Right Shoulder Pain? Avoid This Common X-ray Mistake.

Key Takeaway
Your ultimate guide to Right Shoulder Pain? Avoid This Common X-ray Mistake. starts here. For acute right shoulder pain following a fall with limited range of motion, and an initial AP X-ray, the next most appropriate step is to obtain an axillary view x-ray. A single AP view is insufficient to conclusively rule out a fracture or a shoulder dislocation, which an axillary view helps to diagnose, guiding proper management.
A 33-year-old male presents to the ED after a traumatic sports injury to the shoulder. You are presented with the following radiograph. What is your immediate interpretation, and what crucial error in diagnostic evaluation must you avoid here?
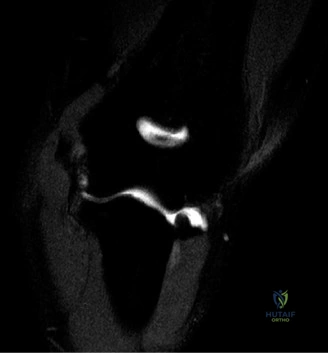
Candidate: The AP view shows a potential "lightbulb sign" suggestive of a posterior glenohumeral dislocation. My primary error would be relying solely on this single projection. I would immediately order an axillary lateral or Velpeau view to confirm concentricity.
Failing to mention the axillary view, or worse, suggesting an MRI before confirming the reduction status of the joint. Candidates often forget that the "lightbulb sign" is a classic marker of internal rotation and posterior displacement, but it is not diagnostic without an orthogonal view.
The candidate must state: "One view is no view." I would state that the AP view is suggestive of posterior dislocation due to the internal rotation/lightbulb appearance. I would mandate a true axillary lateral (or modified Velpeau view) to definitively assess glenohumeral concentricity. Furthermore, I would emphasize that failure to get this orthogonal view is the most common cause of a missed posterior dislocation, which can lead to rapid secondary articular damage.
We see a high prevalence of anterior instability in young, athletic patients. What is the most critical prognostic variable regarding the risk of recurrence, and how does the patient's age influence your surgical decision-making?

Candidate: Age is the most critical variable. Patients under 20 have up to a 90% recurrence risk non-operatively. As age increases, recurrence risk drops. In young active patients, I would advocate for early surgical stabilization to prevent cumulative bone loss.
Failing to mention the "unhappy triad" for older patients (>40), where the risk of recurrence is low but the risk of a concomitant rotator cuff tear is significantly higher. Candidates often focus only on the young cohort and ignore the different risk profile in the elderly.
Structure the answer by age: <20 years (~90% recurrence), 20-40 years (~60% recurrence), and >40 years (~10% recurrence). Highlight that in the young, failure is usually due to capsulolabral avulsion, while in the elderly, we must screen for rotator cuff pathology. Emphasize that in the young athlete, we aim to prevent the "bipolar bone loss" cycle that leads to early-onset osteoarthritis (dislocation arthropathy).
When assessing a patient for a potential Latarjet procedure, what is the role of the "engaging Hill-Sachs" lesion, and how is the "glenoid track" used to make that determination?
Candidate: The glenoid track is calculated as 83% of the glenoid width minus any bone loss. If the Hill-Sachs lesion extends medially past this track, it is "off-track" and will engage the glenoid. This is a strong indication for a Latarjet procedure or Remplissage.
Simply stating "it engages" without defining the glenoid track. Examiners expect the candidate to know the specific percentage (83%) and the mechanism of interaction (Hill-Sachs medial to the track on the anterior rim).
Define the "glenoid track" as the contact zone between the humeral head and glenoid during ABER. Explain that if the Hill-Sachs lesion's medial margin exceeds the glenoid track, it is "off-track." This indicates that simple soft-tissue stabilization will fail, necessitating bony augmentation (like a Latarjet) to increase the effective glenoid surface area or a Remplissage to mechanically fill the humeral defect.
