Mastering SC Joint Dislocations: Diagnosis & Treatment Insights

Key Takeaway
Your ultimate guide to Mastering SC Joint Dislocations: Diagnosis & Treatment Insights starts here. **SC joint dislocations** involve displacement of the sternoclavicular joint. Patients typically experience severe pain, often supporting the injured arm with a tilted head. Anterior dislocations may show a prominent medial clavicle. Posterior dislocations, though rarer, can cause venous congestion, numbness, and tingling, requiring careful evaluation due to associated risks.
A 22-year-old male presents to the Emergency Department following a high-energy rugby tackle. He complains of chest pain and a sensation of "choking" when lying supine. On inspection, there is fullness at the medial aspect of the clavicle, but the clavicular head is not palpable. What is your immediate diagnostic priority and how do you proceed with imaging?
Candidate: Given the mechanism and symptoms of airway compromise, I suspect a posterior sternoclavicular dislocation. My priority is assessing ABCs. For imaging, I would start with a chest radiograph and a Serendipity view. If a posterior dislocation is suspected, I would immediately order a CT scan of the chest with contrast to evaluate for mediastinal injury.
Failing to emphasize the life-threatening nature of the airway symptoms. Candidates often jump to physical exam maneuvers without securing the airway or performing a full trauma survey. Some omit the need for a CT angiogram, failing to realize the medial clavicle's proximity to the great vessels.
I would treat this as a potential medical emergency. After ensuring airway stability, I would obtain a CT chest with IV contrast as the gold standard to assess the relationship of the medial clavicle to the retrosternal structures (the "danger zone"). I would explicitly mention that this is a posterior dislocation until proven otherwise, given the patient's symptoms of dyspnea and the mechanism of injury.
You have confirmed a posterior sternoclavicular dislocation on CT. The patient is stable, but there is clear indentation behind the sternal notch. Describe the surgical anatomy you need to be aware of and the potential pitfalls of an open approach.
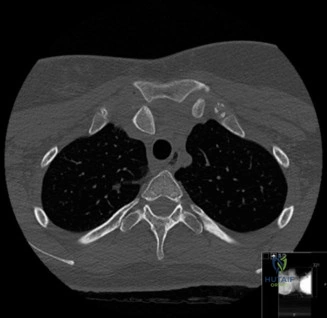
Candidate: The retrosternal "danger zone" contains the innominate artery and vein, trachea, and esophagus, often within 5-10mm of the clavicle. During an open approach, the primary pitfall is iatrogenic injury to these structures during dissection or drilling. I must use a malleable retractor posteriorly at all times to shield these vessels.
Forgetting to mention the specific need for a cardiothoracic or vascular surgeon to be on standby. Candidates often focus purely on the orthopedic hardware and forget the necessity of a multidisciplinary team for this specific injury.
Anatomically, I am concerned about the innominate vessels and the trachea. I would emphasize: 1. Strict use of posterior malleable retractors. 2. Mandatory presence of vascular/cardiothoracic surgery support in the OR. 3. Avoiding any pin fixation due to the risk of migration. 4. Using a soft-tissue figure-of-eight reconstruction (Spencer & Kuhn technique) rather than metal hardware.
You are in the operating theater for an open reduction. The clavicle is unstable after reduction. Describe your method of fixation and why you avoid older techniques.

Candidate: I would perform a figure-of-eight reconstruction using a tendon graft (e.g., semitendinosus). I avoid K-wires or Steinman pins because they are associated with catastrophic migration into the heart or great vessels, which has been well-documented in literature.
Suggesting "K-wires with a bend at the end" to prevent migration. The examiner will immediately flag this as unacceptable practice in modern orthopedics.
I would use a soft-tissue reconstruction (Spencer & Kuhn technique). I would create drill tunnels in the manubrium and clavicle (15mm from the joint) and pass the graft in a figure-of-eight. Transarticular metal fixation is absolutely contraindicated due to the lethal risk of migration. I would also mention that the costoclavicular ligament is the primary stabilizer I am attempting to augment.
The patient is a 20-year-old athlete. Looking at this radiograph, what is the most important diagnostic consideration before you assume this is a dislocation?
Candidate: In a patient aged 20, I must consider a physeal injury. The medial clavicular physis does not close until age 22 to 25. Therefore, what appears to be a dislocation is often a Salter-Harris type I or II fracture of the medial clavicular epiphysis.
Ignoring the age of the patient and assuming it is a true ligamentous dislocation. Failing to mention the late closure of the medial clavicular physis.
I must rule out a Salter-Harris physeal fracture. Because the medial clavicle is the last physis to fuse (up to 25 years), we often see "pseudo-dislocations" where the metaphysis displaces while the epiphysis remains in the joint. This requires a high index of suspicion on CT to differentiate between a true joint disruption and a physeal injury.
