Radius Anterior Approach: Safe Nerve Protection & Complete Exposure
Key Takeaway
Your ultimate guide to Radius Anterior Approach: Safe Nerve Protection & Complete Exposure starts here. The radius anterior approach, or Henry's approach, is a surgical technique offering safe, excellent exposure of the entire radius. It is used for treating fractures, nonunions, osteotomies, and bone tumors. This approach carefully avoids injury to the posterior interosseous nerve by subperiosteally stripping the supinator muscle, using it to protect the nerve during the procedure.
Introduction and Epidemiology
The anterior approach to the radius, classically described by Arnold K. Henry, remains one of the most versatile and highly utilized extensile exposures in orthopedic surgery. This approach provides safe, comprehensive access to the entire volar surface of the radius, from the bicipital tuberosity proximally to the radiocarpal joint distally. While isolated distal radius fractures frequently utilize a limited distal variation of this approach for volar locked plating, the classic extensile Henry approach is paramount for managing complex diaphyseal fractures, nonunions, tumors, and chronic osteomyelitis.
Epidemiologically, radial shaft fractures often occur in conjunction with ulnar shaft fractures (both-bone forearm fractures) or as isolated injuries such as Galeazzi fracture-dislocations. Diaphyseal forearm fractures account for approximately 10 to 14 percent of all fractures in the upper extremity. Because the forearm functions essentially as a complex joint facilitating pronation and supination, precise anatomic reduction of the radial bow is mandatory. The anterior approach facilitates this by allowing direct visualization of the fracture site, enabling rigid internal fixation while systematically protecting critical neurovascular structures.
The primary advantage of the anterior approach over the dorsal (Thompson) approach is its exploitation of a true internervous plane throughout the entire length of the forearm. By navigating between muscles innervated by the radial and median nerves, the surgeon can achieve wide exposure without denervating the forearm musculature.
Surgical Anatomy and Biomechanics
A profound understanding of forearm anatomy and biomechanics is critical for executing the anterior approach safely. The radius is not a straight bone; it possesses a complex, triplanar curvature known as the radial bow. The maximum radial bow occurs at the middle third of the diaphysis and is essential for generating the torque required for full pronation and supination. Failure to restore this bow during fracture fixation invariably leads to restricted rotational kinematics.
Osteology and Musculature
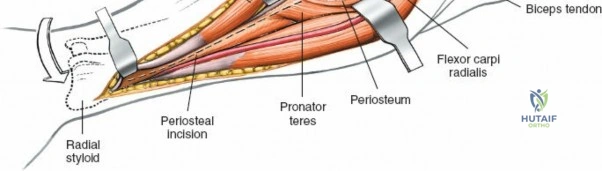
The anterior surface of the radius serves as the origin and insertion point for several key muscles. Proximally, the bicipital tuberosity accepts the insertion of the biceps brachii tendon. The supinator muscle wraps around the proximal third of the radius. In the middle third, the pronator teres inserts on the lateral convexity of the radius. Distally, the flexor pollicis longus originates from the anterior diaphyseal surface, while the pronator quadratus spans the distal radioulnar articulation.
The musculature of the volar forearm is divided into functional compartments. The "mobile wad of Henry" consists of the brachioradialis, extensor carpi radialis longus, and extensor carpi radialis brevis. The volar flexor-pronator mass includes the pronator teres, flexor carpi radialis, palmaris longus, flexor digitorum superficialis, and flexor carpi ulnaris. The internervous plane of the anterior approach capitalizes on the separation between the mobile wad and the flexor-pronator mass.
Neurovascular Anatomy
The primary structures at risk during the anterior approach are the posterior interosseous nerve, the superficial radial nerve, and the radial artery.
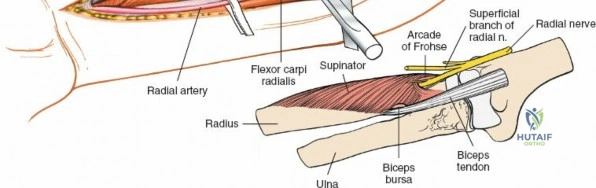
The radial nerve bifurcates into the deep posterior interosseous nerve and the superficial sensory radial nerve at the level of the radiocapitellar joint. The posterior interosseous nerve dives dorsally through the Arcade of Frohse and between the two heads of the supinator muscle. Exposing the proximal third of the radius places this nerve in direct jeopardy.
The radial artery runs distally down the forearm under the medial edge of the brachioradialis. In the proximal forearm, it gives off the radial recurrent artery, which forms a vascular plexus often referred to as the "leash of Henry." These vessels must be meticulously ligated to mobilize the brachioradialis laterally and access the proximal radius.

Indications and Contraindications
The extensile anterior approach is highly versatile. Decision-making regarding its use depends on the pathology, the level of the radial involvement, and the condition of the soft tissue envelope.
Surgical Indications
The uses of the anterior approach include:
* Open reduction and internal fixation of radial shaft fractures and Galeazzi fractures.
* Bone grafting and rigid fixation of fracture nonunions or malunions.
* Radial osteotomy for deformity correction.
* Biopsy and en bloc resection of bone tumors.
* Excision of sequestra in cases of chronic osteomyelitis.
* Anterior exposure of the bicipital tuberosity for distal biceps tendon repairs.
* Fasciotomy for the treatment of acute compartment syndrome of the forearm.
Relative Contraindications
Contraindications are primarily relative and include active soft tissue infection over the volar forearm, severe traumatic compromise of the anterior soft tissue envelope (e.g., massive degloving), or specific proximal radius fracture patterns that are strictly dorsal and better addressed via a Thompson approach.
Operative Versus Non Operative Management Parameters
| Management Strategy | Clinical Scenario | Rationale and Biomechanical Objective |
|---|---|---|
| Non-Operative | Nondisplaced isolated radial shaft fractures (rare in adults); Pediatric plastic deformation or greenstick fractures. | Cast immobilization (long arm cast). Pediatric bone possesses high remodeling potential. Adult nondisplaced fractures require close serial radiographic monitoring. |
| Operative (ORIF) | Displaced radial shaft fractures; Galeazzi fractures; Both-bone forearm fractures; Open fractures. | Restoration of radial bow, length, and rotation. Dynamic compression plating achieves absolute stability, allowing early active range of motion and preventing radioulnar synostosis. |
| Operative (Excision/Grafting) | Atrophic nonunions; Chronic osteomyelitis with sequestrum. | Debridement of avascular bone, restoration of biology via autologous bone grafting (e.g., iliac crest), and revision rigid fixation. |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is mandatory to ensure adequate exposure and appropriate implant selection. Standard orthogonal anteroposterior and lateral radiographs of the forearm, including the elbow and wrist joints, are required to evaluate the fracture pattern, assess the radioulnar joints, and measure the radial bow. Contralateral radiographs may be obtained in cases of complex comminution or nonunion to template the native radial bow.
Patient Positioning Details
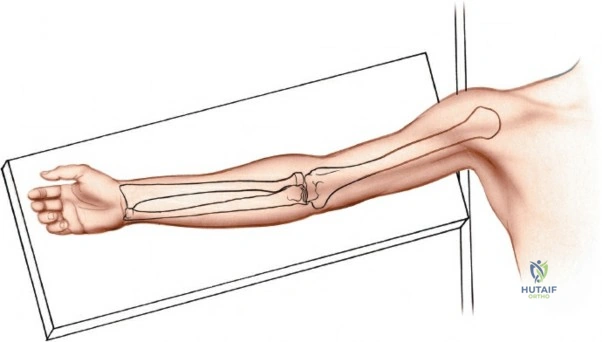
Place the patient supine on the operating table. The affected extremity is extended onto a radiolucent hand table or arm board to facilitate intraoperative fluoroscopy.
Apply a pneumatic tourniquet high on the brachium. A critical technical pearl regarding exsanguination: do not exsanguinate the arm fully with an Esmarch bandage before inflating the tourniquet. Elevating the arm for two minutes prior to inflation is sufficient. Leaving venous blood in the upper extremity makes the delicate vascular structures, particularly the radial recurrent veins within the leash of Henry, significantly easier to identify and ligate during the superficial dissection.
Finally, position the forearm in supination. Supination is the most critical positional requirement, as it rotates the posterior interosseous nerve away from the anterior surgical field, maximizing the safety margin during proximal dissection.
Detailed Surgical Approach and Technique
The anterior approach can be tailored to expose the entire radius or limited to specific thirds (proximal, middle, or distal) depending on the pathology.
Landmarks and Incision Planning
Accurate palpation of surface anatomy dictates the incision trajectory.
1. Palpate the biceps tendon, a taut cord crossing the anterior elbow joint medial to the brachioradialis.
2. Palpate the brachioradialis, the fleshy bulk forming the lateral mobile wad.
3. Palpate the styloid process of the radius, which represents the most distal aspect of the lateral radius when the forearm is supinated.
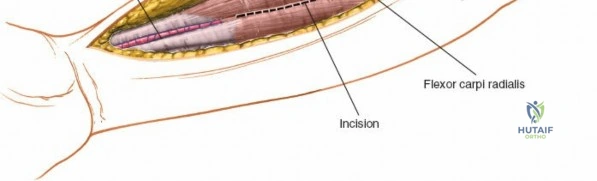
Make a straight longitudinal incision beginning at the anterior flexor crease of the elbow, just lateral to the biceps tendon, extending distally to the radial styloid. The exact length of the incision is dictated by the extent of the diaphyseal involvement.
Superficial Dissection and Internervous Planes
The approach relies on a continuous internervous plane that shifts depending on the level of the forearm.
Distal Internervous Plane:
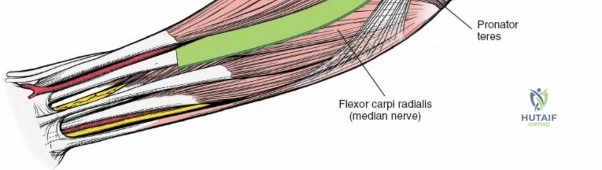
In the distal half of the forearm, the internervous plane lies between the brachioradialis muscle (innervated by the radial nerve) and the flexor carpi radialis muscle (innervated by the median nerve).
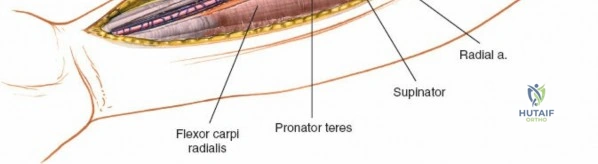
Proximal Internervous Plane:
In the proximal half of the forearm, the plane lies between the brachioradialis muscle (radial nerve) and the pronator teres muscle (median nerve).
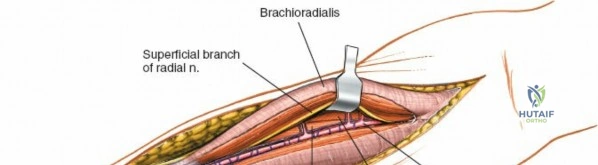
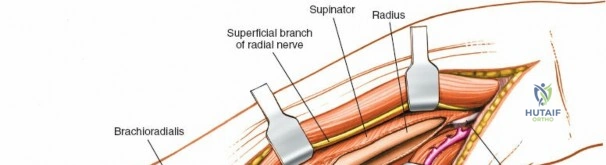
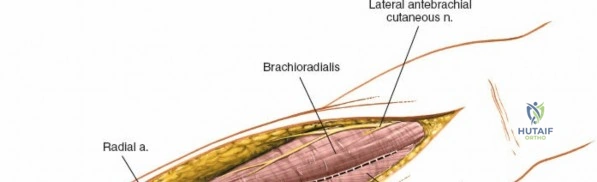
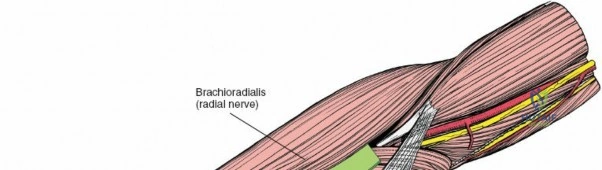
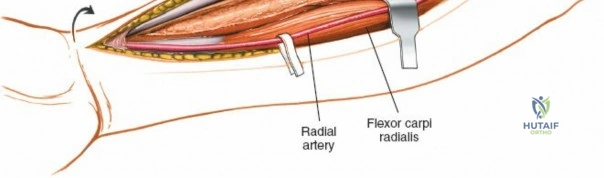
Incise the deep fascia of the forearm in line with the skin incision. Identify the medial border of the brachioradialis. Retract the brachioradialis laterally. At this stage, the superficial radial nerve will be visible on the undersurface of the brachioradialis; it must be protected and retracted laterally with the muscle belly.
Simultaneously, identify the radial artery running alongside the flexor carpi radialis. The artery is typically mobilized medially with the flexor-pronator mass to protect it from the retractors.
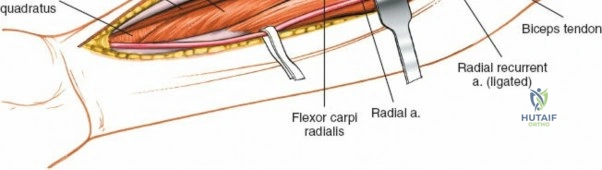
Managing the Leash of Henry
To mobilize the brachioradialis fully and access the proximal third of the radius, the radial artery's recurrent branches must be addressed. The radial recurrent artery and its associated veins form the "leash of Henry," which tethers the mobile wad to the central vascular bundle. Isolate, ligate, and divide these vessels. Electrocoagulation can be used for smaller veins, but formal suture ligation or surgical clips are recommended for the arterial branches to prevent postoperative hematoma.
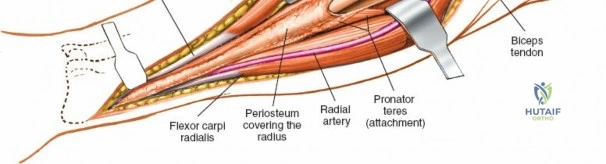
Deep Dissection of the Proximal Third
Exposing the proximal third of the radius is the most hazardous portion of the procedure due to the proximity of the posterior interosseous nerve.
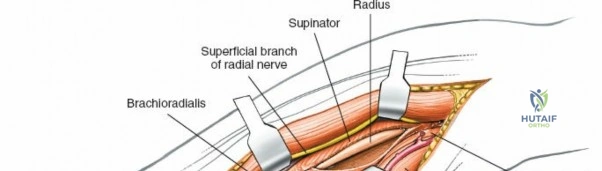
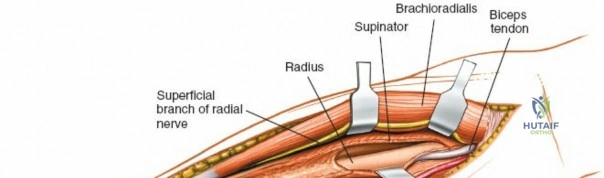
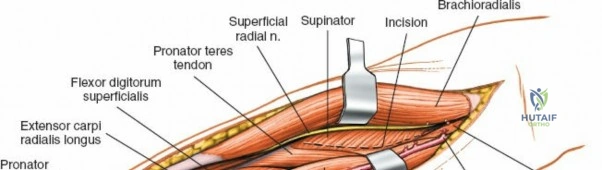
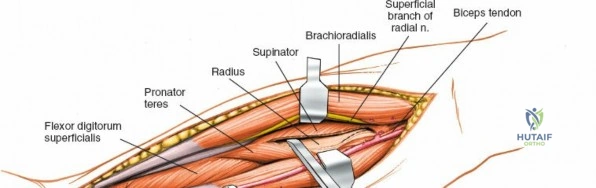
With the forearm fully supinated, identify the supinator muscle wrapping around the proximal radius. The posterior interosseous nerve runs within the substance of this muscle. To safely expose the bone, the supinator must be detached from its insertion on the anterior aspect of the radius.

Incise the supinator insertion sharply along the anterior ridge of the radius. Elevate the muscle belly subperiosteally from medial to lateral. By maintaining a strict subperiosteal plane, the supinator muscle belly acts as a protective cushion for the posterior interosseous nerve.
Critical Retractor Placement: Great care must be taken in positioning retractors. The posterior interosseous nerve may physically contact the bone at the level of the distal radial neck, directly opposite the bicipital tuberosity. Posteriorly placed Hohmann retractors can easily compress the nerve against the radial neck, resulting in iatrogenic neurapraxia. Always place retractors gently and ensure they rest subperiosteally.
Deep Dissection of the Middle Third
In the middle third of the diaphysis, the pronator teres inserts onto the lateral aspect of the radius. For midshaft fractures, this insertion often requires partial elevation. Supinate the forearm to bring the insertion anteriorly. Detach the pronator teres from its footprint using electrocautery or a periosteal elevator. During closure, the pronator teres does not necessarily require formal reattachment, as it will scar into the surrounding fascial tissues without significant loss of pronation strength.
Deep Dissection of the Distal Third
For distal shaft exposures, the flexor pollicis longus and the pronator quadratus must be elevated. The flexor pollicis longus originates from the anterior surface of the radius. Retract its muscle belly medially.
The pronator quadratus covers the distal quarter of the radius. Incise its lateral border (the radial insertion) and elevate it subperiosteally from lateral to medial. This exposes the flat volar surface of the distal radius, providing an excellent bed for plate application.
Fracture Reduction and Plate Application
Once the entire necessary length of the radius is exposed, debride the fracture ends. Hematoma and interposed soft tissue must be cleared. Reduce the fracture using reduction forceps, ensuring absolute restoration of the radial bow.
Apply a dynamic compression plate (typically a 3.5mm limited contact dynamic compression plate or a locking compression plate, depending on bone quality) to the volar surface. The volar surface is flat distally, making it biomechanically and anatomically ideal for plate seating. Ensure that proximal screws do not inadvertently injure the posterior interosseous nerve by penetrating too far past the dorsal cortex.
Complications and Management
While the anterior approach provides unparalleled exposure, it carries specific risks that demand meticulous surgical technique. Iatrogenic neurovascular injuries and functional deficits can occur if anatomic boundaries are disrespected.
Posterior Interosseous Nerve Palsy
The most feared complication is injury to the posterior interosseous nerve. This typically manifests as an inability to extend the metacarpophalangeal joints and the thumb, though wrist extension is partially preserved (with radial deviation) due to the intact innervation of the extensor carpi radialis longus (supplied by the radial nerve proximal to its bifurcation). Injury usually results from excessive traction, poor retractor placement at the radial neck, or failure to maintain a subperiosteal plane during supinator elevation.
Superficial Radial Nerve Neuroma
The superficial radial nerve is at risk during the superficial dissection and mobilization of the brachioradialis. Aggressive retraction can cause neurapraxia, or direct laceration can lead to a painful neuroma. The nerve must be identified early and retracted gently with the brachioradialis muscle belly.
Radioulnar Synostosis
Cross-union between the radius and ulna is a devastating complication that abolishes forearm rotation. The risk is highest in proximal third fractures, highly comminuted both-bone forearm fractures, and cases involving severe soft tissue trauma or delayed surgery.
Complication Incidence and Salvage Strategies
| Complication | Estimated Incidence | Avoidance and Salvage Strategy |
|---|---|---|
| Posterior Interosseous Nerve Palsy | 2% - 5% | Avoidance: Full supination during proximal dissection; strictly subperiosteal supinator elevation; avoid dorsal retractor placement. Salvage: Observation for 3-6 months (most are neurapraxias). If no recovery, EMG/NCS followed by nerve exploration or tendon transfers. |
| Superficial Radial Nerve Injury | 1% - 3% | Avoidance: Identify under BR early; retract laterally with the muscle. Salvage: Neuroma excision and burying the proximal stump into the brachioradialis muscle belly. |
| Radioulnar Synostosis | 2% - 8% | Avoidance: Use separate approaches for radius and ulna in both-bone fractures; meticulous hemostasis; copious irrigation of bone dust. Salvage: Surgical excision of the synostosis after maturation (typically 6-12 months post-injury), combined with radiation prophylaxis or Indomethacin. |
| Loss of Forearm Rotation | 10% - 15% | Avoidance: Anatomic restoration of the radial bow; rigid fixation allowing early active ROM. Salvage: Hardware removal if impinging; corrective osteotomy for malunion. |
Post Operative Rehabilitation Protocols
Immediate postoperative management focuses on edema control and the prevention of joint stiffness. The rigidity of modern internal fixation constructs generally allows for early mobilization, which is critical for restoring the complex kinematics of the forearm.
Immediate Post Operative Phase
The patient is placed in a bulky soft dressing and a removable volar splint. The arm is elevated to minimize swelling. Active and active-assisted range of motion of the fingers, thumb, and shoulder is initiated immediately in the recovery room to prevent secondary stiffness and promote venous return.
Early Mobilization Phase
Assuming absolute stability was achieved with dynamic compression plating, the splint can be removed for supervised physical therapy within the first 3 to 5 days. Therapy focuses on active and active-assisted pronation and supination, as well as elbow and wrist flexion and extension. Passive stretching is generally avoided in the early phases to prevent excessive stress on the soft tissues and the fracture site.
Strengthening and Return to Function
Radiographic union is monitored serially, typically at 2, 6, and 12 weeks. Once clinical and radiographic evidence of bridging callus or obliteration of the fracture line is present (usually around 8 to 12 weeks), progressive resistance exercises are initiated. Return to heavy manual labor or contact sports is generally permitted once full radiographic consolidation is achieved and the patient has regained at least 80% of their grip strength and rotational torque compared to the contralateral side.
Summary of Key Literature and Guidelines
The foundational principles of the anterior approach to the radius remain anchored in Arnold K. Henry’s original anatomical descriptions. His meticulous mapping of the internervous planes and the vascular "leash" established the standard for safe volar exposures.
Contemporary guidelines, heavily influenced by the AO Foundation (Arbeitsgemeinschaft für Osteosynthesefragen), emphasize the necessity of absolute stability in diaphyseal forearm fractures. The AO principles dictate that the radius and ulna must be treated as an articular complex. The anterior approach is the preferred method for achieving the direct visualization necessary for anatomic reduction of the radial bow and the application of interfragmentary lag screws and neutralization plates.
Recent anatomical studies have further refined the understanding of the posterior interosseous nerve's trajectory. Literature highlights that the distance from the radiocapitellar joint to the Arcade of Frohse can vary, reinforcing the mandate for subperiosteal elevation of the supinator rather than relying on fixed metric distances to avoid nerve injury. Adherence to these anatomical principles ensures that the anterior approach remains a highly effective and safe procedure in the orthopedic surgeon's armamentarium.
