Solve Orthopedic Cases: Extensor Carpi Radialis Brevis & Elbow Pain
Key Takeaway
This topic focuses on Solve Orthopedic Cases: Extensor Carpi Radialis Brevis & Elbow Pain, Valgus extension overload (VEO) in athletes, like baseball pitchers, presents as posteromedial elbow pain exacerbated by throwing. It involves chronic stress, leading to chondrolysis and osteophyte formation, with cubital tunnel syndrome being a common neurologic complication. While distinct, issues affecting the extensor carpi radialis brevis, such as lateral epicondylitis, also cause activity-related elbow discomfort.
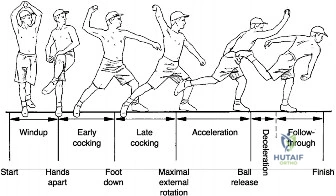
You are presented with a 16-year-old competitive baseball pitcher complaining of posteromedial elbow pain. He describes the pain as worsening during the deceleration phase of throwing. He has failed 6 months of conservative management. How do you approach the physical examination to distinguish between primary UCL insufficiency and Valgus Extension Overload (VEO)?

Candidate: I would examine the elbow for tenderness at the medial epicondyle and the sublime tubercle. I would perform a valgus stress test at 30 degrees to check for UCL laxity. I would also check range of motion, specifically looking for a loss of terminal extension, and perform an O'Driscoll's moving valgus stress test. If the pain is in the posterior compartment, it is likely VEO.
Failing to emphasize the *provocation* of pain. Simply listing tests is insufficient. Candidates often miss the significance of "forced terminal extension" as the defining maneuver for VEO and fail to explain *why* the 30-degree valgus stress test is performed (to unlock the olecranon from the fossa).
I would perform a systematic assessment focusing on the triad of medial tension, lateral compression, and posterior shear. 1. Medial stability: Valgus stress test at 30 degrees (to clear the olecranon from the fossa) and the Moving Valgus Stress Test to specifically challenge the anterior bundle of the UCL. 2. Posterior impingement: Forced terminal extension—if this reproduces the sharp posteromedial pain, it is highly suggestive of VEO. 3. Neurological: Assess ulnar nerve stability (subluxation) and Tinel's, as ulnar neuritis frequently co-exists with medial/posterior pathology. 4. Differential: Check resisted wrist flexion/pronation to rule out medial epicondylitis.
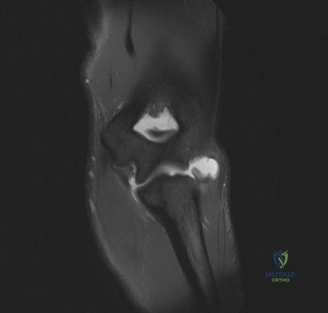
The imaging confirms a hypertrophic posteromedial olecranon osteophyte. You are planning arthroscopic debridement. What is the specific "danger zone" you must avoid during resection, and what is the clinical consequence of over-resecting this bone?
Candidate: The danger zone is the medial cortex of the olecranon. If I resect too much of this, the patient will become unstable. This is because the medial olecranon acts as a bony stabilizer against valgus stress, and if it's gone, the UCL takes all the load, potentially leading to failure of the ligament.
Providing a vague answer without citing the biomechanical role of the olecranon as a "secondary stabilizer." Candidates often fail to mention the direct link between over-resection and the requirement for subsequent "Tommy John" (UCL reconstruction) surgery.
The danger zone is the medial cortex of the olecranon. The olecranon serves as a critical secondary bony stabilizer to valgus stress. Excessive resection—specifically beyond 2-3mm—violates this structural support, shifting the entire valgus load onto the anterior bundle of the UCL. This inevitably leads to iatrogenic valgus instability, which is a catastrophic complication often mandating secondary ligamentous reconstruction.
During your arthroscopic evaluation, you note that after removing the osteophyte, the joint remains somewhat "loose" to valgus stress. How do you manage this intraoperatively, and what is the rationale for your decision?

Candidate: If it's loose, I should perform a stress test under fluoroscopy. If there's significant opening, I may need to consider a UCL reconstruction or repair. I would explain to the patient that the osteophyte was just a symptom of the underlying ligamentous instability.
Not having a threshold. A "little bit of looseness" is often physiological. Failing to mention dynamic assessment (comparison to the contralateral side) or the fact that isolated debridement is usually the primary step, with reconstruction reserved for proven high-grade insufficiency.
First, I would perform a dynamic arthroscopic valgus stress test, ideally with fluoroscopic confirmation, comparing the opening to the contralateral, non-throwing elbow. 1. If the opening is >1-2mm compared to the contralateral side, the UCL is likely insufficient. 2. I would then counsel that simply removing the osteophyte will likely fail to return the athlete to high-level throwing. 3. Depending on the patient's goals and the state of the ligament, I would proceed with a concomitant UCL reconstruction or, at minimum, document the findings extensively to discuss a staged approach versus immediate reconstruction with the patient/family.
