Sternoclavicular & Patellar Instability: Surgical Guide
Key Takeaway
Sternoclavicular joint dislocations present unique clinical challenges. Anterior dislocations are typically managed conservatively, whereas posterior dislocations represent true orthopedic emergencies due to the proximity of vital mediastinal structures. Conversely, iatrogenic medial patellar instability often results from excessive lateral retinacular release, necessitating precise surgical reconstruction. This guide details the biomechanics, indications, and step-by-step operative techniques for managing both complex pathologies.
Comprehensive Introduction and Patho-Epidemiology
The surgical management of articular instability encompasses a diverse spectrum of pathologies, ranging from high-energy traumatic disruptions to insidious iatrogenic complications. This chapter comprehensively addresses two distinct, yet equally challenging, clinical entities: Sternoclavicular Joint (SCJ) instability and Iatrogenic Medial Patellar Instability. Although anatomically disparate, both conditions demand a profound understanding of precise ligamentous biomechanics, meticulous preoperative planning, and exacting surgical execution to restore native joint kinematics and prevent catastrophic morbidity.
Sternoclavicular joint instability is a relatively rare phenomenon, accounting for less than 3% of all shoulder girdle injuries. The SCJ serves as the sole true synovial articulation bridging the appendicular skeleton of the upper extremity with the axial skeleton. Traumatic dislocations of the SCJ present a stark clinical dichotomy. Anterior dislocations, typically resulting from an indirect lateral compressive force that levers the medial clavicle anteriorly, are generally benign and amenable to conservative management. Conversely, posterior dislocations, caused by a direct anteromedial blow or a compressive force rolling the shoulder forward, are true orthopedic emergencies. The posterior displacement of the medial clavicle places critical mediastinal structures—including the subclavian vessels, innominate vein, trachea, esophagus, and brachial plexus—at immediate risk of compression or laceration. Furthermore, the clinician must maintain a high index of suspicion in patients under 25 years of age, as the medial clavicular epiphysis is the last physis to fuse in the human body (typically between ages 22 and 25). In this demographic, what radiographically or clinically mimics an SCJ dislocation is frequently a Salter-Harris type I or II physeal fracture.
Atraumatic anterior subluxation of the SCJ represents a separate patho-epidemiological cohort. Predominantly observed in young females, this condition is frequently associated with generalized ligamentous laxity syndromes, such as Ehlers-Danlos syndrome, Marfan syndrome, or benign joint hypermobility syndrome. Provoked by specific positional maneuvers like shoulder abduction and extension, this subluxation is usually painless but accompanied by a disconcerting mechanical "clunk." Operative intervention in this specific demographic is universally condemned, as it invariably leads to surgical failure, recurrent instability, and severe iatrogenic morbidity.
In stark contrast to the traumatic etiology of SCJ dislocations, medial patellar instability in the virgin knee is an exceedingly rare pathology. Rather, it is almost exclusively an iatrogenic complication stemming from an overzealous, unwarranted, or technically flawed lateral retinacular release (LRR). Historically performed with high frequency for anterior knee pain or lateral patellar compression syndrome, LRR destroys the vital lateral tether of the patella. Consequently, the unopposed dynamic pull of the vastus medialis obliquus (VMO) and the medial patellofemoral ligament (MPFL) forces the patella to subluxate medially during early knee flexion. The modern orthopedic surgeon must be acutely aware of this iatrogenic epidemic, as diagnosing and reconstructing the medialized patella requires a complex reversal of the previous surgical insult, demanding sophisticated soft-tissue and osseous realignment strategies.
Detailed Surgical Anatomy and Biomechanics
Sternoclavicular Joint Anatomy and Kinematics
The sternoclavicular joint is a diarthrodial saddle joint characterized by profound osseous incongruity. Less than half of the medial clavicular articular surface maintains contact with the shallow clavicular notch of the manubrium. Consequently, the joint relies almost entirely on its robust capsuloligamentous complex for stability. This complex comprises the anterior and posterior sternoclavicular ligaments, the interclavicular ligament, and the extra-articular costoclavicular (rhomboid) ligament. The posterior sternoclavicular ligament is the thickest and biomechanically most critical structure, serving as the primary restraint against both anterior and posterior translation of the medial clavicle.
The costoclavicular ligament, consisting of anterior and posterior fascicles, anchors the inferior aspect of the medial clavicle to the first rib and its costal cartilage. It acts as a pivotal fulcrum during shoulder elevation and acts as the primary restraint to superior displacement of the proximal clavicle. An intra-articular fibrocartilaginous disc bisects the joint space, enhancing congruency and acting as a vital shock absorber. This disc is firmly attached to the first costal cartilage inferiorly and the superoposterior aspect of the clavicle proximally, effectively preventing medial displacement of the clavicle over the manubrium.
Biomechanically, the SCJ is remarkably mobile, participating in every movement of the upper extremity. It allows for approximately 35 degrees of upward elevation, 35 degrees of anterior-posterior excursion, and up to 50 degrees of axial rotation. Because of this extensive multi-planar motion, surgical fusion (arthrodesis) of the SCJ is poorly tolerated and severely restricts global shoulder kinematics, making ligamentous reconstruction the gold standard for chronic instability.
Patellofemoral Joint Lateral Restraints
The patellofemoral joint is a complex articulation governed by intricate dynamic and static stabilizers. While the medial structures (primarily the MPFL) have garnered significant attention, the lateral structures are equally vital for maintaining central patellar tracking within the trochlear groove. The lateral retinaculum is a bi-layered structure. The superficial layer consists of the oblique retinaculum, which originates from the iliotibial band (ITB) and interdigitates with the vastus lateralis aponeurosis. The deep layer comprises the deep transverse retinaculum, the epicondylopatellar ligament, and the patellotibial ligament.
The vastus lateralis (VL) and the vastus lateralis obliquus (VLO) provide the dynamic lateral pull that counterbalances the VMO. When an iatrogenic lateral retinacular release is performed, the deep transverse retinaculum and the lateral patellotibial ligament are transected. If the release extends too proximally, the VLO and VL tendon are compromised. This catastrophic loss of the lateral tether disrupts the delicate coronal plane equilibrium. As the knee flexes from 0 to 30 degrees—the critical phase before the patella fully engages the bony stability of the trochlear groove—the unopposed medial vectors dynamically subluxate the patella medially. This abnormal tracking leads to severe medial articular shear stress, progressive chondromalacia, and the classic clinical presentation of iatrogenic medial patellar instability.
Exhaustive Indications and Contraindications
The decision-making process for surgical intervention in both SCJ and patellar instability requires a rigorous evaluation of the patient's history, pathoanatomy, and functional demands. The following table delineates the strict indications and absolute contraindications for operative management.
| Pathology | Surgical Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Anterior SCJ Dislocation | Chronic, unremitting pain failing >6 months conservative care; Impending skin necrosis from medial clavicular prominence; Severe cosmetic deformity in highly selected patients. | Atraumatic, voluntary, or habitual subluxation (e.g., Ehlers-Danlos); Acute asymptomatic anterior dislocation. | Poor soft tissue envelope; Active systemic infection; Non-compliant patient. |
| Posterior SCJ Dislocation | Acute posterior dislocation (urgent closed reduction); Failed closed reduction; Hemodynamic instability or mediastinal compression (stridor, dysphagia, neurovascular deficit); Chronic symptomatic posterior dislocation. | Lack of cardiothoracic surgical backup; Use of K-wires or Steinmann pins across the SCJ (Absolute risk of fatal migration). | Asymptomatic chronic posterior dislocation discovered incidentally in low-demand patients. |
| Iatrogenic Medial Patellar Instability | Symptomatic medial subluxation confirmed on physical exam (positive medial apprehension/gravity subluxation test) failing conservative management; Documented history of prior lateral retinacular release. | Primary lateral patellar instability; Advanced, bone-on-bone patellofemoral osteoarthritis; Active knee joint infection. | Uncorrected severe coronal or axial plane malalignment (e.g., profound femoral anteversion); Complex regional pain syndrome (CRPS). |
Rationale for Sternoclavicular Interventions
Anterior SCJ dislocations are notoriously difficult to maintain in a reduced position using closed methods. However, because the functional impairment of an unreduced anterior dislocation is negligible and the surgical complication rate is historically high, benign neglect with early mobilization remains the treatment of choice. Conversely, posterior dislocations carry a mortality risk if left untreated due to the proximity of the great vessels. Up to 30% of posterior dislocations present with life-threatening complications, dictating emergent reduction. Open reduction is mandated when soft tissue interposition (often the joint capsule or the intra-articular disc) blocks closed reduction.
Rationale for Patellar Interventions
In the setting of iatrogenic medial patellar instability, conservative management (bracing, VMO stretching, lateral strengthening) is almost universally futile once the lateral structures have been structurally ablated. Surgical intervention is dictated by the precise nature of the previous iatrogenic insult. If the lateral release was recent and tissue quality permits, a direct repair or advancement of the vastus lateralis is indicated. If a previous distal realignment (e.g., Fulkerson osteotomy) excessively medialized the tibial tubercle, a revision osteotomy to lateralize the tubercle is required. For chronic cases with deficient lateral tissues, a structural reconstruction using a lateral patellar tendon strip is the definitive indication.
Pre-Operative Planning, Templating, and Patient Positioning
Sternoclavicular Joint Pre-Operative Protocol
Standard orthogonal radiography of the SCJ is notoriously difficult to interpret due to the superimposition of the ribs, sternum, and mediastinal structures. While the "Serendipity view"—an anteroposterior projection with the X-ray beam tilted 40 degrees cephalad—can help differentiate anterior from posterior displacement, it is insufficient for definitive surgical planning.
A Computed Tomography (CT) scan of the chest with intravenous contrast is the absolute gold standard and is mandatory for all suspected posterior dislocations. The CT scan provides multiplanar reconstructions that definitively characterize the direction of dislocation, differentiate true dislocations from medial clavicular physeal fractures, and most importantly, evaluate the integrity and proximity of the great vessels. The surgeon must meticulously template the medial clavicle and manubrium to plan drill hole trajectories for the figure-of-eight reconstruction, ensuring the retrosternal cortex is breached safely.
Patient Positioning: The patient is placed in the supine position on a radiolucent operating table. A thick sandbag or a tightly rolled towel is placed longitudinally between the scapulae. This critical maneuver allows the bilateral shoulders to fall posteriorly, opening the anterior chest wall and facilitating the reduction of the medial clavicle. The entire chest, neck, and bilateral upper extremities are prepped and draped to allow for intraoperative manipulation. Furthermore, an ipsilateral lower extremity is prepped and draped to facilitate the harvest of a semitendinosus or gracilis autograft. It is an absolute requirement that a cardiothoracic surgeon is either scrubbed or immediately available on standby in the operating room prior to making the incision.
Patellofemoral Joint Pre-Operative Protocol
Pre-operative imaging for iatrogenic medial patellar instability must include a comprehensive radiographic series: weight-bearing anteroposterior, true lateral (at 30 degrees of flexion to assess patellar height via the Caton-Deschamps index), and axial Merchant views. Magnetic Resonance Imaging (MRI) is critical to assess the extent of the previous lateral release, the quality of the remaining lateral retinacular tissue, and the status of the patellofemoral articular cartilage. A CT scan is often utilized to calculate the Tibial Tubercle-Trochlear Groove (TT-TG) distance; an excessively small or negative TT-TG distance may indicate a previous over-medialization osteotomy that requires revision.
Patient Positioning: The patient is positioned supine on the operating table. A high-thigh tourniquet is applied but optimally left uninflated unless visualization is compromised, allowing for dynamic assessment of patellar tracking. A lateral thigh post is placed, and the foot is secured in a sterile limb positioner to allow for unrestricted knee flexion from 0 to 120 degrees. The contralateral limb is carefully padded and secured.
Step-by-Step Surgical Approach and Fixation Technique
Posterior Sternoclavicular Joint: Closed Reduction
Closed reduction should be attempted for acute posterior dislocations (less than 3 weeks old) under general anesthesia with complete muscle relaxation.
1. Traction and Extension: With the interscapular bump in place, the affected arm is abducted to 90 degrees and extended. The surgeon applies sustained, inline axial traction.
2. Manipulation: If traction alone fails to disengage the medial clavicle from behind the manubrium, the surgeon percutaneously grasps the medial clavicle using a sterile, heavy towel clip.
3. Anterior Translation: While an assistant maintains axial traction, the surgeon physically lifts the medial clavicle anteriorly to clear the manubrial rim. A palpable and audible "clunk" typically signifies reduction.
4. Stability Assessment: Once reduced, posterior dislocations are usually stable due to the intact anterior capsular hinge. The joint is immobilized in a figure-of-eight brace for 4 to 6 weeks.
Posterior Sternoclavicular Joint: Open Reconstruction
If closed reduction fails or the injury is chronic, open reduction and autograft reconstruction are indicated.
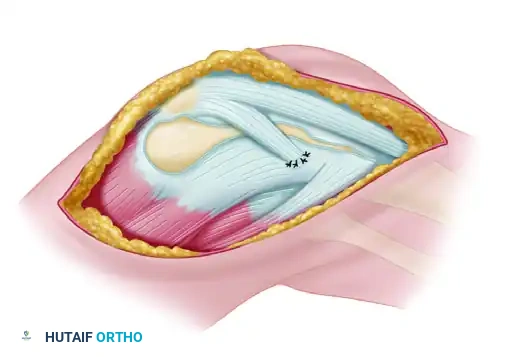
1. Surgical Approach: A 7-cm transverse incision is made centered over the SCJ, extending from the medial third of the clavicle to the center of the manubrium. The platysma is divided, and full-thickness fasciocutaneous flaps are elevated. The periosteum is meticulously preserved.
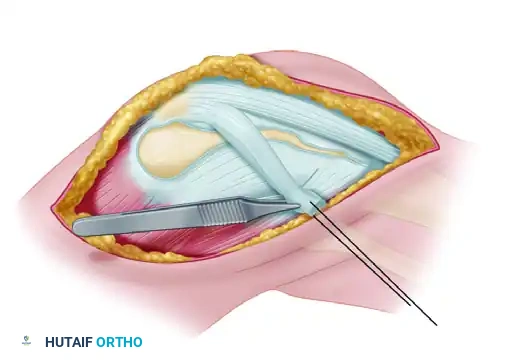
2. Retrosternal Protection: The medial clavicle is carefully mobilized. A blunt, curved retractor (such as a malleable ribbon or a specialized sternal retractor) is carefully passed posterior to the medial clavicle and manubrium to protect the innominate vein and pleura during drilling.
3. Graft Harvest and Preparation: A semitendinosus or gracilis autograft is harvested from the ipsilateral knee, whipstitched at both ends, and sized.
4. Drill Tunnels: Using a 4.0 mm or 4.5 mm drill bit, two osseous tunnels are created in the medial clavicle (superior to inferior) and two corresponding tunnels are created in the manubrium. The drill must be advanced with extreme caution, utilizing the protective retrosternal retractor as a backstop.
5. Figure-of-Eight Fixation: The autograft is passed through the clavicular and manubrial tunnels in a figure-of-eight configuration. The joint is manually reduced, and the graft is tensioned and sutured to itself using heavy, non-absorbable braided suture.
6. Absolute Contraindication Reminder: Under no circumstances should Kirschner wires (K-wires) or Steinmann pins be utilized to stabilize the SCJ. The repetitive micro-motion of the shoulder girdle universally leads to hardware breakage and catastrophic intrathoracic migration into the heart, aorta, or lungs.
Iatrogenic Medial Patellar Instability: Patellar Tendon Reconstruction
When inadequate lateral tissues remain for primary repair, a structural reconstruction using the lateral portion of the patellar tendon is executed to create a robust lateral tether.
Step 1: Positioning and Exposure
Following exsanguination and tourniquet inflation, a standard anterolateral incision is utilized, incorporating previous surgical scars to minimize skin necrosis. Full-thickness fasciocutaneous flaps are elevated to widely expose the extensor mechanism, the patella, the patellar tendon, and the lateral tibial metaphysis.
Step 2: Graft Harvest
A lateral one-quarter strip (approximately 5 to 7 mm in width) of the patellar tendon is sharply developed. The incision begins at the inferolateral pole of the patella and extends distally to the tibial tubercle. The strip is sharply detached from its distal osseous insertion on the tibial tubercle but is left meticulously attached proximally to the inferolateral pole of the patella, maintaining its native blood supply and structural anchor.
Step 3: Graft Routing and Preparation
The detached distal end of the patellar tendon strip is mobilized. A heavy non-absorbable running locking suture (e.g., #2 FiberWire or similar ultra-high-molecular-weight polyethylene suture) is woven into the free distal end of the graft using a Krackow or whipstitch technique. This allows for precise tensioning and subsequent fixation.
Step 4: Fixation to the Lateral Tibial Tubercle
The graft is routed laterally and distally, effectively recreating the vector of the deep transverse retinaculum and the lateral patellotibial ligament. The strip is attached at the lateral tibial tubercle or the lateral metaphysis of the tibia. Fixation is achieved either by direct suturing to the robust local periosteum, passing the graft through a transosseous bony tunnel, or utilizing a biocomposite suture anchor.
SURGICAL PEARL:
Tensioning of the graft is the most critical and unforgiving step of the procedure. The graft must be tensioned with the knee flexed to exactly 30 degrees. It should be tensioned just enough to prevent medial subluxation past the medial trochlear ridge. Over-tensioning will cause iatrogenic lateral compression, severe patellofemoral pain, and restricted normal patellar tracking.
Step 5: Closure
The tourniquet is deflated, and meticulous hemostasis is obtained to prevent postoperative hemarthrosis. The wound is irrigated copiously with sterile saline. The subcutaneous tissues are closed in layers with absorbable sutures, and the skin is reapproximated with a subcuticular stitch or surgical staples.
Complications, Incidence Rates, and Salvage Management
Surgical interventions for both SCJ and patellar instability are fraught with potential complications. The surgeon must be prepared to manage these adverse events promptly and effectively. The table below outlines the most critical complications, their estimated incidence, and appropriate salvage strategies.
| Complication | Estimated Incidence | Etiology / Pathophysiology | Salvage Management / Resolution |
|---|---|---|---|
| Mediastinal Vascular Injury (SCJ) | 1 - 3% (Posterior Dislocations) | Penetration of the retrosternal space by drill bits, aberrant instruments, or the displaced clavicle itself causing laceration of the innominate vein or subclavian artery. | Immediate packing, emergent sternotomy by cardiothoracic surgery. Prevention via meticulous placement of retrosternal retractors is paramount. |
| Hardware Migration (SCJ) | Historical (High); Modern (Near 0% if avoided) | Use of K-wires or pins. Repetitive shoulder motion causes metal fatigue, breakage, and fatal migration into the heart or great vessels. | Absolute contraindication. If previously placed hardware is discovered, emergent surgical removal is required regardless of symptoms. |
| Recurrent SCJ Instability | 10 - 15% | Graft stretching, failure of fixation, or non-compliance with postoperative immobilization. | Revision reconstruction with allograft. In refractory cases with severe pain, a medial clavicle excision (resecting <1.5 cm to preserve the costoclavicular ligament) may be considered. |
| Iatrogenic Lateral Patellar Compression | 5 - 10% | Over-tensioning of the lateral patellar tendon graft during fixation, effectively recreating the pathology the original lateral release attempted to cure. | Aggressive physical therapy. If refractory, surgical re-exploration and controlled lengthening or release of the reconstructed graft. |
| Graft Failure / Recurrent Medial Instability | 5 - 8% | Fixation failure at the tibial metaphysis, poor tissue quality of the harvested patellar tendon, or failure to address underlying bony malalignment. | Revision reconstruction using semitendinosus allograft or revision of the tibial tubercle osteotomy to correct the TT-TG distance. |
| Post-Operative Arthrofibrosis (Knee) | 3 - 7% | Prolonged immobilization, excessive surgical trauma, or inadequate postoperative pain control preventing early range of motion. | Intensive physical therapy. If ROM is not achieved by 12 weeks, manipulation under anesthesia (MUA) or arthroscopic lysis of adhesions is indicated. |
Phased Post-Operative Rehabilitation Protocols
Successful outcomes following complex ligamentous reconstructions depend as much on strict adherence to a phased, biologically sound rehabilitation protocol as they do on the surgical execution itself. The rehabilitation must balance the need to protect the healing graft with the necessity of restoring early range of motion to prevent arthrofibrosis.
Sternoclavicular Joint Reconstruction Rehabilitation
Phase I: Maximum Protection (Weeks 0-6)
Immediately postoperatively, the patient is placed in a figure-of-eight brace or a customized shoulder immobilizer. Absolute restriction of shoulder elevation above 60 degrees and avoidance of cross-body adduction are mandatory to prevent catastrophic stress on the figure-of-eight autograft. Passive range of motion (PROM) of the elbow, wrist, and hand is initiated immediately. Gentle pendulum exercises may begin at week 4 under the strict supervision of a physical therapist.
Phase II: Moderate Protection and Active Motion (Weeks 6-12)
The immobilizer is discontinued. Active-assisted range of motion (AAROM) and active range of motion (AROM) are progressively introduced. The focus shifts to restoring scapulothoracic kinematics and periscapular muscle strength. Isotonic strengthening of the rotator cuff and deltoid begins at week 8, utilizing low-resistance, high-repetition protocols.
Phase III: Return to Function (Months 3-6)
Advanced strengthening and plyometric exercises are integrated. Heavy lifting, contact sports, and overhead athletic activities are strictly prohibited until at least 6 months postoperatively. Return to play is contingent upon achieving full, painless ROM and 90% strength symmetry compared to the contralateral shoulder.
Lateral Patellotibial Ligament Reconstruction Rehabilitation
Phase I: Maximum Protection (Weeks 0-4)
* Weight-Bearing: The patient is allowed touch-down weight-bearing (TDWB) with crutches to protect the tibial fixation site.
* Bracing: The knee is locked in full extension in a hinged knee brace for all ambulation and sleeping.
* Range of Motion: Passive range of motion (PROM) is initiated from 0 to 90 degrees. Active knee extension is strictly avoided to prevent eccentric stress on the healing lateral graft and the extensor mechanism.
* Exercises: Isometric quadriceps sets, straight leg raises (performed strictly within the locked brace to prevent extensor lag), and ankle pumps for deep vein thrombosis (DVT) prophylaxis.
Phase II: Moderate Protection (Weeks 4-8)
* Weight-Bearing: Progress to full weight-bearing as tolerated.
* Bracing: The brace is unlocked to allow functional ROM during ambulation. The brace is eventually discontinued entirely once quadriceps control is deemed adequate (defined as the ability to perform a straight leg raise with zero degrees of extensor lag).
* Range of Motion: Progress to full active and passive ROM.
* Exercises: Closed kinetic chain exercises (e.g., mini-squats, leg presses) are initiated to stimulate quadriceps hypertrophy without inducing high patellofemoral shear forces. Open kinetic chain knee extension remains contraindicated.
Phase III: Return to Function (Weeks 8-16)
* Strengthening: Advanced strengthening focusing on the entire kinetic chain, specifically targeting the core, gluteal, and quadriceps musculature.
* Proprioception: Balance board, single-leg stabilization, and agility drills are introduced.
* Return to Sport: Patients may begin a gradual return to sports-specific activities between 4 and 6 months postoperatively. Clearance is provided only when the patient has achieved at least a 90% limb symmetry index on functional hop testing and demonstrates absolutely no clinical signs of recurrent instability or apprehension.
Summary of Landmark Literature and Clinical Guidelines
The evolution of surgical management for both SCJ and patellar instability is deeply rooted in landmark orthopedic literature. A comprehensive understanding of these foundational texts is essential for any practicing orthopedic surgeon or resident preparing for board examinations.
Regarding the Sternoclavicular Joint, the seminal work by Wirth and Rockwood established the modern classification system for SCJ injuries and definitively outlined the catastrophic risks associated with transarticular pin fixation. Their extensive review of the literature highlighted numerous fatalities secondary to K-wire migration into the mediastinum, cementing the absolute contraindication that governs modern practice. Furthermore, Groh et al. popularized the figure-of-eight semitendinosus autograft reconstruction technique. Their long-term outcome studies demonstrated superior biomechanical stability and clinical outcomes compared to subclavius tendon transfers or primary ligamentous repairs, establishing the figure-of-eight autograft as the gold standard for chronic SCJ instability.
In the realm of the patellofemoral joint, the historical context is critical. Hughston originally warned against the indiscriminate use of lateral retinacular releases, noting that destroying the lateral structures without addressing underlying bony malalignment (such as an increased Q-angle) would lead to unpredictable outcomes. Decades later, Nonweiler and DeLee provided the definitive clinical description of iatrogenic medial patellar instability, coining the term and describing the classic physical examination findings, including the gravity subluxation test. More recently, literature focusing on lateral patellotibial ligament reconstruction—specifically utilizing the lateral strip of the patellar tendon—has demonstrated excellent survivorship and patient-reported outcomes. These contemporary studies emphasize that restoring the precise anatomical vector of the deep transverse retinaculum is paramount to re-establishing normal patellofemoral kinematics and resolving the debilitating symptoms of medial subluxation.
