter provides an exhaustive, definitive guide to understanding the pathoanatomy, meticulous preoperative planning, and precise surgical execution of the anatomic Bankart repair and inferior capsular shift. Our objective is to equip the orthopedic surgeon with the technical mastery required to restore the intricate architecture of the shoulder, ensuring enduring stability without compromising functional kinematics.
Detailed Surgical Anatomy and Biomechanics
Before a surgical blade ever meets the skin, the operating surgeon must possess an uncompromising, three-dimensional understanding of glenohumeral anatomy and biomechanics. The shoulder’s stability is not derived from a single structure, but rather from a synergistic symphony of dynamic and static components that dynamically adapt to the arm's position in space.
Dynamic Stabilizers
The dynamic stabilizers are primarily the musculotendinous units that actively compress the humeral head into the shallow glenoid fossa. This fundamental biomechanical principle is known as concavity compression. The efficiency of concavity compression is dictated by the magnitude of the compressive force generated by the muscles and the depth of the concavity provided by the glenoid and intact labrum.
The rotator cuff muscles—the supraspinatus, infraspinatus, teres minor, and subscapularis—are the primary effectors of this dynamic stability. They fire in a highly coordinated, force-couple mechanism to steer the humeral head and maintain its articulation within the center of the glenoid throughout the arc of motion. The subscapularis, in particular, acts as a dynamic anterior buttress, although its primary role is internal rotation and joint compression rather than acting as a static checkrein against anterior translation.
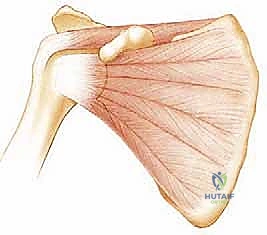
FIG 1 • Dynamic stabilizers of the glenohumeral joint include the rotator cuff muscles (supraspinatus, infraspinatus, teres minor, subscapularis; A,B).
Beyond the rotator cuff, the periscapular musculature (serratus anterior, rhomboids, trapezius, and levator scapulae) plays an indispensable role. Proper scapulothoracic kinematics ensure that the glenoid is constantly repositioned to provide a stable platform for the humeral head, a concept known as scapulohumeral rhythm. Dysrhythmia or scapular winging drastically alters the joint reaction forces, predisposing the anterior capsuloligamentous structures to excessive strain. Furthermore, the long head of the biceps tendon contributes to anterior stability. Originating from the supraglenoid tubercle and superior labrum, it acts as a dynamic depressor of the humeral head and provides resistance to anterior translation, particularly when the arm is abducted and externally rotated—the classic provocative position for anterior instability.
Static Stabilizers
The static stabilizers comprise the passive, non-contractile restraints that provide inherent stability at the end ranges of motion. These include the osseous geometry, the glenoid labrum, the glenohumeral ligaments, and the negative intra-articular pressure of the joint. The bony glenoid is relatively flat and pear-shaped, offering minimal intrinsic constraint. However, the glenoid labrum—a dense, fibrocartilaginous rim—attaches to the periphery of the glenoid, deepening the socket by up to 50% and significantly increasing the articular surface area available for contact with the humeral head.

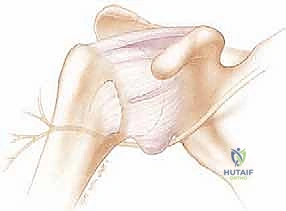
FIG 1 • The static stabilizers of the glenohumeral joint include the glenohumeral ligaments of the capsule (C), and the glenoid labrum (D), which deepens the socket and serves as an attachment for the glenohumeral ligaments and biceps tendon.
The capsule-labral complex is the critical focus of our surgical intervention. It consists of the anterior, middle, and superior glenohumeral ligaments, which function as variable tension checkreins depending on arm position. The Superior Glenohumeral Ligament (SGHL) and the coracohumeral ligament reside within the rotator interval, providing primary restraint to inferior translation when the arm is adducted. The Middle Glenohumeral Ligament (MGHL) is highly variable in its thickness and origin, but generally resists anterior translation in the mid-range of abduction (approximately 45 degrees).
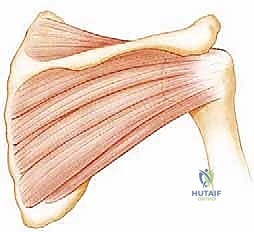
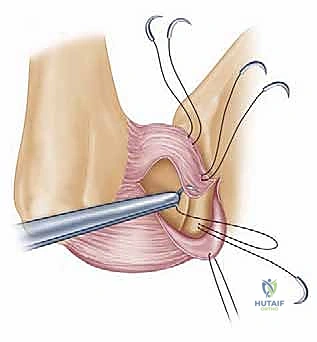
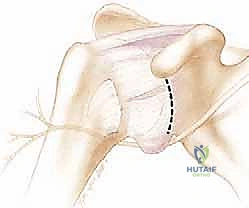
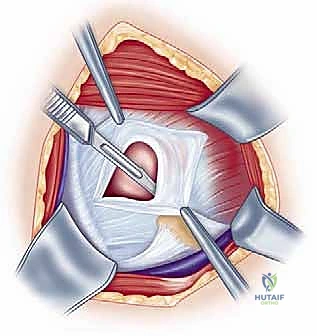
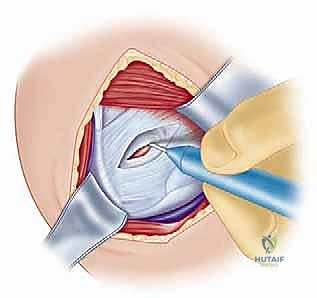
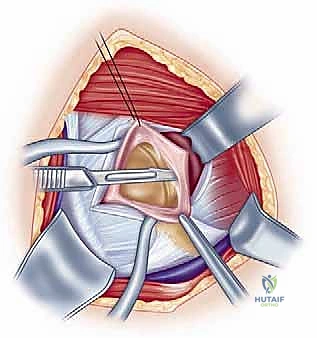
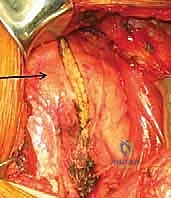
FIG 2 • A. The Bankart lesion: tear of the anterior inferior glenoid labrum.

FIG 2 • B. Axial view MRI scan showing the anterior labral periosteal sleeve avulsion (ALPSA).
The Inferior Glenohumeral Ligament (IGHL) complex is the most robust and biomechanically significant static restraint against anterior instability. It is composed of an anterior band, a posterior band, and an interposed axillary pouch, functioning analogously to a hammock supporting the humeral head. When the arm is placed in the classic "at-risk" position of 90 degrees of abduction and maximal external rotation, the anterior band of the IGHL tightly crosses the joint anteriorly, serving as the primary barrier to anterior-inferior translation. Biomechanical studies have demonstrated that failure of this complex typically occurs at the glenoid insertion (the Bankart lesion, 40% of cases), but significant plastic deformation and capsular stretching (up to 34% elongation) occur before overt macroscopic tearing. This microscopic failure and permanent elongation necessitate the capsular shift component of our surgical reconstruction.
Neurovascular Structures of Concern
Navigating the anterior shoulder requires profound respect for the regional neurovascular anatomy, as iatrogenic injury can result in devastating functional consequences. The axillary nerve is the structure at highest risk during an inferior capsular shift. Arising from the posterior cord of the brachial plexus, it courses anterior to the subscapularis before diving posteriorly through the quadrangular space. Crucially, as it traverses the inferior capsule, it lies a mere 2 to 3 millimeters from the dependent axillary pouch. During the release of the inferior capsule from the humeral neck, or when placing anchors at the 6 o'clock position on the glenoid, the axillary nerve is in immediate proximity and must be meticulously protected, often requiring direct visualization or palpation.
The musculocutaneous nerve, derived from the lateral cord, pierces the coracobrachialis muscle typically 3 to 5 centimeters distal to the tip of the coracoid process. However, anatomic variations exist where it may enter much closer to the coracoid. Aggressive medial retraction of the conjoined tendon during the deep deltopectoral dissection can cause traction neuropraxia of this nerve, leading to profound weakness in elbow flexion. Retractors placed on the medial aspect of the conjoined tendon must be used judiciously and relaxed periodically.
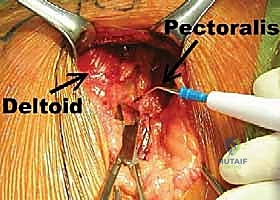
Superficially, the cephalic vein marks the internervous plane between the deltoid (axillary nerve) and the pectoralis major (medial and lateral pectoral nerves). While sacrificing the vein is rarely catastrophic, preserving it is preferred to optimize venous drainage of the upper extremity. We typically retract the cephalic vein laterally with the deltoid, as its major tributaries generally drain from the deltoid muscle belly, minimizing the risk of avulsing these branches during retraction. Finally, the deeper brachial plexus and axillary artery/vein lie medial to the coracoid process; while generally safe during a standard Bankart repair, errant medial dissection or catastrophic retractor slippage can theoretically endanger these vital structures.
Exhaustive Indications and Contraindications
The decision to proceed with an open Bankart repair and inferior capsular shift must be predicated on rigorous patient selection. Not all instability is created equal, and applying this powerful soft-tissue operation to the wrong pathology will inevitably lead to failure. The Thomas and Matsen classification of TUBS (Traumatic, Unidirectional, Bankart, Surgery) versus AMBRI (Atraumatic, Multidirectional, Bilateral, Rehabilitation, Inferior capsular shift) historically guided treatment, but modern understanding recognizes a vast spectrum of instability that often blurs these lines.
Absolute indications for an open Bankart repair and inferior capsular shift include recurrent, symptomatic anterior glenohumeral instability that has failed a comprehensive trial of non-operative management (including dedicated physical therapy focusing on dynamic stabilizers). It is particularly indicated in patients with profound capsular laxity, such as those with a concomitant drive-through sign on arthroscopy or multidirectional instability with a predominant anterior component. Furthermore, young, high-demand collision athletes (e.g., rugby or American football players) often benefit from the robust, structural reinforcement provided by an open capsular shift, which historically demonstrates lower recurrence rates in this specific demographic compared to arthroscopic techniques. Revision stabilization scenarios, where prior arthroscopic anchors have failed and capsular tissue is attenuated, represent a classic indication for the open approach.
Contraindications must be carefully evaluated to prevent surgical failure. The most critical contraindication to a soft-tissue-only repair is the presence of critical glenoid bone loss. Biomechanical and clinical data clearly demonstrate that if the anterior glenoid defect exceeds 20% to 25% of the inferior glenoid width (often resulting in an "inverted pear" glenoid), soft-tissue repair alone will fail at unacceptably high rates. These patients require a bony augmentation procedure, such as a Latarjet or distal tibial allograft. Similarly, a massive, engaging Hill-Sachs lesion that falls "off-track" necessitates either a Remplissage procedure or an osseous allograft, rather than an isolated anterior capsular shift.
Voluntary dislocators—patients who can willfully subluxate or dislocate their shoulders, often for secondary gain or due to underlying psychiatric conditions—represent an absolute contraindication to surgical stabilization. Surgery in these patients almost universally fails and can lead to severe complications. Additionally, patients with profound, uncorrected multidirectional instability driven entirely by systemic collagen disorders (e.g., Ehlers-Danlos or Marfan syndrome) should be approached with extreme caution, as their inherently defective collagen often stretches out again despite a technically perfect capsular shift.
| Indication / Contraindication | Specific Pathology / Patient Profile | Clinical Rationale |
|---|---|---|
| Absolute Indication | Recurrent Traumatic Anterior Instability | Failure of conservative therapy; functional impairment in daily life or sports. |
| Absolute Indication | Revision Stabilization | Failed prior arthroscopic Bankart; attenuated capsular tissue requiring robust open shift. |
| Relative Indication | High-Demand Collision Athletes | Open repair provides superior biomechanical strength in patients subject to extreme joint forces. |
| Relative Indication | Profound Capsular Laxity (HAGL) | Humeral Avulsion of the Glenohumeral Ligament requires open repair to restore the lateral capsular reflection. |
| Absolute Contraindication | Critical Glenoid Bone Loss (>20-25%) | Soft tissue repair will fail; requires structural bone graft (Latarjet, Iliac Crest, or Tibial Allograft). |
| Absolute Contraindication | Voluntary Dislocators | High risk of intentional recurrence; underlying psychiatric or behavioral factors must be addressed first. |
| Relative Contraindication | Severe Connective Tissue Disorders | Ehlers-Danlos, Marfan syndrome; high risk of recurrent capsular stretching despite anatomic repair. |
| Relative Contraindication | Engaging "Off-Track" Hill-Sachs | Requires combined procedure (Remplissage or humeral head allograft) to prevent engagement over the anterior rim. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the bedrock upon which successful surgical outcomes are built. This process begins with a comprehensive clinical evaluation. The surgeon must elicit a detailed history, focusing on the mechanism of the initial injury, the frequency and ease of subsequent dislocations, the direction of instability, and the specific arm positions that provoke symptoms. A thorough physical examination is paramount. We assess for generalized ligamentous laxity using the Beighton criteria. Inspection may reveal muscle atrophy, particularly of the deltoid or rotator cuff, hinting at chronic disuse or concurrent nerve injury.
Provocative testing is critical for confirming the diagnosis and direction of instability. The Apprehension Test is performed with the patient supine, bringing the arm into 90 degrees of abduction and progressive external rotation. A positive test is not merely pain, but a distinct sense of impending dislocation and guarding by the patient. The Jobe Relocation Test follows immediately; applying a posterior-directed force on the proximal humerus should relieve the apprehension, confirming anterior instability. The Sulcus Sign, evaluated by applying inferior traction on the adducted arm, assesses for inferior laxity and a patulous rotator interval. Finally, the Load and Shift test, ideally performed under anesthesia, allows the surgeon to objectively grade the degree of anterior and posterior humeral head translation across the glenoid rim.
Advanced Imaging Protocols
Radiographic evaluation begins with standard plain films: a True AP (Grashey view), a Scapular Y, and an Axillary lateral view. The Axillary view is non-negotiable, as it is essential for identifying anterior glenoid rim fractures (Bony Bankart lesions) and confirming joint concentricity. Specialized views, such as the Stryker Notch view or AP internal rotation view, are highly sensitive for detecting posterolateral humeral head compression fractures (Hill-Sachs lesions).

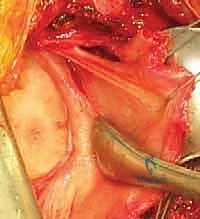
FIG 3 • AP radiographs of the left shoulder showing a dislocated shoulder (A) and subsequent reduction (B). There is a Hill-Sachs fracture of the posterolateral humeral head. C. Axial MRI scan in a patient with deficient glenoid labrum and subscapularis tendon tear.
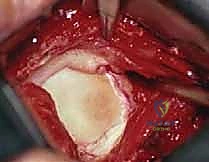
FIG 2 • C,D. CT scan with axial view and reconstruction image, respectively, showing a large anterior inferior glenoid “bony Bankart” fracture.
To quantify bone loss accurately, a high-resolution Computed Tomography (CT) scan with 3D reconstructions with the humeral head digitally subtracted is the gold standard. We utilize the "best-fit circle" method on the en face sagittal view of the glenoid to calculate the percentage of anterior bone loss. Furthermore, the CT scan allows for the assessment of the "Glenoid Track," determining whether a Hill-Sachs lesion will engage the anterior glenoid rim during functional ranges of motion.

FIG 3 • AP radiographs of the left shoulder showing a dislocated shoulder (A) and subsequent reduction.

Magnetic Resonance Imaging (MRI), or preferably MR Arthrography (MRA), is indispensable for evaluating the soft tissues. MRA exquisitely details the labral pathology, distinguishing between a classic Bankart lesion, an ALPSA (Anterior Labral Periosteal Sleeve Avulsion) where the labrum has healed medially down the glenoid neck, or a GLAD (Glenolabral Articular Disruption) lesion. It also allows for the assessment of capsular volume, the integrity of the IGHL, and the presence of concurrent rotator cuff pathology.

Anesthesia and Patient Positioning
For an open Bankart repair and inferior capsular shift, the patient is typically positioned in the modified beach chair position. This position offers several distinct advantages over the lateral decubitus position: it allows for an anatomic orientation of the shoulder, facilitates excellent visualization of the anterior structures, and permits unhindered manipulation of the arm through a full range of motion to assess the tension of the capsular shift dynamically.
Anesthesia usually consists of a regional interscalene nerve block for optimal perioperative pain control, combined with general endotracheal anesthesia to ensure complete muscle relaxation. Once anesthetized, a thorough Examination Under Anesthesia (EUA) is performed and documented. The patient is then brought upright to approximately 45 to 60 degrees. The head and
Clinical & Radiographic Imaging Archive