

A 29-year-old competitive weight-lifter presents with acute anterior shoulder pain and loss of power following a bench press injury. He reports an audible 'pop'. On inspection, you note a loss of the anterior axillary fold and ecchymosis extending down the medial arm. How would you structure your clinical assessment to confirm your diagnosis and rule out pitfalls?

Candidate: I would perform a focused shoulder examination. I’d look for the loss of the anterior axillary fold and medial muscle retraction. I would test resisted adduction at different angles of abduction to differentiate the clavicular and sternocostal heads. I would specifically palpate the axilla to check for the tendon. I'd also rule out rotator cuff and biceps pathology using clinical tests.
The candidate fails to address the "pseudo-tendon" pitfall. Many candidates skip the physical act of deep palpation to distinguish the intact superficial fascia from the avulsed tendon, leading to a missed diagnosis of a complete tear.
A structured response is essential: 1. Inspection: Note the loss of axillary fold and the "hollow" in the deltopectoral groove. 2. Palpation: Crucially, mention the "Intact Fascia" Illusion—the superficial fascia may feel cord-like; I would palpate deep to this for the actual tendon footprint. 3. Functional Testing: Resisted adduction at 90° for the sternocostal head and adduction at 0° for the clavicular head. 4. Differential Exclusion: Systematically perform Hawkins-Kennedy (impingement), Lift-off/Belly-press (subscapularis), and Speed’s test (long head of biceps) to rule out concurrent intra-articular pathology.
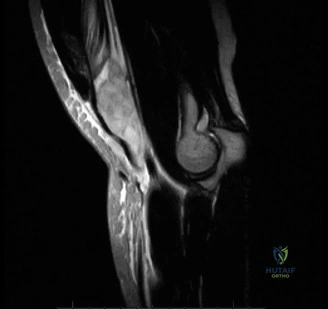
The MRI confirms a complete avulsion of the sternocostal head. You are planning surgery for this 29-year-old. What are the key considerations for your surgical approach and fixation strategy?
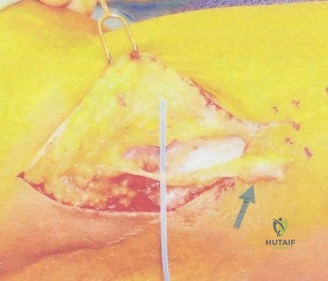
Candidate: I would perform a deltopectoral approach. I’d identify the retracted tendon, mobilize it carefully to avoid injury to the pectoral nerves, and perform a re-attachment to the humerus using suture anchors or buttons. I would ensure the bone bed is decorticated.
The candidate ignores the bilaminar anatomy of the insertion. Failing to mention the specific anatomical footprint (lateral lip of the bicipital groove) and the specific technique to avoid nerve injury (medial/lateral pectoral nerve protection) is a major weakness.
I would approach via the deltopectoral interval, mobilizing the tendon while protecting the medial and lateral pectoral nerves—especially the medial pectoral nerve which pierces the pectoralis minor. I would use Krackow or Mason-Allen locking stitches on the tendon. For fixation, I would advocate for cortical button fixation on the lateral lip of the bicipital groove, as biomechanical studies show superior load-to-failure compared to anchors. The footprint must be decorticated to bleeding bone to ensure biological healing. I would emphasize re-creating the native footprint to restore the length-tension relationship.
The patient asks about his return to weight-lifting. What advice do you give regarding the rehabilitation timeline and long-term risk management?
Candidate: I would tell him it takes about 6 months to get back to the gym. I'd advise him to start with light weights and gradually work his way up, avoiding heavy bench presses initially.
The candidate is too vague. They fail to mention the specific risk of re-rupture due to eccentric loading and provide no technical advice on how the patient should modify his technique (e.g., grip width, depth of press) to avoid future injury.
The return to sport must be strictly phased: 1. Phase 1-2 (0-12 weeks): Focus on protective immobilization and passive, then active-assisted ROM. No heavy lifting. 2. Phase 3 (3-6 months): Isotonic strengthening; avoid eccentric loading. 3. Return to lifting (6 months+): I would insist on specific biomechanical modifications: narrowing the grip width to reduce the lever arm and utilizing a "floor press" or "board press" to limit the humerus from extending past the torso, thereby protecting the repair from the high-torque, end-range eccentric position that caused the primary injury.
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding shoulder-and-elbow-cases-4