Mastering Approaches to the Upper Third of the Radius

Key Takeaway
We review everything you need to understand about Mastering Approaches to the Upper Third of the Radius. Surgery involving the proximal third of the radius is complex due to the posterior interosseous nerve, which spirals closely around the bone. This nerve is highly vulnerable during surgical exposure. However, the anterior approach offers safe access to the third of the radius by subperiosteally stripping and utilizing the supinator muscle to protect the posterior interosseous nerve.
Comprehensive Introduction and Patho-Epidemiology
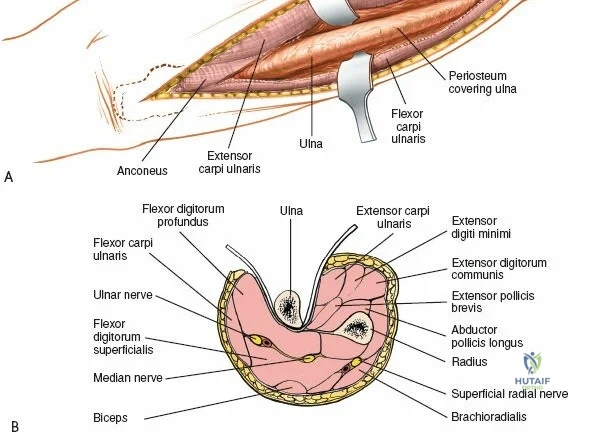
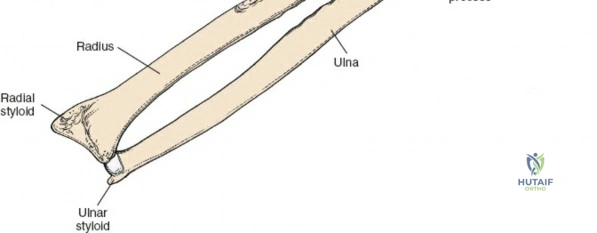
The surgical anatomies of the two bones of the forearm differ significantly, dictating vastly different operative strategies. The ulna features a subcutaneous border that extends for its entire length; the bone can be reached simply and directly via a straightforward approach without endangering major neurovascular structures. In stark contrast, the upper two-thirds of the radius are deeply enclosed by a complex, multi-layered sheath of muscles. Accessing the proximal radius requires a profound understanding of three-dimensional forearm anatomy, as the radius acts not merely as a static strut, but as a rotating lever arm essential for pronation and supination.
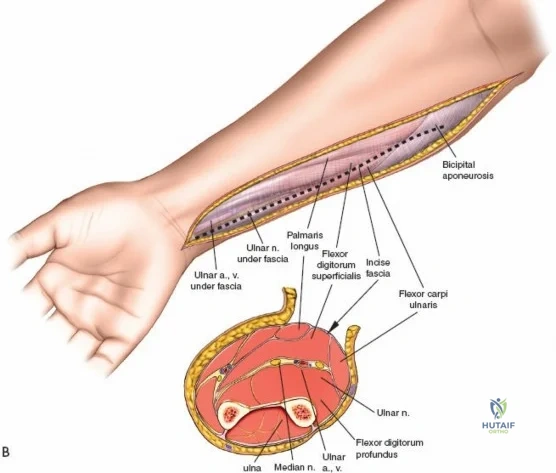
All surgical interventions in the upper third of the radius are complicated by the presence of the posterior interosseous nerve (PIN). This critical motor nerve winds spirally around the proximal radial shaft, often lying in direct contact with the periosteum of the radial neck. The anterior approach to the radius, classically described by A.K. Henry, remains the gold standard extensile exposure. It relies on meticulous subperiosteal dissection and dynamic positioning (supination) to protect the PIN, allowing the surgeon to expose the entire length of the radius from the bicipital tuberosity to the radial styloid.

The epidemiology of proximal radius pathology necessitates a reliable, extensile approach. Fractures of the proximal third of the radius, often occurring as part of a Monteggia fracture-dislocation variant or an isolated high-energy trauma, require anatomic reduction and rigid internal fixation to restore the radial bow and preserve forearm rotation. Furthermore, the upper radius is a frequent site for primary bone tumors, chronic osteomyelitis, and nonunions that demand wide exposure for resection, grafting, or complex reconstruction.
Mastering the anterior approach requires an intimate familiarity with the mobile wad of Henry, the intricate leash of recurrent radial vessels, and the precise internervous planes that safeguard forearm function. While alternative posterior approaches (such as the Thompson approach) exist, the anterior approach is unparalleled in its extensile utility, providing safe, continuous access to the volar surface of the radius while effectively neutralizing the risk to the posterior interosseous nerve when executed correctly.

Detailed Surgical Anatomy and Biomechanics
Osteology and Biomechanics of the Proximal Radius
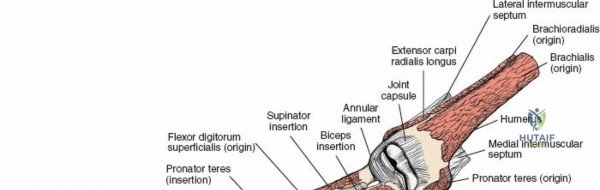
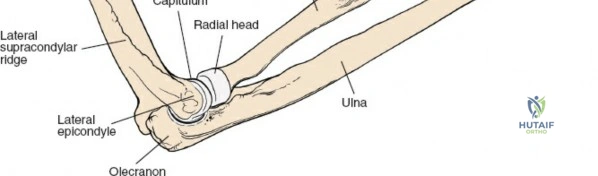
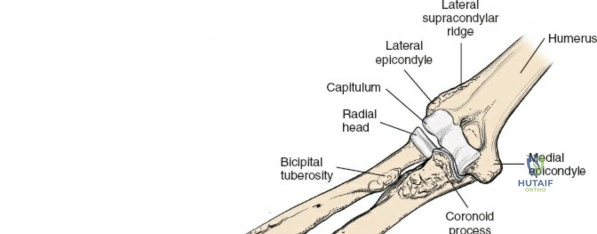
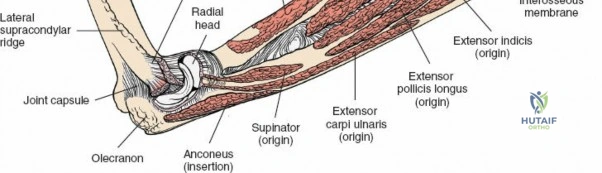
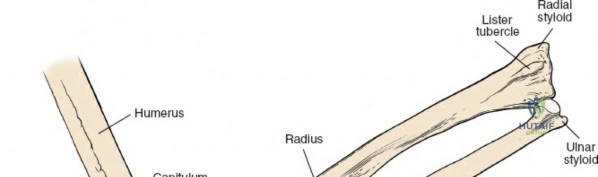
The radius and ulna function together as a highly coordinated articular quadrangle. The proximal radius consists of the radial head, which articulates with the capitellum; the radial neck; and the bicipital tuberosity, which serves as the insertion site for the biceps brachii tendon. The biomechanics of the forearm dictate that the radius rotates around the stationary ulna during pronation and supination. The normal lateral curvature of the radius—the radial bow—is critical for this rotational clearance. Any surgical approach to the proximal radius must allow for the precise restoration of this bow, as even a minor malreduction can lead to profound deficits in forearm rotation.
The Internervous Planes of the Forearm
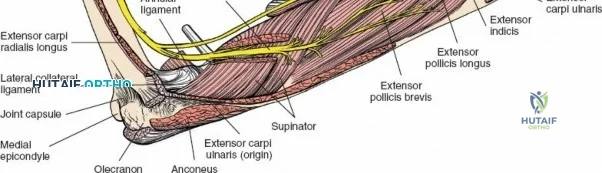
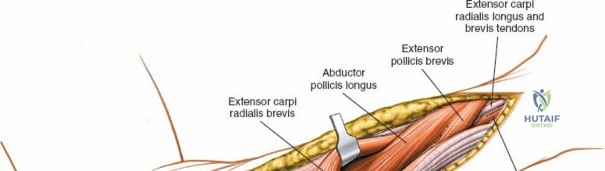
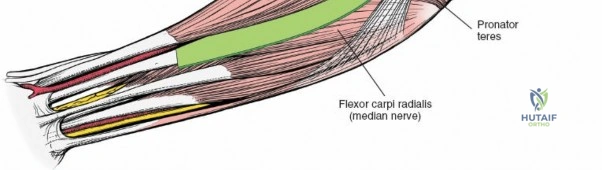
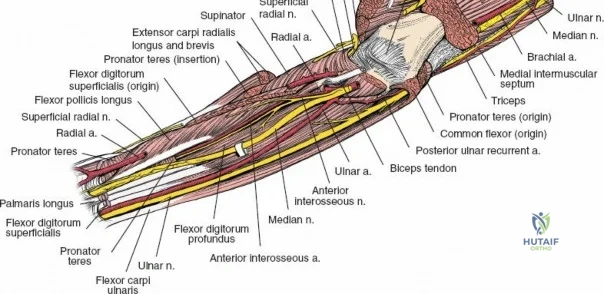
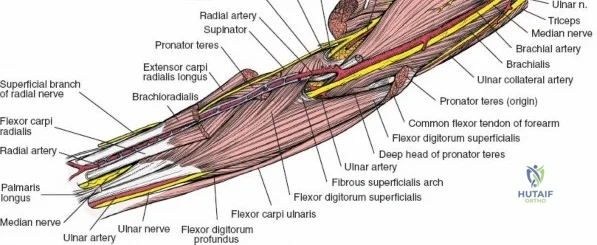
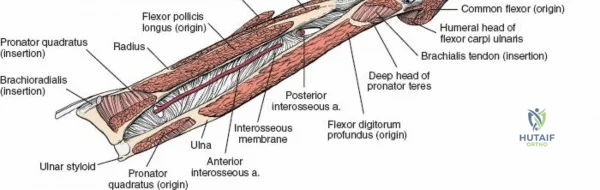
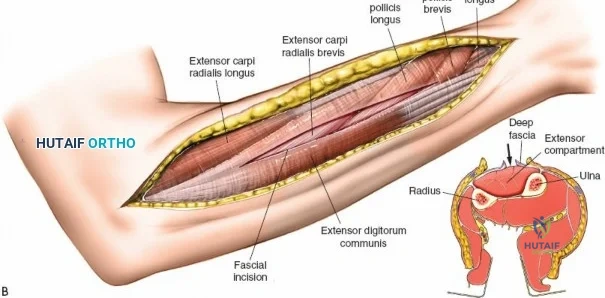
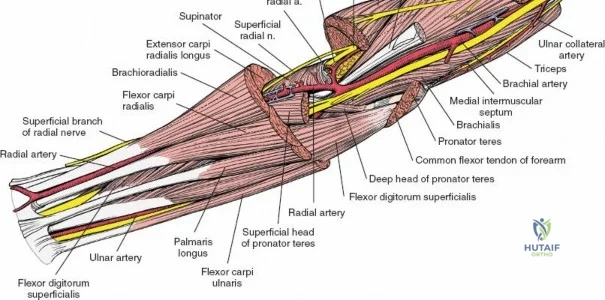
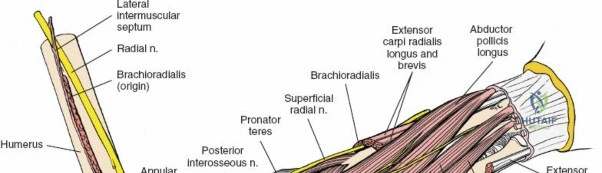
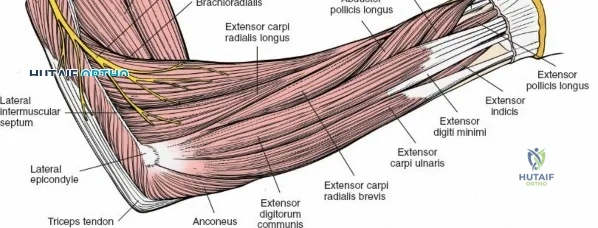
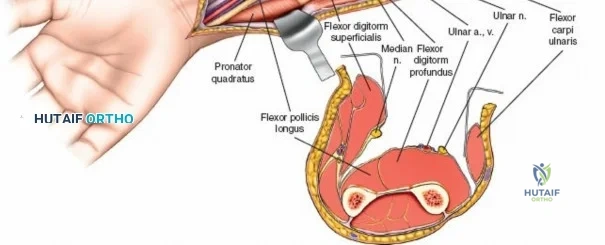
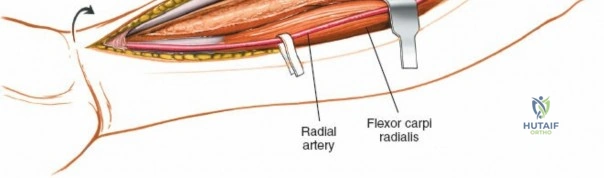
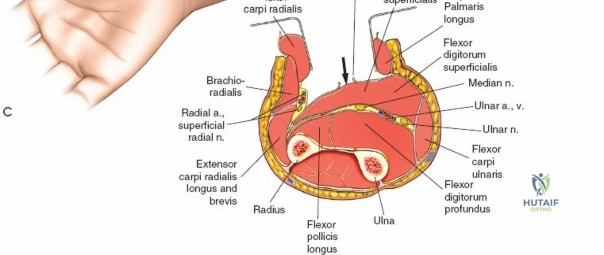
The anterior approach to the radius is an elegant example of utilizing true internervous planes to achieve deep exposure without denervating musculature. Distally, the internervous plane lies between the brachioradialis muscle (innervated by the radial nerve) and the flexor carpi radialis muscle (innervated by the median nerve). Proximally, the plane transitions to lie between the brachioradialis (radial nerve) and the pronator teres muscle (median nerve). Exploiting this plane allows the surgeon to mobilize the entire lateral muscular compartment (the "mobile wad" comprising the brachioradialis, extensor carpi radialis longus, and extensor carpi radialis brevis) away from the anterior flexor compartment.

The Posterior Interosseous Nerve (PIN)
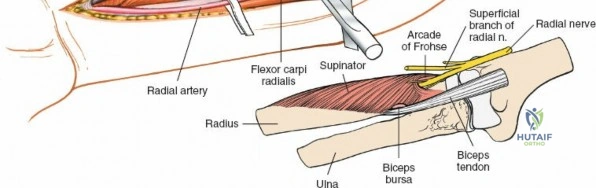
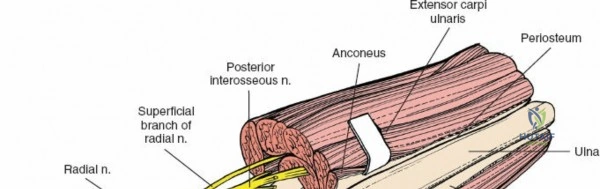
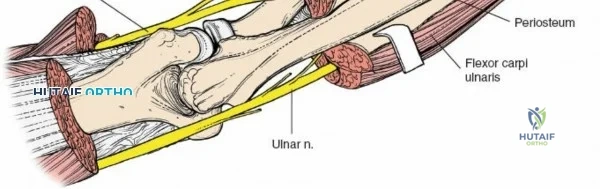
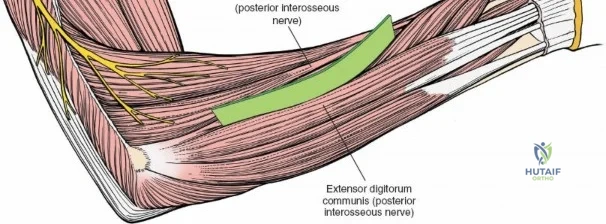
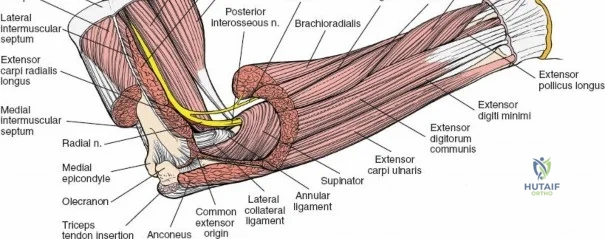
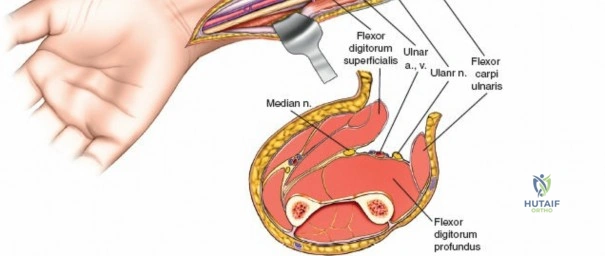
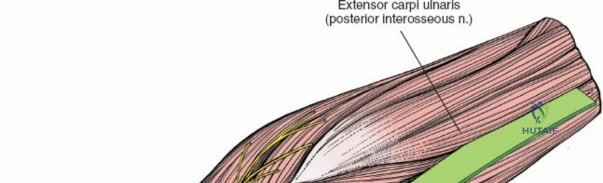
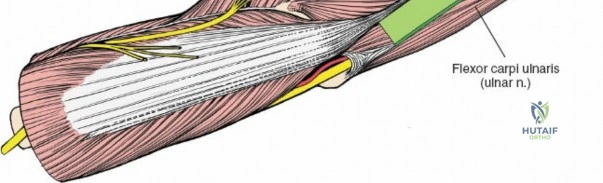
The posterior interosseous nerve is the single most important structure left vulnerable during exposure of the proximal radius. A branch of the radial nerve, the PIN dives into the supinator muscle through the Arcade of Frohse. It travels obliquely and spirally around the radial neck and proximal shaft within the substance of the supinator. In approximately 25% of patients, the nerve comes into direct contact with the posterior periosteum of the radial neck. Therefore, any blind placement of retractors around the posterior aspect of the proximal radius is strictly contraindicated, as it can easily crush the nerve against the bone, resulting in devastating loss of finger and thumb extension.
Vascular Anatomy and the Recurrent Radial Leash
The radial artery runs distally through the forearm, initially lying deep to the brachioradialis muscle before becoming more superficial in the distal third. Just distal to the elbow joint, the radial artery gives off a complex network of vessels known as the recurrent radial artery leash (the "leash of Henry"). These vessels branch laterally to supply the brachioradialis and the mobile wad. To successfully mobilize the brachioradialis laterally and access the proximal radius, this entire leash of vessels must be meticulously isolated, ligated, and divided. Failure to do so will tether the brachioradialis, prevent adequate exposure, and risk severe postoperative hematoma from avulsed vessels.
Exhaustive Indications and Contraindications
The anterior approach to the radius is highly versatile, but patient selection and preoperative planning are paramount. The surgeon must weigh the need for extensile exposure against the specific location of the pathology.
Indications for the Anterior Approach
The primary utility of the anterior approach lies in its extensile nature. It is the approach of choice for open reduction and internal fixation (ORIF) of diaphyseal radius fractures, particularly those involving the proximal or middle thirds. It is also highly indicated for the management of fracture nonunions requiring decortication and structural bone grafting. Oncologic surgeons utilize this approach for the biopsy and wide resection of primary or metastatic bone tumors of the radial shaft. Additionally, chronic osteomyelitis requiring sequestrectomy, radial osteotomies for malunion correction, and anterior exposure of the bicipital tuberosity for distal biceps tendon repairs are classic indications. Finally, it serves as the foundation for volar fasciotomies in the treatment of acute forearm compartment syndrome.
Contraindications and Alternative Approaches
While versatile, the anterior approach is not universally applicable. Isolated fractures of the radial head or neck are generally better served by a direct lateral (Kocher) or posterolateral (Kaplan) approach, which provides more direct articular access without the need for extensive diaphyseal dissection. Similarly, isolated fractures of the distal radius are typically addressed via a modified distal Henry approach (volar approach to the distal radius), which does not require the proximal mobilization of the supinator. Relative contraindications include previous extensive surgical approaches on the posterior aspect of the forearm where the vascularity of the radius may already be compromised, or in cases of severe soft tissue compromise over the anterior forearm.
Summary Table of Indications and Contraindications
| Category | Specific Pathologies / Scenarios | Clinical Rationale |
|---|---|---|
| Primary Indications | Proximal/Middle 1/3 Radius Fractures | Allows extensile exposure for long plates and restoration of the radial bow. |
| Primary Indications | Radial Diaphyseal Nonunions | Facilitates wide exposure for autologous bone grafting and rigid fixation. |
| Primary Indications | Forearm Compartment Syndrome | Provides access for complete volar flexor compartment decompression. |
| Primary Indications | Distal Biceps Tendon Ruptures | Grants direct access to the bicipital tuberosity for anatomic reinsertion. |
| Relative Contraindications | Isolated Radial Head Fractures | A Kocher or Kaplan approach provides superior, less morbid articular access. |
| Absolute Contraindications | Active Anterior Soft Tissue Infection | Incising through infected tissue risks seeding the bone and deep compartments. |
Pre-Operative Planning, Templating, and Patient Positioning
Pre-Operative Templating and Imaging
Meticulous preoperative planning is mandatory for proximal radius surgery. High-quality orthogonal radiographs of the forearm, including the elbow and wrist joints, must be obtained to assess the fracture pattern, the degree of comminution, and the status of the distal radioulnar joint (DRUJ). In cases of complex fractures, tumors, or nonunions, a computed tomography (CT) scan with 3D reconstruction is highly recommended. Templating should be performed to select the appropriate plate length and contour, keeping in mind the normal radial bow. The surgeon must ensure that the chosen fixation construct will not impinge on the PIN or restrict forearm rotation.
Patient Positioning and Operating Room Setup
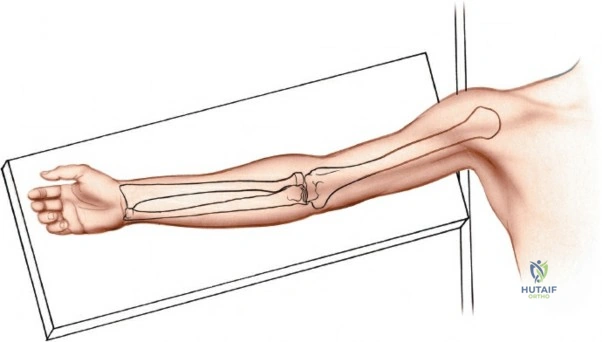
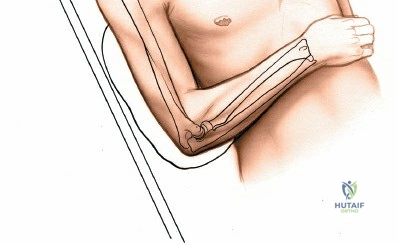
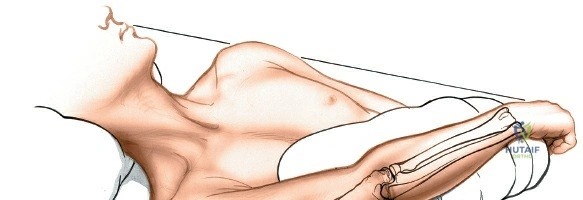
Place the patient supine on the operating table. The affected upper extremity is extended onto a radiolucent hand table or arm board. The shoulder should be abducted to approximately 90 degrees, and the elbow extended. A pneumatic tourniquet is applied high on the brachium. The setup must allow for unimpeded use of intraoperative fluoroscopy (C-arm), which should be positioned parallel to the arm board to allow for easy anterior-posterior and lateral imaging without compromising the sterile field.
The Tourniquet Exsanguination Pearl
A critical, often overlooked technical pearl in the anterior approach to the radius involves the exsanguination process. While standard protocol dictates tight exsanguination with an Esmarch bandage prior to tourniquet inflation, this can completely empty the venous system. In the anterior approach, identifying and ligating the recurrent radial leash of vessels is a pivotal step. If the arm is fully exsanguinated, these delicate veins collapse and become nearly invisible, increasing the risk of avulsion during blunt dissection. Therefore, it is highly recommended to elevate the arm for 2 to 3 minutes to allow for gravity exsanguination, but do not use an Esmarch bandage before inflating the tourniquet. Leaving venous blood in the arm keeps the venae comitantes of the radial artery and the recurrent radial leash engorged, making them vastly easier to identify, isolate, and ligate.
Step-by-Step Surgical Approach and Fixation Technique
Landmarks and Incision Planning
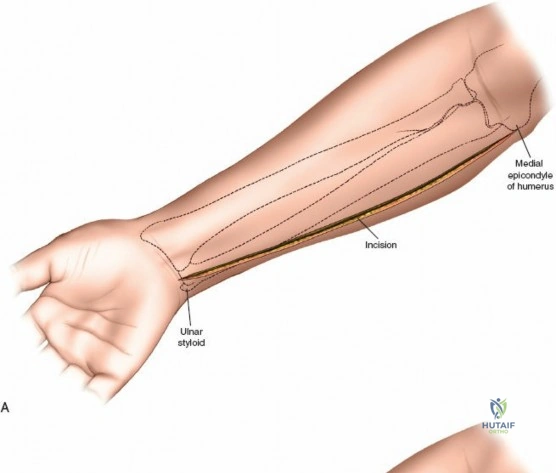
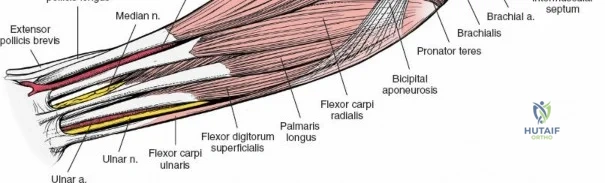
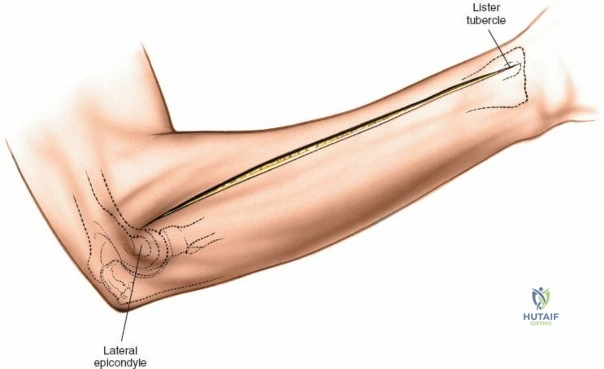
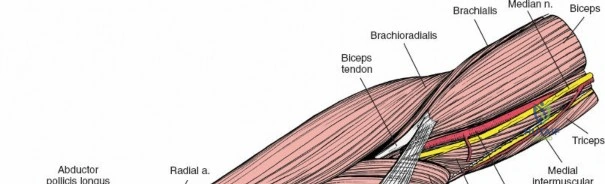
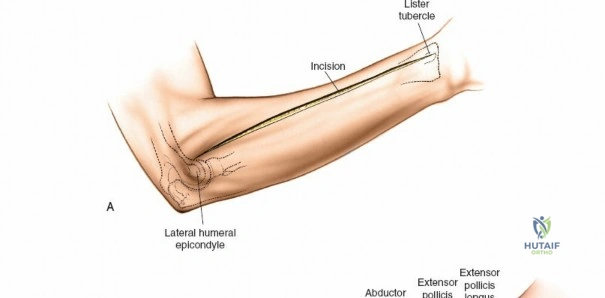
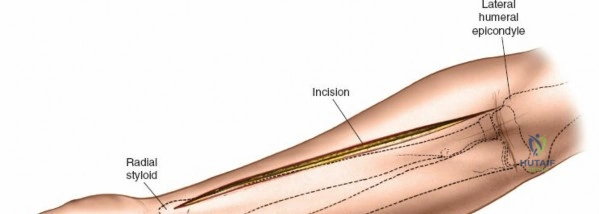
Accurate identification of surface landmarks is the first step in a successful Henry approach. Palpate the biceps tendon, a stout, taut structure crossing the anterior elbow joint just medial to the brachioradialis muscle. Next, palpate the brachioradialis itself, the fleshy muscle forming the lateral border of the cubital fossa. Finally, identify the styloid process of the radius distally. Note that when the forearm is fully supinated (the anatomic position), the radial styloid is truly lateral.
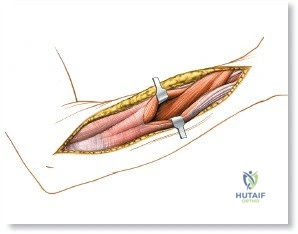
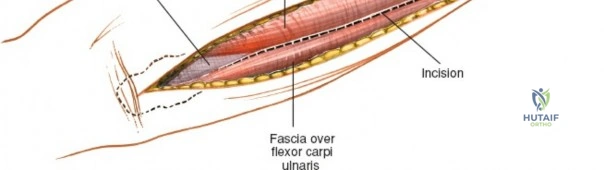
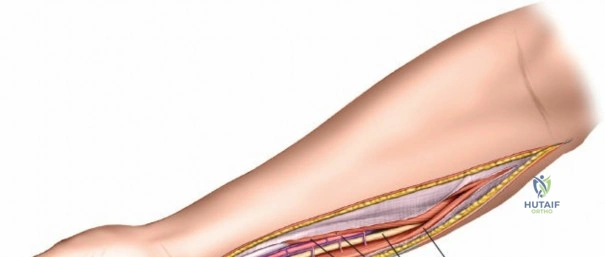
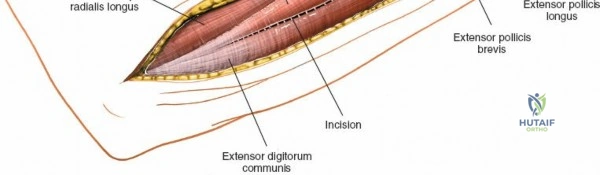
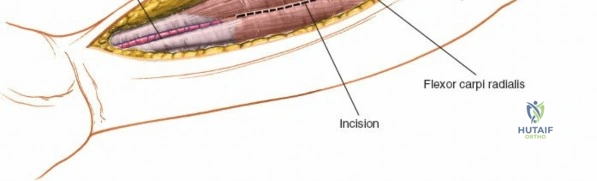
Make a straight or gently curved incision beginning at the anterior flexor crease of the elbow, just lateral to the biceps tendon. Extend this incision distally toward the styloid process of the radius. The exact length and placement of the incision are dictated by the specific pathology; the approach is highly modular, and often only the proximal, middle, or distal third of the incision is required.
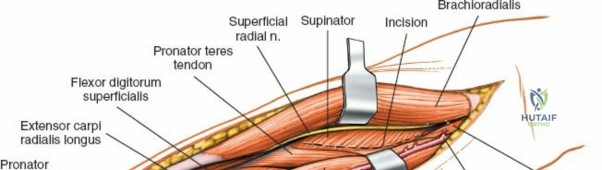
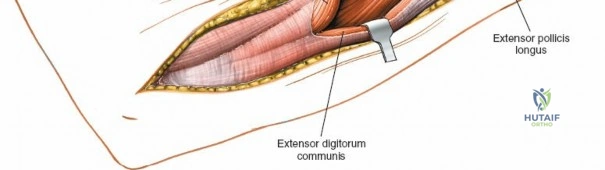
Superficial Surgical Dissection and Internervous Plane
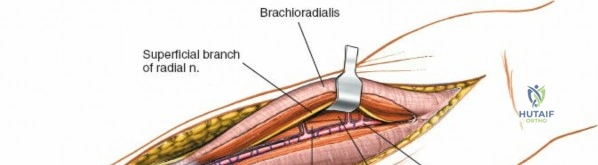
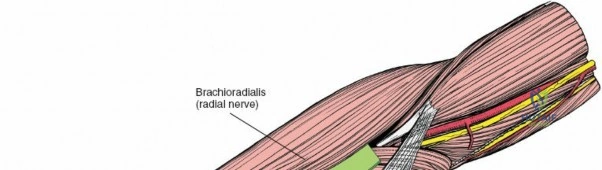
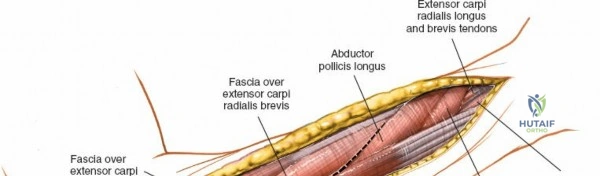
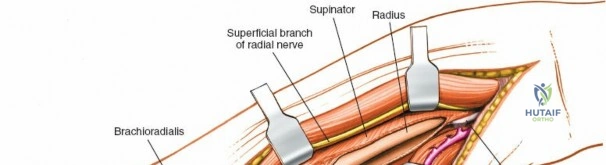
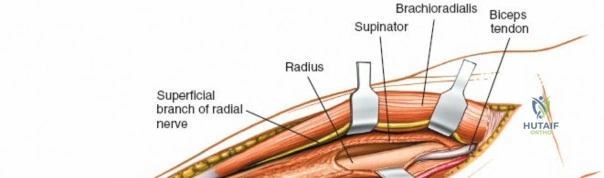
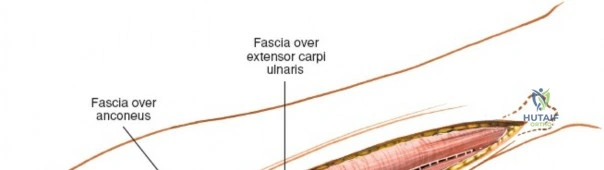
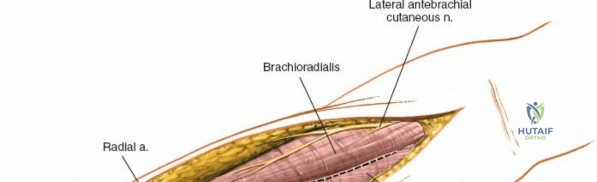
Incise the deep fascia of the forearm in line with the skin incision. The initial goal is to identify the medial border of the brachioradialis as it courses down the forearm. It is a common pitfall to search for this border too far laterally. At the level of the elbow, the brachioradialis is expansive and extends almost halfway across the anterior forearm. It is surprisingly easy to mistake the plane between the brachioradialis and the extensor carpi radialis longus for the correct intermuscular plane.
To confirm the correct plane, look for the superficial branch of the radial nerve. This sensory nerve runs on the undersurface of the brachioradialis muscle. Once the true medial edge of the brachioradialis is found, develop the plane between it and the pronator teres (proximally) or the flexor carpi radialis (distally). Retract the brachioradialis laterally, taking care to keep the superficial radial nerve attached to its undersurface to protect it from traction injury.

Managing the Radial Artery and Recurrent Leash
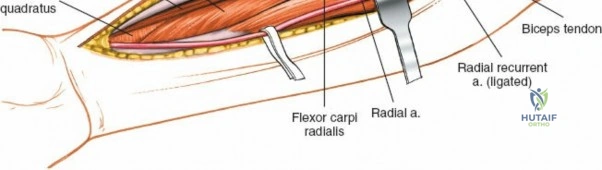
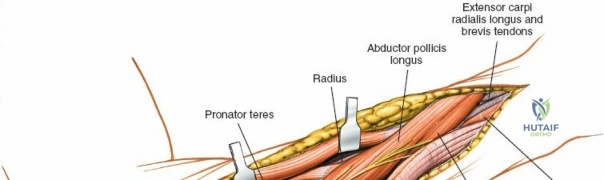
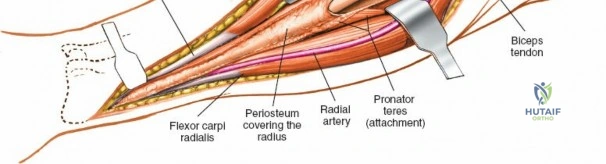
As the brachioradialis is retracted laterally, the radial artery and its venae comitantes are exposed lying deep in the middle part of the forearm, closely related to the medial edge of the wound. Begin dissection distally and work proximally. Just below the elbow joint, the radial artery gives off the recurrent radial artery and a leash of muscular branches that dive laterally into the brachioradialis.
This leash must be meticulously managed. Take time to isolate, ligate, and divide these vessels. Do not attempt to use electrocautery alone on the larger branches, and absolutely avoid blunt avulsion. Avulsion of these vessels from the main radial artery is a potent cause of difficult-to-control intraoperative bleeding and severe postoperative hematoma. Once the leash is divided, the brachioradialis can be fully mobilized laterally, exposing the deep muscular layer.
Deep Surgical Dissection: Exposing the Proximal Third
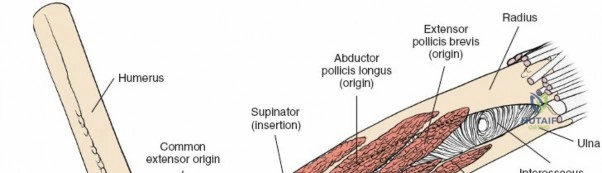
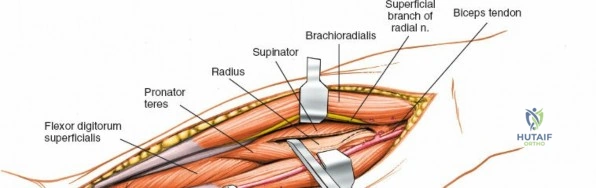
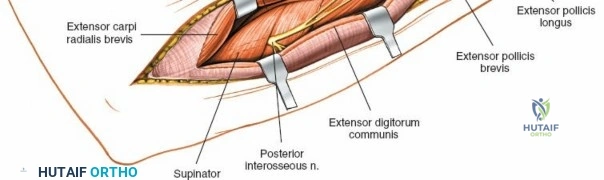
Exposing the proximal third of the radius requires extreme vigilance due to the proximity of the posterior interosseous nerve. The key anatomical landmark here is the insertion of the biceps tendon. Follow the biceps tendon distally to its insertion on the bicipital tuberosity of the radius. A small bursa lies just lateral to the tendon; incise this bursa to gain initial access to the proximal radial shaft. Because the radial artery lies superficial and medial to the tendon at this level, all deep dissection must remain strictly lateral to the biceps tendon.
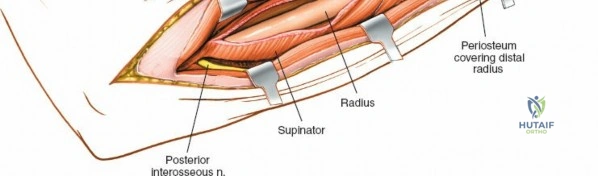
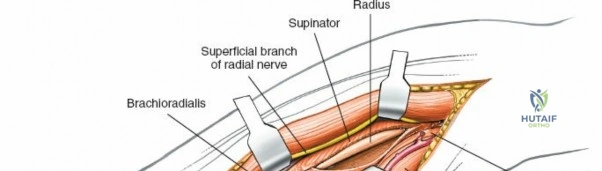
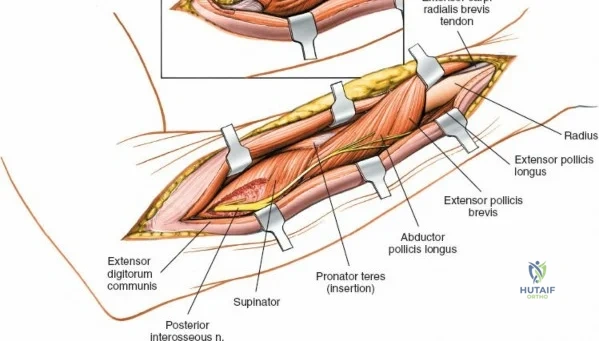
The proximal radius is draped by the supinator muscle. The PIN passes directly through the belly of the supinator. To protect the nerve, the forearm must be fully supinated. Supination dynamically rotates the radius, carrying the insertion of the supinator anteriorly and simultaneously displacing the PIN laterally and posteriorly, safely away from the surgical field.
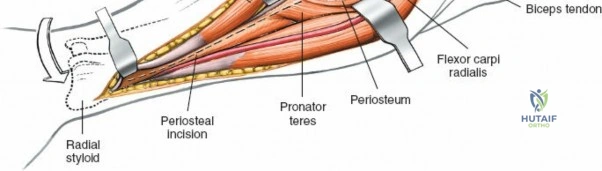
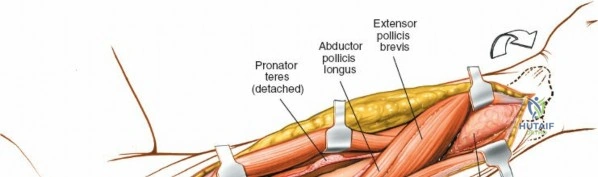
With the forearm fully supinated, identify the broad insertion of the supinator on the anterior aspect of the radius. Incise the supinator directly along the line of its insertion onto the bone. It is critical to detach the muscle by dividing its insertion sharply at the bone, rather than splitting the muscle belly, which would risk cutting the PIN.

Proceed with strict subperiosteal dissection, elevating the supinator laterally off the bone. This is one of the rare instances in orthopedic surgery where the safety gained by staying in a subperiosteal plane completely outweighs the theoretical vascular damage to the bone caused by periosteal stripping. The elevated supinator muscle belly now acts as a protective cushion for the PIN.

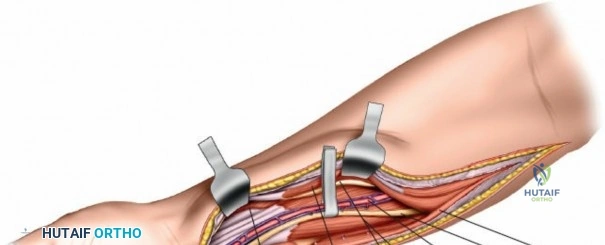
Retractor Placement and Fixation Technique
Once the proximal radius is exposed, great care must be taken with retractor placement. Never place Hohmann or levering retractors blindly around the posterior surface of the radial neck. Because the PIN may touch the bone posteriorly in up to 25% of patients, a posteriorly placed retractor can easily crush the nerve against the radial cortex. Instead, use gentle right-angle retractors or place retractors only on the anterior and lateral aspects of the bone, utilizing the elevated supinator as a shield.
For fracture fixation, a dynamic compression plate or locking compression plate is applied to the volar surface of the radius. The volar surface provides a flat, mechanically advantageous surface for plating and allows for excellent soft tissue coverage by the overlying muscle bellies upon closure. Ensure that the natural radial bow is meticulously restored during reduction to guarantee full postoperative pronation and supination.
Complications, Incidence Rates, and Salvage Management
Surgical approaches to the upper third of the radius are fraught with potential complications. A thorough understanding of these risks, their
Clinical & Radiographic Imaging Archive