Operative Management of Sternoclavicular Joint Instability
Key Takeaway
The sternoclavicular joint is a complex articulation where dislocations, though rare, present significant clinical challenges. While anterior dislocations are typically managed conservatively, posterior dislocations and severe, symptomatic recurrent instability may necessitate surgical intervention. This guide details the biomechanics, indications, and meticulous surgical techniques—including fascial loop stabilization and resection arthroplasty—required to safely navigate the vital neurovascular anatomy posterior to the joint.
Comprehensive Introduction and Patho-Epidemiology
The sternoclavicular joint (SCJ) represents the sole true synovial articulation linking the axial skeleton to the appendicular skeleton of the upper extremity. Because of its inherent osseous incongruity—functioning biomechanically as a diarthrodial saddle joint—its stability relies almost entirely on a robust, multifaceted ligamentous complex rather than bony containment. The medial clavicle articulates with the clavicular notch of the manubrium sterni and the superior aspect of the first rib cartilage. Due to the significant mismatch in articular surface areas, less than half of the medial clavicle actually articulates with the manubrium at any given time, making the joint intrinsically unstable from an osseous perspective.
Injuries to this joint are relatively uncommon, accounting for less than 3% of all shoulder girdle traumas and approximately 1% of all joint dislocations. The vast majority of recurrent dislocations of the sternoclavicular joint are anterior and, in most clinical scenarios, require only conservative treatment. Posterior dislocations, although exceedingly uncommon, are true orthopaedic and trauma emergencies. The perilous proximity of the mediastinal structures—including the great vessels, trachea, and esophagus—means that posterior displacement can lead to life-threatening compressive or lacerating injuries, dictating the need for urgent, and often closed, reduction in the acute setting, or open reduction if closed measures fail.
In the classic orthopaedic literature, Nettles and Lindscheid reported 60 patients with acute sternoclavicular joint dislocations, 57 of which were anterior, highlighting the sheer rarity of posterior variants. Similarly, in Rockwood’s extensive and seminal series of 273 dislocations, 221 were anterior. The mechanism of injury typically involves indirect forces applied to the shoulder girdle. An anterolateral force applied to the shoulder compresses the clavicle medially and posteriorly, often resulting in a posterior dislocation, whereas a posterolateral force drives the medial clavicle anteriorly.
Recurrent atraumatic anterior subluxation of the sternoclavicular joint, typically occurring with shoulder abduction and extension, is most frequently observed in young females. Often, it is associated with generalized ligamentous laxity (e.g., benign hypermobility syndrome, Ehlers-Danlos syndrome) and, according to Rockwood, is generally a self-limiting condition. Most patients with recurrent anterior SCJ dislocation should be treated non-operatively with a generalized upper extremity strengthening program, focusing intensely on periscapular stabilization, posture correction, and the strict avoidance of activities that place undue stress on the joint. Surgery for atraumatic anterior instability is recommended only if severe symptoms completely and irrevocably limit the activities of daily living, as surgical interventions in this region are fraught with severe, potentially catastrophic complications.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of the regional anatomy is non-negotiable when operating on the sternoclavicular joint. The medial end of the clavicle lies directly anterior to several vital structures, separated only by a thin layer of strap muscles (sternohyoid and sternothyroid) and fascial planes. The proximity of these structures means that any posterior plunging of surgical instruments, drills, or errant hardware can result in immediate, life-threatening hemorrhage or visceral injury.
The vital structures immediately posterior to the SCJ include:
* Vascular: The brachiocephalic (innominate) veins, the superior vena cava, the aortic arch, and the internal jugular and subclavian arteries and veins. The left brachiocephalic vein is particularly vulnerable as it crosses the midline directly posterior to the manubrium.
* Neurological: The vagus nerve, the phrenic nerve, the recurrent laryngeal nerve, and the anterior roots of the brachial plexus.
* Visceral: The trachea, the esophagus, and the apical pleura of the lungs.
The primary stabilizers of the SCJ include the anterior and posterior sternoclavicular capsular ligaments, the interclavicular ligament, and the costoclavicular (rhomboid) ligament. Biomechanical studies have definitively shown that the posterior capsular ligament is the most critical structure, acting as the strongest restraint to both anterior and posterior translation of the medial clavicle. The interclavicular ligament provides superior stability, while the robust costoclavicular ligament—consisting of an anterior and posterior fasciculus—resists superior displacement and limits excessive elevation and rotation.
Furthermore, the joint contains an intra-articular fibrocartilaginous disc that divides the joint into two separate synovial cavities. This disc is firmly attached superiorly to the medial clavicle and inferiorly to the first costal cartilage. It acts as a crucial shock absorber, dramatically increasing joint congruity, and acts as a tether to prevent medial displacement of the clavicle over the manubrium during medial compressive loads. Understanding the kinematics of the SCJ is also vital; during full shoulder elevation, the medial clavicle rotates posteriorly up to 50 degrees, elevates roughly 35 degrees, and retracts 35 degrees. Any surgical reconstruction must account for these massive rotational and translational forces to prevent premature graft failure.
Exhaustive Indications and Contraindications
The decision-making process for operative intervention at the sternoclavicular joint requires a meticulous balance of patient symptomatology, functional deficit, and the inherent risks of mediastinal proximity. Operative management is rarely the first line of treatment, except in specific, high-acuity scenarios. The surgeon must carefully select patients who have failed exhaustive non-operative management or those who present with anatomic emergencies.
| Clinical Scenario | Operative Indication | Contraindication / Relative Contraindication |
|---|---|---|
| Acute Anterior Dislocation | Rarely indicated. Only if severely symptomatic irreducible soft-tissue interposition occurs. | Routine acute anterior dislocations (manage non-operatively). |
| Acute Posterior Dislocation | Irreducible by closed means, or presence of mediastinal compression (vascular/tracheal compromise). | Medically unstable patient (stabilize first). |
| Recurrent Traumatic Anterior Instability | Failure of >6 months of targeted physical therapy with severe limitation of ADLs. | Voluntary dislocators, atraumatic multidirectional instability. |
| Recurrent Posterior Instability | Symptomatic recurrent subluxation/dislocation causing pain or transient mediastinal symptoms. | Asymptomatic subluxations. |
| Chronic Degenerative Joint Disease with Instability | Intractable pain failing injections/therapy (Indication for Resection Arthroplasty). | Active local or systemic infection. |
| Hardware Fixation | NEVER INDICATED. Transarticular K-wires or pins are strictly forbidden. | ABSOLUTE CONTRAINDICATION: Use of smooth or threaded pins due to fatal migration risk. |
The indications for surgery must be explicitly documented, particularly distinguishing between traumatic and atraumatic etiologies. Traumatic unidirectional instability in a patient without generalized hyperlaxity responds reasonably well to soft-tissue reconstruction. Conversely, operating on a patient with voluntary instability or underlying connective tissue disorders (e.g., Ehlers-Danlos) is a relative, if not absolute, contraindication due to the exceptionally high rate of recurrent stretching of the reconstructed tissues and subsequent failure.
Furthermore, the presence of degenerative changes dictates the type of procedure. A joint-preserving stabilization (like a figure-of-eight graft) is indicated in a young patient with a healthy articular surface. However, if the joint is riddled with post-traumatic osteoarthritis, stabilizing a painful, arthritic joint will only lead to a stable, but persistently painful shoulder. In such cases, a resection arthroplasty (e.g., the Rockwood procedure) combined with stabilization of the medial stump is the procedure of choice.
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is the cornerstone of safe and effective sternoclavicular joint surgery. Standard orthogonal radiographs are notoriously difficult to interpret due to the overlapping shadows of the ribs, sternum, and vertebrae. Therefore, specialized views such as the "Serendipity view" (a 40-degree cephalic tilt view targeting the SCJ) are essential for initial screening. However, the gold standard for evaluating SCJ pathology is a fine-cut Computed Tomography (CT) scan with 3D reconstructions.
A CT scan not only confirms the direction of the dislocation but also assesses the presence of medial clavicular physeal fractures. The medial clavicular epiphysis is the last to ossify (around age 18) and the last to fuse (up to age 25). Many apparent SCJ dislocations in patients under 25 are actually Salter-Harris physeal fractures, which have a tremendous remodeling potential and often heal with conservative management. If vascular compromise or chronic posterior dislocation is suspected, a CT Angiogram (CTA) is mandatory to map the proximity of the great vessels and detect any pseudoaneurysms or vessel adherence to the clavicle.
Patient positioning and operating room setup require meticulous attention. The patient is placed in the supine position on a standard radiolucent operating table. A critical step is the placement of a bump—typically three or four folded towels or a sandbag—vertically between the scapulae. This allows the bilateral shoulder girdles to fall posteriorly, thereby opening the anterior joint space of the SCJ and reducing the medial clavicle anteriorly, which is especially helpful in posterior dislocations. The head is placed on a neutral foam donut, and the anesthesia team is instructed to avoid excessive neck extension.
Due to the catastrophic risk of vascular injury, it is strongly recommended that a cardiothoracic or vascular surgeon be notified and available on standby, particularly during revision cases or chronic posterior dislocations where scar tissue binds the clavicle to the brachiocephalic vein. The surgical field must be prepped and draped widely, exposing the entire sternum, bilateral clavicles, and the anterior chest down to the xiphoid process, allowing for the possibility of an emergent median sternotomy if massive hemorrhage occurs.
Step-by-Step Surgical Approach and Fixation Technique
Surgical intervention at the SCJ demands a masterful, unhurried technique. All dissection must remain strictly subperiosteal. The periosteal sleeve acts as a vital barrier between the surgical instruments and the mediastinum.
Principles of Capsular Shift and T-Plasty
When local capsular tissue is robust and sufficient—typically in acute or subacute traumatic anterior dislocations without severe tissue attenuation—direct repair or plication of the sternoclavicular joint capsule can be attempted. The principles of capsular tensioning are universal across orthopaedic joint reconstructions. For comparative academic reference, the classic T-plasty capsular shift illustrates the fundamental biomechanics of capsular tensioning that can be conceptually adapted when managing redundant SCJ capsules.
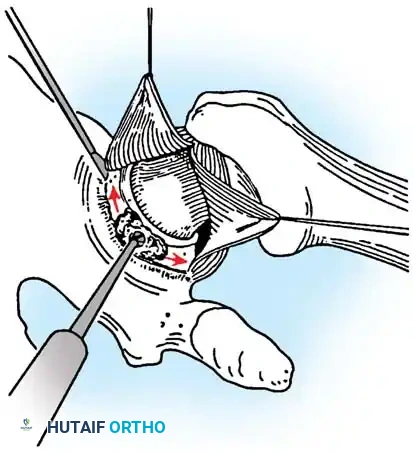
Fig. A: An incision is made in the capsule perpendicular to the joint rim to create a T-plasty. Superior and inferior capsular flaps are tagged with sutures.
The T-plasty begins with a meticulous exposure of the anterior capsule. An incision is made along the axis of the joint, followed by a perpendicular limb to create distinct superior and inferior capsular flaps. These flaps are tagged with heavy non-absorbable sutures. The joint is inspected, and any intra-articular loose bodies or degenerative disc fragments are debrided.
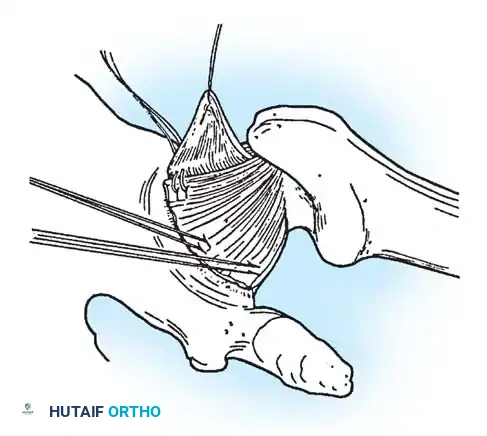
Fig. B: The inferior capsular flap is shifted superiorly; sutures attach it securely to the rim, eliminating inferior redundancy.
The inferior capsular flap is then aggressively shifted superiorly and medially, tensioning the inferior and anterior restraints. Sutures are passed through the robust periosteum of the manubrium or through small bone anchors placed safely in the anterior cortex of the sternum. This maneuver eliminates the inferior capsular redundancy that often contributes to multidirectional micro-instability.
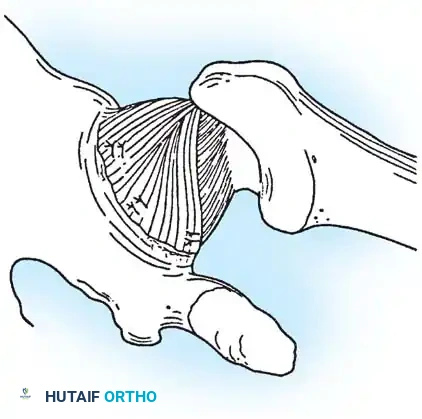
Fig. C: The superior flap is advanced inferiorly to create a robust, double-layer closure. (Adapted principles from Lieberman JR, et al: Recurrent dislocation of a hip with a labral lesion, J Bone Joint Surg 75A:1524, 1993.)
Finally, the superior flap is advanced inferiorly over the shifted inferior flap, creating a robust, double-layered "pants-over-vest" closure. This dramatically thickens the anterior restraint. However, if good capsular and ligamentous materials are unavailable or severely attenuated, local tissue reconstruction using autograft or allograft must be employed.
Speed Stabilization Using Fascial Loop (Technique 45-9)
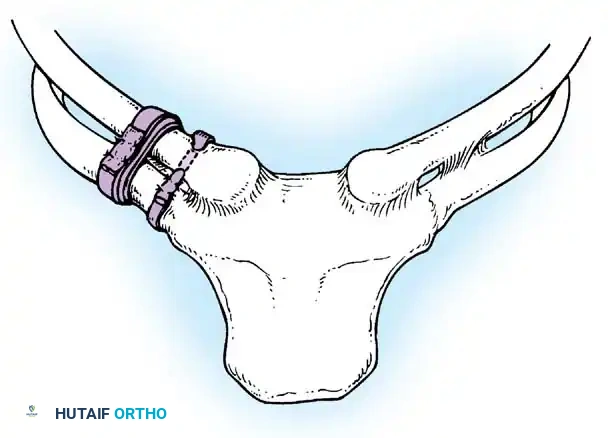
In 1928, Allen described a method of stabilizing the SCJ using a fascial loop passed through holes drilled in the medial clavicle and the second rib. The Speed technique is a refined, biomechanically superior modification of this operation, utilizing a fascial loop (such as palmaris longus, gracilis, fascia lata, or a semitendinosus allograft) passed around the clavicle and the first rib, effectively recreating the costoclavicular ligament.
Incision and Exposure: Beginning at a point 1.3 cm lateral to the midline of the sternum, an incision 6.5 cm long is made parallel to the inferior border of the medial third of the clavicle. The platysma is divided, and the medial third of the clavicle is completely freed of all soft tissues using meticulous subperiosteal dissection. Unless intra-articular pathology dictates otherwise, the sternoclavicular joint capsule should not be opened to preserve its remaining stabilizing function.
Rib Preparation and Graft Passage: The medial end of the first rib and its cartilage are exposed by detaching and retracting a portion of the pectoralis major muscle laterally and distally. Using a specialized rib stripper, about 5 cm of the first rib is carefully freed of soft tissue, keeping its cartilage intact. This dissection must be performed slowly and directly on the bone to protect the underlying apical pleura. A blunt-pointed aneurysm needle is passed deep to the first rib at the level of the costoclavicular ligament. A nonabsorbable suture attached to the graft (1.5 cm wide and 20 cm long) is threaded and drawn deep to the rib, and subsequently deep to the clavicle.
Fig. 45-20: Speed technique for the repair and stabilization of the sternoclavicular joint using a figure-of-eight fascial loop.
Figure-of-Eight and Osseous Fixation: The graft passage is repeated to form a double loop of fascia around the clavicle and the first rib in a figure-of-eight configuration. The ends are sutured together under tension while the clavicle is held in a reduced position. For enhanced stability against anteroposterior translation, a hole is drilled through the clavicle about 1.5 cm lateral to its medial end. A second strip of fascia is passed through this hole and sutured securely, providing rigid osseous fixation that augments the soft-tissue loops.
Resection Arthroplasty of the Sternoclavicular Joint (Rockwood Technique 45-10)
Rockwood established that if sufficient capsular material is unavailable, or if the joint is severely arthritic, resection of the medial 1 to 1.5 inches of the clavicle should be performed, followed by robust stabilization of the residual clavicle to the first rib to prevent it from migrating superiorly into the neck.
Positioning and Incision: With the patient supine and a bump between the scapulae, an 8- to 20-cm skin incision is made, beginning cephalad to the superior border of the medial aspect of the clavicle, extending to the notch of the manubrium, and continuing caudad onto the anterior surface of the manubrium.
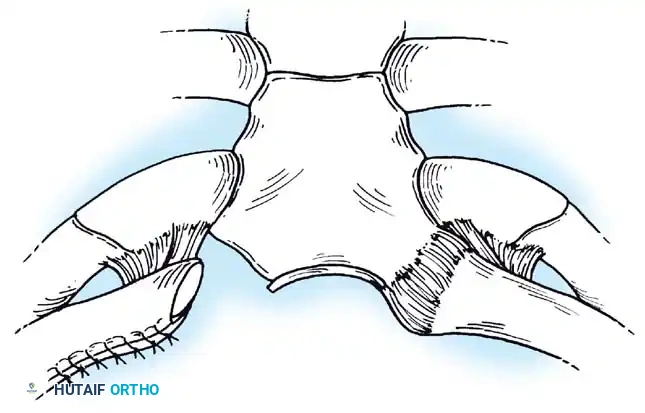
Fig. 45-21A: Skin incision made along the superior border of the medial aspect of the clavicle to the notch of the manubrium.
Deep Dissection and Periosteal Elevation: A deep incision is made along the medial 4 to 5 cm of the clavicle, crossing the capsular ligament.
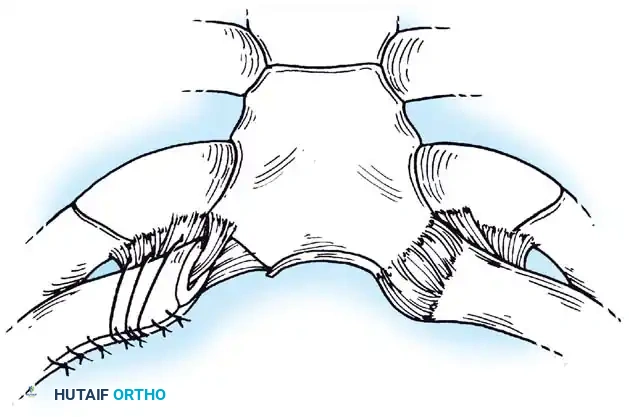
Fig. 45-21B: Deep incision made along the medial clavicle across the capsular ligament.
The periosteum is dissected carefully off the medial portion of the clavicle. It is critical to preserve this periosteal tube for later closure and to protect the underlying costoclavicular ligament. The sternal head of the sternocleidomastoid muscle is preserved, but the clavicular head is reflected free.
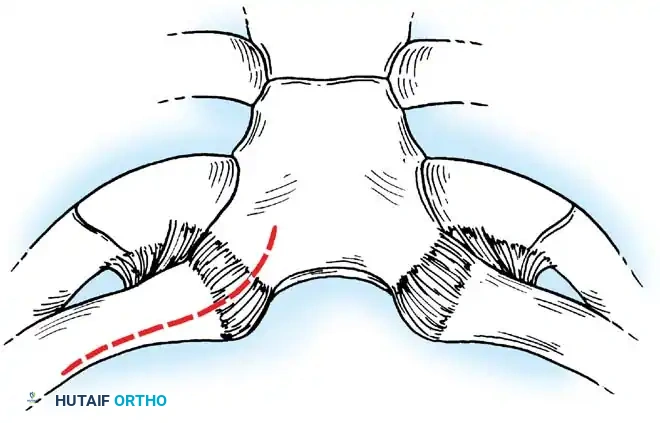
Fig. 45-21C: Periosteum dissected off the medial portion of the clavicle, preserving the periosteal tube.
Osteotomy Execution: A curved 1- or 2-cm wide retractor (such as a malleable or right-angle retractor) is passed posterior to the clavicle to isolate it and physically shield the posterior vascular structures. The osteotomy site is placed medial to the stabilizing costoclavicular ligament to allow resection of exactly 1.5 cm of the medial clavicle. Drill holes are placed through both cortices to prevent splintering, and the osteotomy is completed using an air-powered drill with a side-cutting bit.
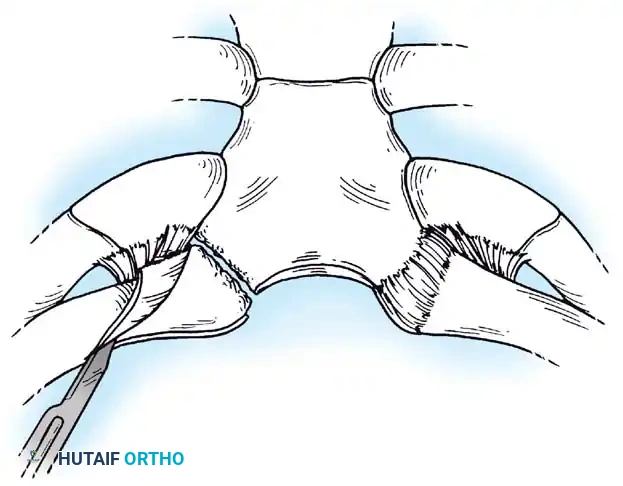
Fig. 45-21D: Drill holes made through both cortices. An air-powered side-cutting drill completes the osteotomy.
Stabilization with Intact Costoclavicular Ligament: If the sternal attachment of the intra-articular disc ligament is intact, a nonabsorbable No. 1 cotton Dacron suture is woven through the ligament. The medullary canal of the medial clavicle is drilled and curetted. Two small holes are drilled into the superior cortex, 1 cm lateral to the resection. The free ends of the suture are passed into the canal and out the superior holes, then tied tightly while holding the clavicle in a reduced position.
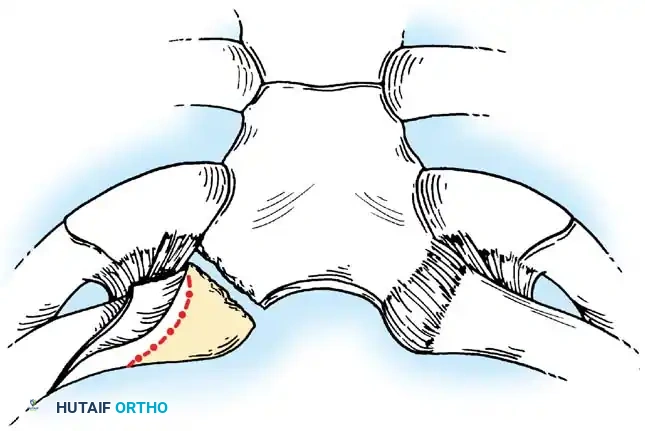
Fig. 45-21E: Closure of the periosteal tube secures the stabilized medial end of the clavicle when the costoclavicular ligament is intact.
Stabilization with Absent Costoclavicular Ligament: If the costoclavicular ligament is absent, continuity between the clavicle and first rib must be reestablished. Heavy nonabsorbable sutures (or allograft tape) are passed around the remaining medial end of the clavicle, through its periosteal tube, and through the residual scar of the old ligament on the first rib. The sutures are tied securely, ensuring the clavicle is not compressed directly onto the rib, which would cause severe mechanical pain.
Fig. 45-21F: Closure when the costoclavicular ligament is absent. Sutures are passed through the stump of the old ligament or around the first rib for stability.
Complications, Incidence Rates, and Salvage Management
Surgical interventions at the sternoclavicular joint carry a unique and highly morbid complication profile compared to other orthopaedic procedures. The proximity of the mediastinum leaves zero margin for error. Complications can be broadly categorized into intraoperative neurovascular injuries, postoperative mechanical failures, and chronic soft-tissue issues.
| Complication | Estimated Incidence | Etiology / Pathomechanism | Salvage / Management Strategy |
|---|---|---|---|
| Vascular Laceration | < 1% (but highly lethal) | Plunging drills/saws, over-penetration of retractors into the brachiocephalic vein or SVC. | Immediate packing, emergent median sternotomy by cardiothoracic surgery, primary vascular repair. |
| Pneumothorax | 1 - 3% | Errant dissection around the first rib damaging the apical pleura. | Intraoperative detection requires a chest tube (thoracostomy); postoperative requires serial CXR and potential tube placement. |
| Recurrent Instability | 10 - 20% | Graft stretching, failure of fixation, non-compliance with postoperative restrictions. | Revision using robust allograft (e.g., semitendinosus figure-of-eight) or conversion to resection arthroplasty. |
| Hardware Migration | Historical (High) | Use of K-wires or Steinmann pins migrating into the heart, aorta, or pulmonary artery. | Absolute prevention: Never use transarticular pins. If historical pins are found, urgent cardiothoracic removal is required. |
| Hypertrophic Scarring | 15 - 25% | Tension across the anterior chest wall skin during healing. | Intralesional corticosteroid injections, silicone sheeting, plastic surgery revision if severe. |
The most historically infamous complication of SCJ surgery is the migration of smooth or threaded transarticular pins. Literature is replete with case reports of K-wires migrating into the right ventricle, ascending aorta, and pulmonary vasculature, often resulting in fatal cardiac tamponade or exsanguination. Consequently, the use of any unconstrained metallic pins across the SCJ is universally condemned and considered a gross deviation from the standard of care.
Salvage management for a failed soft-tissue reconstruction typically involves a thorough reassessment of the patient's bone quality and ligamentous laxity. If a primary figure-of-eight graft fails, a revision reconstruction utilizing a thicker allograft (such as an Achilles tendon or robust semitendinosus graft) anchored with modern biocomposite tenodesis screws in the clavicle and sternum can be attempted. If the joint is unsalvageable or persistently painful, converting to a Rockwood medial clavicle resection arthroplasty is the definitive salvage procedure, provided the clavicle is securely tethered to the first rib to prevent superior migration and impingement on the neurovascular bundle of the neck.
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following sternoclavicular joint reconstruction or resection arthroplasty is a delicate balance between protecting the healing soft tissues and preventing adhesive capsulitis of the glenohumeral joint. Because the SCJ undergoes significant rotation and translation during arm elevation, early aggressive motion will inevitably stretch and fail the graft or repair.
Phase I: Maximal Protection (Weeks 0 to 6)
Immediately postoperatively, the upper extremity is strictly immobilized in a Velpeau dressing or a well-fitted sling-and-swathe. For the first 3 to 4 weeks, motion is limited exclusively to the elbow, wrist, and hand. On the second postoperative day, the patient may be allowed to perform gentle, gravity-assisted pendulum exercises, but they are strictly cautioned against any active flexion or abduction of the shoulder. Elevation above 90 degrees places immense rotational torque on the medial clavicle and will compromise the repair.
Phase II: Controlled Motion (Weeks 6 to 12)
At 6 weeks, the sling is gradually weaned. A phased physical therapy program is initiated, transitioning from passive range of motion (ROM) to active-assisted exercises. Pulley exercises and supine forward elevation are introduced. The patient must continue to avoid pushing, pulling, and heavy lifting. Scapular stabilization exercises (e.g., isometric retractions) are crucial during this phase to ensure that the periscapular musculature absorbs the kinetic chain forces rather than the healing SCJ.
Phase III: Strengthening and Return to Function (Weeks 12+)
Strengthening exercises utilizing resistance bands and light weights are initiated at 8 to 12 weeks, provided full, pain-free ROM has been achieved. Return to heavy manual labor, overhead sports, or contact sports is generally prohibited for a minimum of 4 to 6 months. In patients who have undergone a Rockwood resection arthroplasty, permanent restrictions on maximal overhead lifting may be advised to prevent chronic pain at the pseudarthrosis site between the clavicle and the first rib.
Summary of Landmark Literature and Clinical Guidelines
The evolution of operative management for SCJ instability is deeply rooted in a few landmark studies that have shaped modern orthopaedic consensus. The initial descriptions by Allen in 1928 and subsequent modifications by Speed laid the groundwork for soft-tissue reconstruction, emphasizing the necessity of utilizing robust fascial grafts rather than relying on attenuated local tissue.
Rockwood’s monumental contributions to shoulder literature cannot be overstated. His series of 273 SCJ dislocations definitively mapped the epidemiology and natural history of the disease. Rockwood and Wirth demonstrated that atraumatic anterior instability is almost universally benign and self-limiting, establishing the modern clinical guideline that surgical intervention should be aggressively avoided in this cohort. Furthermore, Rockwood's development of the resection arthroplasty technique provided a reliable, standardized salvage option for the arthritic or irreparably unstable joint, shifting the focus from attempting to force an anatomic reduction of a destroyed joint to creating a stable, pain-free pseudarthrosis.
Current clinical guidelines from the American Academy of Orthopaedic Surgeons (AAOS) and the American Orthopaedic Society for Sports Medicine (AOSSM) strongly echo these historical lessons. The consensus mandates exhaustive non-operative management for anterior instability, urgent closed or open reduction for acute posterior dislocations, the absolute prohibition of transarticular pin fixation, and the necessity of advanced cross-sectional imaging (CT/CTA) for operative planning. Adherence to these principles ensures that the orthopaedic surgeon navigates the treacherous anatomy of the sternoclavicular joint with maximum safety and optimal functional outcomes.
This academic synthesis is based on established protocols from Hutaifortho's Operative Orthopaedics and has been medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is designed to assist orthopedic residents, fellows, and practicing surgeons in surgical preparation and board reviews (AAOS, FRCS, Arab Board).

Chapter Index
- Comprehensive Introduction and Patho-Epidemiology
- Detailed Surgical Anatomy and Biomechanics
- Exhaustive Indications and Contraindications
- Pre-Operative Planning, Templating, and Patient Positioning
- Step-by-Step Surgical Approach and Fixation Technique
- Complications, Incidence Rates, and Salvage Management
- Phased Post-Operative Rehabilitation Protocols
- Summary of Landmark Literature and Clinical Guidelines
Back to Master Guide