Advanced MRI Evaluation and Surgical Management of Upper Extremity Pathologies

Key Takeaway
Magnetic resonance imaging (MRI) is an indispensable modality for evaluating complex upper extremity pathologies. High-resolution imaging utilizing dedicated surface coils allows precise assessment of the triangular fibrocartilage complex, carpal ligaments, and glenoid labrum. This guide details the indications, biomechanical considerations, and surgical management protocols for wrist, elbow, and shoulder lesions identified via advanced MRI techniques.
Comprehensive Introduction and Patho-Epidemiology
The integration of high-resolution Magnetic Resonance Imaging (MRI) into the diagnostic algorithm of upper extremity orthopedics has fundamentally revolutionized the precision with which surgeons can conceptualize, classify, and ultimately manage complex articular and periarticular pathologies. Historically, the evaluation of the shoulder, wrist, and elbow relied heavily on clinical acumen, plain radiography, and invasive diagnostic arthroscopy. Today, the advent of high-field MRI systems—specifically 1.5 Tesla and 3.0 Tesla units—coupled with dedicated phased-array extremity surface coils, allows for an unprecedented visualization of the capsulolabral complex, intrinsic carpal ligaments, and delicate collateral ligamentous structures. This non-invasive modality has become the undisputed gold standard, bridging the gap between ambiguous clinical presentations and definitive surgical planning.
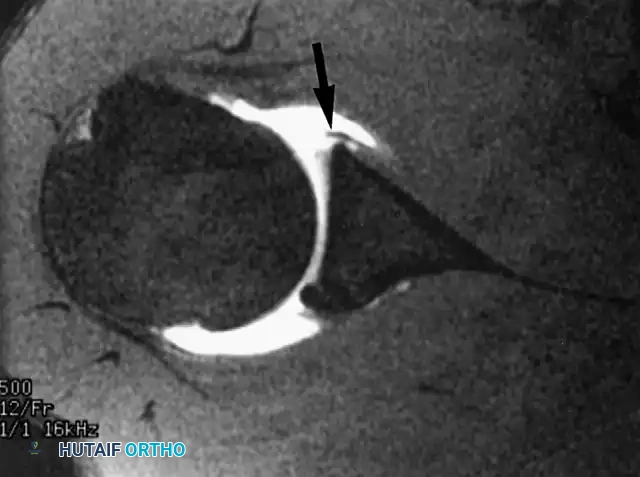
The patho-epidemiology of upper extremity injuries is intimately tied to the unique biomechanical demands placed upon these joints, particularly in athletic and high-demand occupational populations. In the shoulder, the glenohumeral joint trades inherent osseous stability for a global range of motion, rendering it highly susceptible to anterior, posterior, and multidirectional instability. Traumatic anterior dislocations frequently result in the classic Bankart lesion—an avulsion of the anteroinferior labrum and attached inferior glenohumeral ligament (IGHL) complex from the glenoid rim. Epidemiological data suggests that the recurrence rate of anterior instability in young contact athletes (under the age of 20) managed non-operatively approaches 80% to 90%. Furthermore, the "one-way valve" phenomenon associated with superior labral anterior-posterior (SLAP) or posterior labral tears can lead to the insidious development of paralabral cysts, extending into the spinoglenoid or suprascapular notch and causing devastating compressive neuropathies.
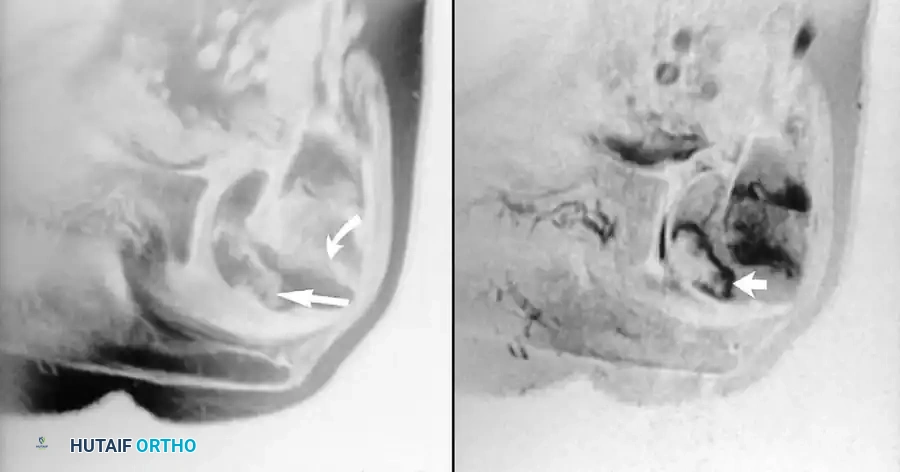
Moving distally, the wrist and elbow present their own distinct epidemiological profiles. Ulnar-sided wrist pain is frequently dubbed the "low back pain of the upper extremity" due to its diagnostic complexity. The triangular fibrocartilage complex (TFCC), the primary stabilizer of the distal radioulnar joint (DRUJ), is highly vulnerable to both traumatic axial loading with hyper-rotation and degenerative attrition. Palmer Class 1 traumatic tears are predominantly seen in young athletes and laborers, whereas Palmer Class 2 degenerative tears correlate strongly with positive ulnar variance and advancing age. In the elbow, the ulnar collateral ligament (UCL) is the focal point of pathology for overhead throwing athletes. The repetitive, extreme valgus stress experienced during the late cocking and early acceleration phases of the pitching motion leads to microtraumatic attenuation, partial undersurface tearing, and eventual catastrophic rupture of the anterior bundle of the UCL, necessitating reconstruction to restore athletic function.
Ultimately, the successful management of these upper extremity pathologies requires a symbiotic relationship between advanced musculoskeletal imaging and meticulous surgical execution. The orthopedic surgeon must not merely read the radiologist's report but must actively interrogate the MRI sequences—correlating signal alterations, capsular redundancies, and subchondral changes with the patient's specific mechanical symptoms. Every MRI examination must be meticulously directed at solving a specific clinical problem, ensuring that the subsequent surgical intervention is both targeted and biologically sound.
Detailed Surgical Anatomy and Biomechanics
The Glenohumeral Joint and Capsulolabral Complex
The glenohumeral joint is a highly sophisticated, unconstrained diarthrodial joint that relies on a complex interplay of static and dynamic stabilizers. The osseous anatomy consists of the shallow glenoid fossa and the large humeral head, a mismatch often compared to a golf ball on a tee. The glenoid labrum, a wedge-shaped ring of fibrous tissue and fibrocartilage, serves as the critical static stabilizer. It deepens the glenoid concavity by approximately 50%, effectively increasing the articular surface area and providing a robust anchor point for the glenohumeral ligaments (superior, middle, and inferior) and the long head of the biceps tendon. The inferior glenohumeral ligament (IGHL) complex, consisting of an anterior band, a posterior band, and an interposed axillary pouch, is the primary restraint to anterior, posterior, and inferior translation of the humeral head when the arm is abducted to 90 degrees.
In the context of paralabral cysts, an intimate understanding of the posterior scapular anatomy is paramount. The suprascapular nerve originates from the upper trunk of the brachial plexus (C5, C6) and courses through the suprascapular notch (beneath the transverse scapular ligament) to innervate the supraspinatus muscle. It then descends through the spinoglenoid notch—a narrow fibro-osseous tunnel bounded by the base of the scapular spine and the posterior glenoid neck—to innervate the infraspinatus. Ganglion cysts originating from posterior labral tears frequently decompress into this notch. Because the nerve is tethered at this location, even a small cyst can exert significant mass effect, resulting in selective denervation of the infraspinatus, characterized clinically by isolated external rotation weakness and profound muscle atrophy.

The Wrist, TFCC, and Carpal Kinematics
The wrist is an intricate biomechanical marvel comprising the radiocarpal, midcarpal, and distal radioulnar joints. The triangular fibrocartilage complex (TFCC) is a heterogeneous structure located at the ulnar aspect of the wrist. It consists of the central articular disc, the volar and dorsal radioulnar ligaments, the meniscus homologue, the ulnar collateral ligament, and the extensor carpi ulnaris (ECU) subsheath. Biomechanically, the TFCC acts as a critical shock absorber, transmitting approximately 20% of the axial load from the carpus to the distal ulna. More importantly, the deep fibers of the volar and dorsal radioulnar ligaments (the ligamentum subcruentum) attach to the fovea at the base of the ulnar styloid, serving as the primary restraint to dorsal and volar translation of the radius around the fixed ulna, thus stabilizing the DRUJ.
The intrinsic carpal ligaments, specifically the scapholunate (SL) and lunatotriquetral (LT) ligaments, are vital for maintaining synchronous carpal kinematics. The SL ligament is C-shaped, with its dorsal band being the thickest and most biomechanically significant restraint to scaphoid flexion and lunate extension. Disruption of the SL ligament leads to dorsal intercalated segment instability (DISI), progressing inevitably to scapholunate advanced collapse (SLAC) arthritis if left untreated. Conversely, the LT ligament relies on its stout volar band for stability; its disruption results in volar intercalated segment instability (VISI). High-resolution 3.0T MRI, particularly with dedicated wrist coils, is essential for identifying partial or complete tears of these delicate intrinsic structures prior to the onset of catastrophic carpal collapse.
The Elbow and Ulnar Collateral Ligament Complex
The elbow is a highly constrained hinge joint, with stability conferred by the congruity of the ulnohumeral articulation and the collateral ligament complexes. The ulnar collateral ligament (UCL) is the primary static restraint to valgus stress. It is composed of three distinct bundles: the anterior, posterior, and transverse bundles. The anterior bundle is the most biomechanically critical, originating from the anteroinferior surface of the medial epicondyle and inserting onto the sublime tubercle of the proximal ulna. It is taut throughout the entire arc of flexion and extension, bearing the brunt of the extreme valgus loads generated during the throwing motion.
During the late cocking and early acceleration phases of pitching, the elbow experiences valgus torques that can exceed the ultimate tensile strength of the native UCL. This repetitive microtrauma leads to attritional changes, often manifesting as partial undersurface tears at the sublime tubercle footprint. Over time, this valgus instability can lead to secondary pathologies, including radiocapitellar chondral overload, posteromedial impingement (valgus extension overload syndrome), and ulnar neuritis due to traction on the ulnar nerve within the cubital tunnel. Accurate MRI evaluation, particularly utilizing MR arthrography, is crucial for identifying these subtle undersurface tears and differentiating them from mere ligamentous edema or physiological laxity.
Exhaustive Indications and Contraindications
The decision to proceed with surgical intervention in the upper extremity must be predicated on a meticulous correlation between the patient's subjective complaints, objective physical examination findings, and advanced MRI pathology. Surgery is rarely indicated based on imaging alone, as asymptomatic labral variants, degenerative TFCC fraying, and mild UCL edema are frequently encountered in the general and athletic populations.
For shoulder instability, surgical stabilization is strongly indicated in young, active individuals following a first-time traumatic anterior dislocation, given the unacceptably high rate of recurrence with non-operative management. It is definitively indicated for recurrent instability, persistent apprehension, or mechanical symptoms (catching, locking) that have failed a comprehensive 3- to 6-month course of physical therapy focusing on periscapular and rotator cuff strengthening. In the presence of a spinoglenoid notch cyst causing suprascapular neuropathy, early arthroscopic decompression and labral repair are indicated to prevent irreversible fatty infiltration and atrophy of the infraspinatus muscle.
In the wrist, surgical repair of the TFCC is indicated for Palmer Class 1B (ulnar avulsion) or 1D (radial avulsion) tears that remain highly symptomatic despite splinting, NSAIDs, and targeted corticosteroid injections, particularly when associated with demonstrable DRUJ instability. Central perforations (Class 1A) are avascular and do not heal; therefore, they are indicated for arthroscopic debridement rather than repair. For the elbow, UCL reconstruction is indicated in high-level throwing athletes who have symptomatic valgus instability, MRI-confirmed full-thickness or high-grade partial tears, and who have failed a minimum of 3 months of rest and structured rehabilitation.
| Pathology / Procedure | Primary Surgical Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Anterior Shoulder Instability (Bankart Repair) | Recurrent traumatic instability; Failed 3-6 months PT; First-time dislocation in high-risk young athlete. | Active joint infection; Voluntary multidirectional instability with underlying psychiatric component. | Significant glenoid bone loss (>20-25%) requiring Latarjet; Severe capsular deficiency; Uncontrolled seizure disorder. |
| Paralabral Cyst Decompression | MRI-confirmed cyst with clinical suprascapular nerve entrapment (EMG/NCS confirmed or visible atrophy). | Asymptomatic incidental cyst without associated labral tear or nerve compression. | Severe, irreversible fatty infiltration of the infraspinatus (Goutallier Grade 3-4) where motor recovery is unlikely. |
| TFCC Repair (Palmer 1B/1D) | Symptomatic peripheral tear failing conservative care; Concomitant DRUJ instability. | Palmer Class 1A (central) tears (require debridement, not repair); Advanced ulnocarpal arthritis. | Positive ulnar variance >2mm (may require concomitant ulnar shortening osteotomy to unload the repair). |
| UCL Reconstruction (Tommy John) | Symptomatic valgus instability in a throwing athlete; MRI-confirmed tear; Failed conservative tx. | Non-athletes or low-demand patients who can function without overhead throwing; Active infection. | Concomitant severe radiocapitellar arthritis; Asymptomatic partial tears found incidentally. |
Pre-Operative Planning, Templating, and Patient Positioning
MRI Protocoling and Advanced Imaging Techniques
The foundation of successful upper extremity surgery begins in the radiology suite. Standard non-contrast MRI is often insufficient for evaluating the intricate intra-articular structures of the shoulder, wrist, and elbow. Musculoskeletal radiologists and orthopedic surgeons must collaborate to tailor the pulse sequences and optimize the field of view (FOV). For the shoulder, MR arthrography (utilizing a dilute gadolinium solution injected intra-articularly) is the gold standard for delineating labral tears, capsular redundancy, and partial-thickness rotator cuff tears. The addition of the ABER (Abduction and External Rotation) view places the anterior band of the IGHL under tension, dramatically increasing the sensitivity for detecting subtle anteroinferior labral avulsions (Bankart, ALPSA, Perthes lesions).
When evaluating the elbow, particularly the UCL, high-resolution coronal and axial T1 and T2 fat-suppressed images are paramount. The presence of a "T-sign" on MR arthrography—where contrast material extends medial to the sublime tubercle footprint—is pathognomonic for a distal UCL undersurface tear. Furthermore, for suspected distal biceps tendon ruptures, the FABS (Flexed, Abducted, Supinated) position is critical. This specialized view aligns the distal biceps tendon parallel to the main magnetic field, eliminating magic angle artifact and allowing for precise assessment of tendon retraction, which directly dictates the necessity for an extensile surgical approach or allograft reconstruction.
Operating Room Setup and Positioning Strategies
Meticulous patient positioning and operating room setup are critical to minimizing intraoperative complications and maximizing surgical efficiency. For arthroscopic shoulder stabilization, the surgeon must choose between the lateral decubitus and the beach-chair positions. The lateral decubitus position requires a beanbag positioner and a specialized traction setup (typically 10-15 lbs of balanced suspension traction applied via a sterile sleeve), which provides excellent distraction of the glenohumeral joint and unparalleled visualization of the inferior capsule. Conversely, the beach-chair position offers a more anatomical orientation, facilitates easier conversion to an open approach if necessary, and minimizes the risk of traction-related neurapraxia, though it requires careful management of cerebral perfusion pressure by the anesthesia team.
For wrist arthroscopy and TFCC repair, the patient is placed supine with the operative arm extended on a specialized radiolucent hand table. The elbow is flexed to 90 degrees, and the hand is suspended in a vertical traction tower. Finger traps are applied to the index and middle fingers, and 10 to 12 lbs of longitudinal traction is utilized to distract the radiocarpal and midcarpal joints. A non-sterile tourniquet is placed high on the brachium. For elbow procedures such as UCL reconstruction, the patient is positioned supine with the arm abducted on a standard arm board. The shoulder is externally rotated to allow unrestricted access to the medial aspect of the elbow. A sterile tourniquet is often preferred to maximize the surgical field, and the entire upper extremity must be prepped and draped free to allow for dynamic intraoperative assessment of valgus stability and full range of motion.
Step-by-Step Surgical Approach and Fixation Technique
Arthroscopic Anterior Shoulder Stabilization (Bankart Repair)
The arthroscopic Bankart repair aims to anatomically restore the capsulolabral complex to the anterior glenoid rim, recreating the bumper effect and tensioning the IGHL. Following the establishment of a standard posterior viewing portal, a thorough diagnostic arthroscopy is performed. Anteroinferior (5 o'clock) and anterosuperior (3 o'clock) working portals are established using an outside-in spinal needle localization technique, ensuring precise trajectory to the glenoid rim. Clear cannulas are inserted to facilitate suture management.
The first critical step is the mobilization of the torn labrum and capsule. Using an arthroscopic elevator and electrocautery, the capsulolabral tissue is aggressively freed from the anterior glenoid neck. It is absolutely imperative to release the tissue inferiorly to the 6 o'clock position; failure to do so will prevent the necessary superior shift of the IGHL during the repair, leading to residual laxity. Once mobilized, the anterior glenoid neck is meticulously decorticated using a motorized burr or rasp to create a bleeding bone bed, which is essential for promoting biological healing of the soft tissue to the bone.
Suture anchor placement begins at the most inferior aspect of the tear, typically at the 5:30 position. Modern all-suture or biocomposite anchors (1.5mm to 2.9mm) are placed directly on the articular margin to avoid medializing the repair. A suture-shuttling device (e.g., a spectrum hook or lasso) is passed through the capsulolabral tissue, taking a healthy "bite" of the IGHL inferior to the anchor. The suture is retrieved and tied using a sliding-locking knot backed up by alternating half-hitches, effectively shifting the capsule superiorly and laterally. This process is repeated sequentially moving superiorly, typically requiring three to four anchors (at 5:30, 4:30, 3:30, and 2:30) to achieve a robust, watertight repair that restores the normal concavity of the glenoid.
Arthroscopic TFCC Repair (Outside-In Technique)
Repair of a Palmer Class 1B TFCC tear (ulnar avulsion) requires precise reattachment of the peripheral fibrocartilage to the highly vascularized ulnar capsule. Following suspension in the traction tower, standard radiocarpal portals (3-4 and 4-5) are established. The 6R portal is often utilized for optimal viewing of the ulnar periphery. A thorough diagnostic sweep is performed, and the central articular disc is evaluated for concomitant perforations.
Once the peripheral tear is identified, the intervening synovitis and scar tissue are cleared using a 2.0 mm or 2.9 mm full-radius shaver. The ulnar capsule is aggressively abraded to stimulate a local inflammatory and healing response. The outside-in repair technique utilizes specialized spinal needles. A small incision is made over the ulnar aspect of the wrist. A spinal needle is introduced just volar to the extensor carpi ulnaris (ECU) tendon, piercing the ulnar capsule and passing through the volar peripheral edge of the torn TFCC. A monofilament PDS suture is shuttled through the needle into the joint and retrieved via the 3-4 portal.
A second spinal needle is then passed just dorsal to the ECU tendon, traversing the capsule and the dorsal peripheral edge of the TFCC tear. A wire loop or a second suture is passed, and the initial PDS suture is shuttled out through the dorsal needle track. This creates a horizontal mattress configuration across the torn TFCC. The knot is tied blindly over the ulnar capsule (but strictly deep to the ECU tendon and dorsal sensory branch of the ulnar nerve), securely reducing the TFCC to its anatomic footprint at the fovea. The DRUJ is then dynamically tested to confirm the restoration of stability.
Ulnar Collateral Ligament Reconstruction (Tommy John Surgery)
The reconstruction of the UCL is a technically demanding open procedure designed to restore valgus stability while preserving the delicate neurovascular structures of the medial elbow. A medial longitudinal incision is made, centered over the medial epicondyle. The medial antebrachial cutaneous nerve branches are identified and protected. The ulnar nerve is carefully decompressed within the cubital tunnel. Depending on the patient's preoperative symptoms and the surgeon's preference, the nerve may be left in situ or transposed anteriorly (subcutaneous or submuscular).
The flexor-pronator mass is split longitudinally in line with its fibers to expose the native, attenuated UCL. The ligament is incised longitudinally to expose the joint and inspect the undersurface. Bone tunnels are then created. On the ulnar side, two convergent tunnels are drilled into the sublime tubercle using a 3.2 mm drill bit, leaving a 1 cm bone bridge. On the humeral side, the anatomic origin of the anterior bundle on the medial epicondyle is identified. Depending on the specific technique (e.g., modified Jobe, docking, or interference screw technique), a single socket or convergent tunnels are drilled into the epicondyle.
An autograft, typically the palmaris longus or gracilis tendon, is harvested and prepared. The graft is passed through the ulnar tunnels and then routed into the humeral tunnels in a figure-of-eight or docking configuration. The critical step is tensioning: the graft must be tensioned with the elbow positioned in approximately 30 degrees of flexion while a strict varus force is applied to close the medial joint space. The graft is then secured using non-absorbable sutures tied over bone bridges or via bioabsorbable interference screws. The flexor-pronator split is closed, and the arm is immobilized to protect the nascent reconstruction.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique and advanced preoperative imaging, surgical interventions of the upper extremity carry inherent risks. Complications can range from minor transient neuropathies to catastrophic hardware failures and devastating joint stiffness. The orthopedic surgeon must be intimately familiar with the etiology of these complications and possess a robust armamentarium of salvage strategies.
In shoulder stabilization, recurrent instability remains the most significant complication, occurring in 5% to 15% of arthroscopic Bankart repairs. Recurrence is strongly correlated with unrecognized critical glenoid bone loss (typically >20%), inadequate capsular plication, or premature return to contact sports. When an arthroscopic soft-tissue repair fails, the primary salvage strategy is an open osseous augmentation procedure, such as the Latarjet procedure (coracoid transfer) or an iliac crest bone block, to restore the glenoid articular arc. Another severe complication is iatrogenic nerve injury; during the decompression of spinoglenoid notch cysts, overzealous dissection medial to the base of the coracoid or posterior to the glenoid neck can result in transection or traction injury to the suprascapular nerve or artery.
In the wrist and elbow, stiffness and hardware-related issues predominate. Following TFCC repair, DRUJ stiffness and loss of pronosupination are common if immobilization is prolonged beyond 4 to 6 weeks. Additionally, knots tied too superficially during outside-in TFCC repairs can cause severe ECU tendinitis or irritation of the dorsal sensory branch of the ulnar nerve, necessitating secondary knot excision. Following UCL reconstruction, ulnar neuropathy is the most frequent complication, occurring in up to 10% to 15% of cases, particularly when the nerve is aggressively mobilized or transposed. Salvage management for recalcitrant ulnar neuritis may require revision neurolysis and submuscular transposition.
| Complication | Incidence (%) | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Recurrent Anterior Shoulder Instability | 5% - 15% | Unrecognized glenoid bone loss (>20%); Poor tissue quality; Non-compliance with rehab. | Revision to open Latarjet procedure or Iliac Crest Bone Graft (ICBG) augmentation. |
| Iatrogenic Suprascapular Nerve Injury | < 1% | Aggressive dissection during cyst decompression at the spinoglenoid notch. | Observation and EMG monitoring; Nerve exploration and grafting if no recovery at 3-6 months. |
| Ulnar Neuropathy (Post-UCL Recon) | 5% - 15% | Traction during surgery; Scarring in the cubital tunnel; Compression from transposition fascial slings. | Conservative management (gabapentin, NSAIDs); Revision neurolysis and submuscular transposition. |
| DRUJ Stiffness (Post-TFCC Repair) | 10% - 20% | Prolonged immobilization >6 weeks; Over-tensioning of the capsular repair. | Aggressive dynamic splinting and therapy; Arthroscopic or open capsular release if refractory. |
| ECU Tendinitis / Irritation | 5% - 10% | Prominent suture knots from outside-in TFCC repair rubbing against the ECU sheath. | Corticosteroid injection; Minor surgical procedure for knot excision and sheath debridement. |
Phased Post-Operative Rehabilitation Protocols
Shoulder Stabilization Rehabilitation
The postoperative rehabilitation following an arthroscopic Bankart repair is a delicate balance between protecting the healing capsulolabral tissues and preventing adhesive capsulitis. The protocol is strictly phased. Phase I (0
