Sternoclavicular Joint Dislocation: Acute Repair & Reconstruction Masterclass
Key Takeaway
This masterclass provides a comprehensive, immersive guide to sternoclavicular joint dislocation repair. We'll delve into intricate surgical anatomy, meticulous preoperative planning, and granular intraoperative execution. Learn precise reduction maneuvers, ligament reconstruction techniques, and critical strategies to manage potential complications. This detailed narrative, from a scrubbed-in perspective, emphasizes safety, efficacy, and optimal patient outcomes for this rare yet challenging injury.
Comprehensive Introduction and Patho-Epidemiology
Sternoclavicular (SC) joint dislocations represent one of the rarer, yet profoundly challenging, injuries encountered in the realm of orthopedic trauma. Accounting for a mere 3% of all shoulder girdle injuries, the relative infrequency of this pathology belies the significant morbidity and potential mortality associated with it. As orthopedic surgeons, it is an absolute certainty that we will encounter this injury pattern, particularly in Level I trauma centers managing high-energy mechanisms such as motor vehicle collisions, equestrian accidents, and high-impact contact sports. The SC joint is the sole true diarthrodial articulation linking the appendicular skeleton of the upper extremity to the axial skeleton, bearing massive biomechanical loads while possessing the least intrinsic bony stability of any major joint in the human body.
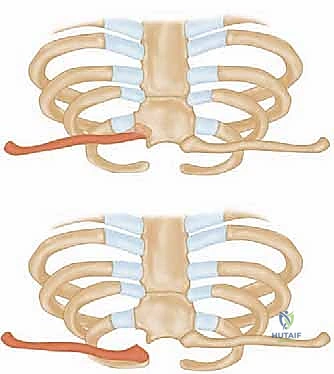
The epidemiological distribution of these injuries heavily favors anterior dislocations, with contemporary series reporting anterior-to-posterior dislocation ratios ranging from 3:1 to as high as 20:1. The mechanism of injury dictates the direction of displacement. Anterior dislocations typically result from an indirect force—specifically, a lateral compressive force applied to the shoulder girdle while the shoulder is rolled backward in extension. Conversely, posterior dislocations result either from a direct, high-energy blow to the anteromedial clavicle, or an indirect lateral compressive force applied while the shoulder is rolled forward in flexion. While anterior dislocations present a prominent, often cosmetically displeasing deformity, they are rarely life-threatening and can frequently be managed with non-operative, symptomatic care.
Posterior dislocations, however, represent a true orthopedic emergency. The posterior displacement of the medial clavicle drives the bone directly into the superior mediastinum, placing a dense network of vital neurovascular and visceral structures at immediate risk. Up to 30% of patients with posterior SC joint dislocations will present with symptoms of mediastinal compression. These symptoms can range from venous congestion and diminished ipsilateral upper extremity pulses to severe dyspnea, dysphagia, dysphonia, or a choking sensation. The potential for catastrophic injury to the brachiocephalic vessels, trachea, and esophagus mandates a high index of suspicion, rapid diagnostic evaluation, and urgent, definitive management.
Furthermore, the diagnosis of SC joint pathology is frequently delayed or missed entirely during the initial trauma evaluation. In the polytraumatized patient, the subtle clinical signs of an SC joint injury are easily overshadowed by more dramatic appendicular fractures, traumatic brain injuries, or blunt thoracic trauma. Standard anteroposterior chest radiographs are notoriously poor at visualizing the SC joint due to the superimposition of the ribs, spine, and mediastinal shadow. Therefore, mastering the clinical examination, understanding the precise patho-anatomy, and utilizing advanced imaging modalities are paramount for the modern orthopedic surgeon to prevent disastrous outcomes.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel ever touches the skin, the orthopedic surgeon must possess an encyclopedic understanding of the intricate, high-stakes anatomy surrounding the sternoclavicular joint. This region is often termed a "critical zone" due to the dense packing of vital structures within millimeters of the articular surface. The medial epiphysis of the clavicle is a fascinating and clinically vital structure. It is the very last long bone epiphysis in the human body to ossify, typically appearing between the ages of 18 and 20, and it does not completely fuse until 23 to 25 years of age. This developmental timeline is a critical diagnostic trap: in young adults under the age of 25, what appears clinically and radiographically to be a true SC joint dislocation is statistically much more likely to be a Salter-Harris type I or II physeal fracture. This distinction fundamentally alters our management algorithm, as physeal fractures have massive remodeling potential and often heal impeccably with closed management, whereas true ligamentous dislocations do not heal with intrinsic stability.
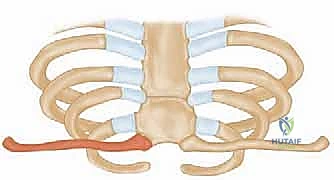
The articular surface of the medial clavicle is bulbous, demonstrating a concave profile in the anteroposterior plane and a convex profile in the vertical plane. This articulates with the reciprocally curved clavicular notch of the manubrium sterni, forming a classic saddle-type joint. The bony congruence is exceptionally poor; less than half of the medial clavicle actually articulates with the sternum at any given time. This inherent osseous instability underscores the joint's absolute reliance on its complex ligamentous envelope. A small articular facet on the inferior aspect of the medial clavicle may also articulate with the cartilage of the first rib in a small percentage of individuals, adding a layer of anatomical variance.
The ligamentous stabilizers of the SC joint are robust and multifaceted. The capsular ligaments are intrinsic thickenings of the joint capsule, enveloping the anterosuperior and posterior aspects. Biomechanical studies have unequivocally demonstrated that the posterior capsule is the single most important primary stabilizer against both anterior and posterior translation of the medial clavicle. The anterior capsule, while significant, is a secondary restraint. The interclavicular ligament spans the superomedial aspects of both clavicles, attaching to the capsular ligaments and the upper margin of the sternum. Functioning much like a wishbone, it contributes to "shoulder poise" by resisting downward glide of the lateral clavicle. The intra-articular disc ligament is a dense, fibrocartilaginous structure that arises from the synchondral junction of the first rib and sternum, passing completely through the joint cavity and attaching to the superior and posterior aspects of the medial clavicle. It effectively divides the joint into two separate synovial spaces and acts as a critical checkrein against medial displacement of the clavicle.
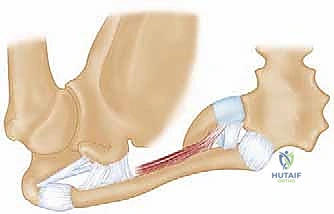
The costoclavicular, or rhomboid, ligament is a massive, extra-articular stabilizer. It originates from the upper surface of the medial first rib and inserts into the rhomboid fossa on the inferior surface of the medial clavicle. It consists of two distinct fasciculi: the anterior fasciculus, which runs upward and laterally to resist lateral displacement and upward rotation, and the posterior fasciculus, which runs upward and medially to resist medial displacement and downward rotation. While the costoclavicular ligament is relatively unloaded when the primary capsular ligaments are intact, it becomes the crucial secondary restraint in the event of capsular rupture, functioning analogously to the coracoclavicular ligaments in acromioclavicular joint dislocations.
The neurovascular anatomy posterior to the SC joint is the primary reason posterior dislocations are feared. Directly behind the joint lies a "curtain of muscles" comprising the sternohyoid, sternothyroid, and scalene muscles. These muscles obscure the surgeon's view of the superior mediastinum. Immediately posterior to this muscular curtain lie the innominate (brachiocephalic) artery and vein, the superior vena cava, the arch of the aorta, the right pulmonary artery, the trachea, the esophagus, and the vagus and phrenic nerves. A posterior dislocation can compress or lacerate any of these structures. Anteriorly, superficial to the joint capsule but deep to the platysma, lies the anterior jugular vein. This vessel is highly variable, can reach up to 1.5 cm in diameter, and lacks valves. Inadvertent laceration during the surgical approach can result in massive, difficult-to-control hemorrhage, emphasizing the need for meticulous, layer-by-layer dissection.
Exhaustive Indications and Contraindications
The decision-making process for operative intervention in SC joint dislocations requires a nuanced understanding of the injury chronicity, direction of displacement, patient age, and functional demands. The management algorithm is distinctly different for anterior versus posterior dislocations, and for acute versus chronic presentations.
Acute anterior dislocations are almost universally managed non-operatively. While closed reduction can occasionally be achieved with posterior pressure and shoulder retraction, the injury is notoriously unstable, and the clavicle typically re-dislocates immediately upon removal of pressure. However, numerous long-term outcome studies have demonstrated that despite the persistent cosmetic deformity, the vast majority of patients with unreduced anterior SC joint dislocations regain full, painless range of motion and return to their pre-injury level of function. Therefore, primary operative stabilization for an acute anterior dislocation is rarely indicated, reserved only for extreme cases of skin tenting threatening necrosis, or in high-level overhead athletes who demand absolute anatomical restoration and understand the significant surgical risks.
Acute posterior dislocations, conversely, demand immediate attention. Closed reduction should be attempted urgently, ideally within the first 48 hours, in a controlled environment such as the operating room with general anesthesia and cardiothoracic surgery available on immediate standby. The classic reduction maneuver involves placing a bump between the patient's scapulae, applying lateral traction to the abducted and extended arm, and utilizing a sterile towel clip to physically grasp the medial clavicle and lift it anteriorly. If closed reduction is successful, the joint is often stable, and non-operative management in a figure-of-eight harness or sling is appropriate. Operative intervention is strictly indicated when an acute posterior dislocation is irreducible by closed means, when it is highly unstable post-reduction, or when there are progressive signs of mediastinal compression (vascular compromise, dyspnea, dysphagia) that do not resolve with reduction attempts.
| Clinical Scenario | Indications for Operative Management | Contraindications for Operative Management |
|---|---|---|
| Acute Anterior Dislocation | - Impending skin necrosis from severe tenting - Polytrauma requiring upper extremity weight-bearing - Elite overhead athlete (relative indication) |
- Asymptomatic deformity - Medically unstable polytrauma patient - Patient unwilling to comply with strict rehab |
| Acute Posterior Dislocation | - Irreducible by closed manipulation - Unstable after successful closed reduction - Persistent mediastinal compression (vascular, airway) - Open dislocation |
- Stable after closed reduction - Medically unfit for general anesthesia - Delayed presentation (>3 weeks) without symptoms |
| Chronic Dislocation (>3 weeks) | - Severe, debilitating pain limiting ADLs - Thoracic outlet syndrome symptoms - Late-onset dysphagia or dyspnea (posterior) |
- Painless cosmetic deformity (anterior) - Mild, manageable discomfort - Active local or systemic infection |
| Medial Physeal Fracture (<25 yrs) | - Severe posterior displacement with mediastinal compromise irreducible by closed means | - Acceptable alignment after closed reduction - Anterior displacement (remodels excellently) |
Chronic dislocations present a different challenge. A chronic anterior dislocation that is asymptomatic requires no intervention; attempting to reconstruct a painless deformity exposes the patient to unnecessary surgical risk. However, if a chronic anterior or posterior dislocation remains severely painful, significantly limits shoulder function, or causes delayed neurovascular compromise, operative reconstruction is indicated. It is critical to note that in chronic cases, primary repair of the native ligaments is impossible due to tissue retraction and scarring; a robust biological reconstruction utilizing autograft or allograft is mandatory to restore stability.
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the bedrock of safe and successful sternoclavicular joint surgery. The complex, overlapping osseous anatomy of the upper thorax renders standard plain radiography insufficient for definitive surgical planning. While the "Serendipity view"—an anteroposterior projection with the X-ray tube tilted 40 degrees cephalad and centered on the manubrium—can provide a rapid assessment of superior/inferior translation and gross anterior/posterior displacement, it lacks the resolution required for operative templating.

In the Serendipity view, an anteriorly dislocated medial clavicle will appear to ride higher than the normal contralateral side, while a posteriorly dislocated clavicle will project lower than the normal side. However, this view is highly dependent on perfect patient positioning and technician skill, making it prone to misinterpretation.

The absolute gold standard, and a non-negotiable prerequisite for surgical intervention, is a high-resolution Computed Tomography (CT) scan. The CT protocol must encompass both sternoclavicular joints and the medial halves of both clavicles to allow for precise contralateral comparison. Axial, coronal, and sagittal reformats, along with 3D surface-rendered reconstructions, are essential. The CT scan definitively differentiates a true ligamentous dislocation from a medial physeal fracture, quantifies the exact degree and vector of displacement, and assesses the integrity of the articular surfaces.
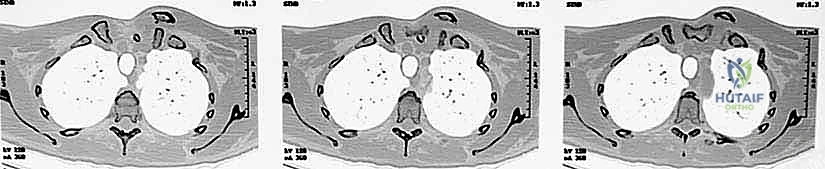
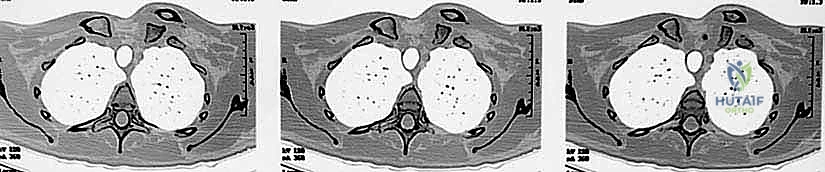
Crucially, in the setting of a posterior dislocation, the CT scan must be performed with intravenous contrast. This "CT Angiogram" phase is vital to delineate the relationship of the displaced medial clavicle to the innominate vessels, the superior vena cava, and the aorta. It identifies pseudoaneurysms, intimal tears, or direct vascular compression that would mandate the immediate presence of a cardiothoracic or vascular surgeon during the exposure. The surgeon must template the anticipated drill hole trajectories for the reconstruction, ensuring they remain safely within the osseous confines of the manubrium and clavicle, directing the drill bit away from the mediastinum at all times.
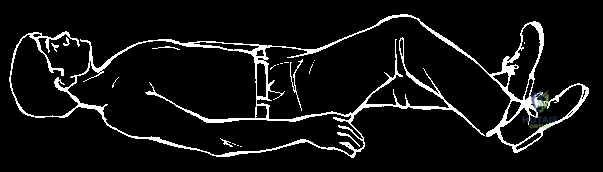
Patient positioning in the operating room requires meticulous attention to detail. The patient is placed in the supine position on a radiolucent operating table. A rolled towel or a specifically designed gel bump is placed vertically between the scapulae. This maneuver allows the shoulders to fall posteriorly, effectively opening up the anterior chest wall, retracting the lateral clavicle, and facilitating reduction of a posterior dislocation. The head is placed on a Mayfield horseshoe headrest or a standard foam donut, and the neck is slightly extended and rotated away from the operative side to maximize exposure of the sternocleidomastoid and the medial clavicular region.
The surgical prep must be extensive. It should extend from the mandible superiorly to the costal margin inferiorly, and from the contralateral nipple line across to encompass the entire ipsilateral upper extremity, allowing the arm to be draped free. This wide prep allows for manipulation of the arm to assist with reduction, provides access for potential graft harvest (if using the palmaris longus, though hamstring autograft or allograft is preferred), and prepares the chest for an emergent median sternotomy should a catastrophic vascular injury occur. The presence of a cardiothoracic surgeon in the hospital, and ideally in the operating suite for high-risk posterior dislocations, is a mandatory safety protocol.
Step-by-Step Surgical Approach and Fixation Technique
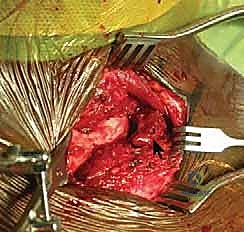
The surgical approach to the sternoclavicular joint requires a deep respect for the surrounding soft tissue envelope and the underlying vascular structures. A transverse or slightly curvilinear "hockey stick" incision is typically employed. The incision begins over the medial aspect of the clavicle, extending medially across the SC joint and curving slightly inferiorly over the midline of the manubrium. This provides excellent exposure of both the clavicular and sternal footprints of the capsular ligaments.

Dissection proceeds sharply through the subcutaneous tissue to the level of the platysma. The platysma is divided in line with the incision. Immediately deep to the platysma, the surgeon must be hyper-vigilant for the anterior jugular vein. This vessel is highly variable; if encountered, it should be carefully mobilized and retracted, or definitively ligated and divided to prevent massive hemorrhage during the deeper dissection. The medial fascia of the pectoralis major and the clavicular head of the sternocleidomastoid are identified. A subperiosteal dissection technique is strictly utilized to elevate these muscle attachments off the medial clavicle and the manubrium. Elevating full-thickness flaps preserves the vascularity of the bone and provides robust tissue for later closure.


Once the joint is exposed, the pathology is assessed. In an acute setting, the torn remnants of the anterior and posterior capsule are identified and tagged with heavy non-absorbable sutures. If the intra-articular disc is irreparably torn or blocking reduction, it may be excised, though preserving it is preferable if possible. Reduction of the joint is then performed under direct visualization. For a posterior dislocation, a bone hook or a robust towel clip is placed around the medial clavicle to pull it anteriorly and laterally, while an assistant applies lateral traction to the abducted arm.

SURGICAL WARNING: The Absolute Contraindication of Pin Fixation
It is an absolute, non-negotiable tenet of orthopedic surgery that smooth or threaded Kirschner wires, Steinmann pins, or any form of unconstrained wire fixation must never be used to stabilize the sternoclavicular joint. The dynamic forces of the shoulder girdle, combined with respiratory excursion, inevitably lead to hardware migration. Pins migrating posteriorly have caused fatal cardiac tamponade, aortic laceration, and tracheal perforation. The literature is replete with catastrophic, lethal complications from this historically flawed technique. Pin fixation of the SC joint is considered below the standard of care.
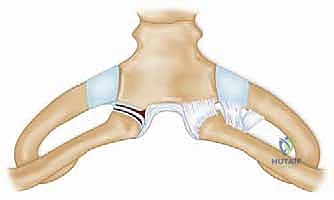
Modern stabilization relies on robust biological reconstruction. While primary repair of the capsule using suture anchors in the manubrium can augment the construct, a figure-of-eight graft reconstruction is the gold standard for restoring multiplanar stability. A semitendinosus or gracilis autograft (or allograft to minimize donor site morbidity) is preferred due to its length and tensile strength.


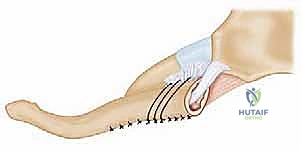
Drill holes, typically 4.0mm to 4.5mm in diameter, are meticulously created. In the medial clavicle, two holes are drilled from anterior to posterior, approximately 1 cm lateral to the articular margin and 1 cm apart. In the manubrium, two corresponding holes are drilled. Critical Step: When drilling the manubrium and the clavicle, a malleable retractor or a broad periosteal elevator must be placed deep to the bone to protect the mediastinal structures from the drill bit plunging. The drill must always be directed from anterior to posterior, with precise control.
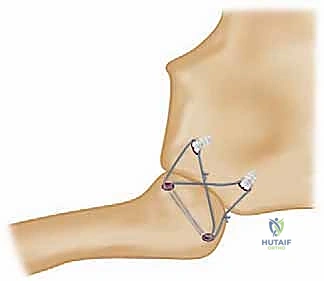
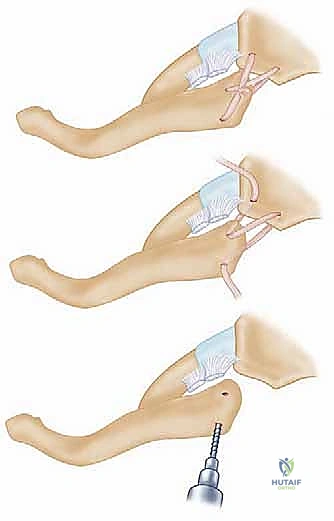
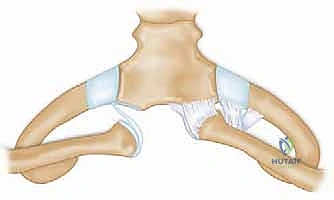
The graft is then passed in a figure-of-eight configuration. Suture passing wires or curved shuttles are used to navigate the graft through the osseous tunnels. The graft is tensioned with the clavicle held in anatomical reduction (often requiring downward and posterior pressure on the medial clavicle). The graft limbs are then sutured to themselves and to the surrounding periosteal tissues using heavy, non-absorbable, braided sutures.

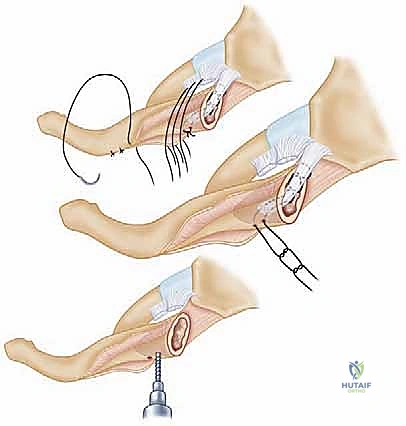
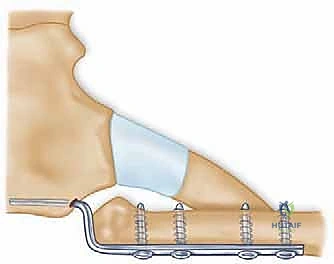
Some modern techniques utilize a "docking" method, where the graft is fixed into blind-ended sockets using biocomposite tenodesis screws, minimizing the need for posterior dissection and reducing the risk to mediastinal structures. Regardless of the specific graft routing, the final construct must be rigidly stable through a functional range of motion on the operating table.

Following fixation, the previously tagged capsular flaps are repaired over the graft to provide secondary stabilization and soft tissue coverage. The sternocleidomastoid and pectoralis fascia are meticulously closed to eliminate dead space, and the skin is closed in a layered fashion.
Complications, Incidence Rates, and Salvage Management
Surgical intervention at the sternoclavicular joint is fraught with potential complications, ranging from minor wound healing issues to catastrophic, life-threatening events. The surgeon must be acutely aware of these risks, counsel the patient appropriately, and possess the technical armamentarium to manage failures.
The most feared complication, historically associated with the now-condemned use of K-wires, is hardware migration into the mediastinum. Even with modern techniques utilizing suture anchors or tenodesis screws, hardware failure can occur. Suture anchors can pull out of the relatively osteopenic manubrium, leading to recurrent instability. Graft failure, either through traumatic rupture before incorporation or gradual attenuation, remains a significant risk, particularly in non-compliant patients who violate postoperative restrictions.
| Complication | Estimated Incidence | Etiology / Mechanism | Management Strategy |
|---|---|---|---|
| Hardware Migration | Historical (High with pins), Rare currently | Respiratory excursion, capillary action, gravity pulling unconstrained pins. | Prevention is absolute: Never use pins. Emergent cardiothoracic retrieval if it occurs. |
| Recurrent Instability | 5% - 15% | Graft attenuation, anchor pull-out, non-compliance with sling, missed secondary restraints. | Revision reconstruction with robust allograft; consider medial clavicle excision if low demand. |
| Infection (Deep) | 1% - 3% | Proximity to airway, extensive dissection, hematoma formation. | Urgent I&D, hardware/graft removal if infected, IV antibiotics, delayed reconstruction. |
| Neurovascular Injury | < 1% (Operative) | Drill plunge, retractor injury to innominate vessels, laceration of anterior jugular vein. | Intraoperative vascular repair, cardiothoracic assistance, meticulous subperiosteal dissection. |
| Thoracic Outlet Syndrome | 2% - 5% | Hypertrophic scarring, excessive inferior displacement of clavicle post-reconstruction. | First rib resection, scalenectomy, neurolysis (often requires specialized peripheral nerve surgeon). |
In cases of recalcitrant recurrent instability, deep infection necessitating graft removal, or severe post-traumatic osteoarthritis of the SC joint, salvage procedures must be considered. The primary salvage operation is an excision of the medial clavicle. However, this is not a simple resection. The excision must be meticulously planned to remove no more than 1.5 to 2.0 cm of the medial clavicle. Crucially, the insertion of the costoclavicular (rhomboid) ligament on the inferior aspect of the clavicle must be absolutely preserved. If the costoclavicular ligament is violated or resected during the excision, the remaining clavicle will become wildly unstable, migrating superiorly and causing severe pain and dysfunction. If the native costoclavicular ligament is incompetent, it must be reconstructed simultaneously with the medial clavicle excision to tether the remaining clavicle to the first rib.
Phased Post-Operative Rehabilitation Protocols
The success of a complex sternoclavicular joint reconstruction relies just as heavily on strict adherence to a phased postoperative rehabilitation protocol as it does on meticulous surgical technique. The biological graft requires significant time to incorporate into the osseous tunnels and achieve tensile strength sufficient to withstand the massive forces generated by the shoulder girdle.
Phase I: Maximum Protection (Weeks 0-6)
Immediately postoperatively, the patient is placed in a well-fitting, rigid
