Total Shoulder Arthroplasty: When Glenohumeral OA Needs Surgery
Key Takeaway
Discover the latest medical recommendations for Total Shoulder Arthroplasty: When Glenohumeral OA Needs Surgery. Total shoulder arthroplasty (TSA) is an operative treatment addressing chronic shoulder pain and disability. It is recommended when conservative measures, including pain medication, physical therapy, and corticosteroid injections, fail to provide lasting relief. Preoperative planning often involves CT scans to assess glenoid bone stock and version for optimal component placement.
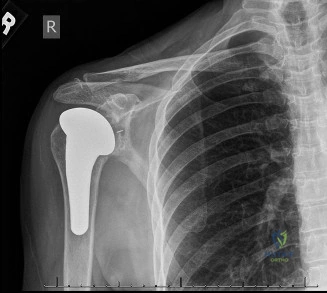
A 68-year-old retired manual labourer presents with a 2-year history of progressive shoulder pain. He struggles to reach his back pocket and has difficulty sleeping on the affected side. On examination, he has globally restricted range of motion, and you elicit crepitus on passive movement. This is his AP radiograph.
What is your differential diagnosis, and what specific clinical features are you looking for to guide your surgical planning?
Candidate: The most likely diagnosis is primary glenohumeral osteoarthritis. Differentials would include cuff tear arthropathy, avascular necrosis, or inflammatory arthropathy. I would look for an intact rotator cuff, which is essential for an anatomic TSA. I’d also assess the range of motion, specifically internal rotation, and check for deltoid function.
Focusing only on the "bone" findings. Candidates often forget to emphasize the rotator cuff status. Mentioning "arthritis" without classifying the glenoid morphology (Walch) or failing to explicitly mention that the rotator cuff MUST be intact for an anatomic shoulder replacement is a significant oversight.
The candidate should immediately classify the clinical picture: Primary OA vs. Secondary (e.g., AVN, CTA, inflammatory). Key examination points: 1) Rotator cuff integrity (clinically testing lag signs/strength); 2) Deltoid function (must be intact); 3) Capsular contracture (especially subscapularis shortening). They must mention that surgical planning requires CT scanning to evaluate Walch glenoid morphology (A/B/C/D) to determine if a standard, augmented, or reverse construct is required.
You have decided to proceed with an anatomic Total Shoulder Arthroplasty. You are now in the theatre. Describe your approach to the anterior soft tissues and the specific precautions you take regarding the neurovascular structures identified here.

Candidate: I use the deltopectoral approach. I identify the cephalic vein in the groove. I release the clavipectoral fascia. The main concern is the axillary nerve during the inferior capsular release, as it sits close to the capsule at the inferior glenoid neck. I also need to be careful with the musculocutaneous nerve medially if I am performing extensive releases.
Failing to mention the "Three Sisters" (anterior circumflex humeral vessels). A high-scoring candidate will mention identifying and ligating these to maintain a bloodless field and using them as a landmark to protect the axillary nerve.
The candidate structures the response: 1) Approach (deltopectoral, cephalic vein management). 2) Subscapularis management (Tenotomy vs. Peel vs. Lesser Tuberosity Osteotomy). 3) Neurovascular safety: Explicitly stating that the axillary nerve is at risk during inferior capsular release and the musculocutaneous nerve is at risk if medial retraction is excessive. 4) The anterior circumflex humeral vessels must be ligated as they mark the superior border of the axillary nerve.
Post-operatively, the patient presents at 6 weeks with concerns about stiffness. You are worried about the glenoid component. What radiographic findings would raise your suspicion for early failure, and what do you know about the microbiology of "stiff" shoulder replacements?

Candidate: Radiographically, I would look for lucent lines around the glenoid component, which suggests aseptic loosening. Regarding stiffness, I am very concerned about low-grade infection, particularly Cutibacterium acnes. It is an indolent, anaerobic organism that often presents without constitutional symptoms but causes stiffness and pain. I would need to keep tissue cultures for at least 14 days.
Ignoring the "stiffness" clue as purely physiological. Candidates must correlate persistent stiffness with occult infection. Failing to mention the specific incubation time for C. acnes (14 days) is a common failure point.
The candidate must articulate: 1) Radiographic signs of loosening: Radiolucent lines >2mm, component migration, or "rocking horse" glenoid. 2) Infection: *C. acnes* is the primary pathogen. 3) Diagnostic strategy: Multiple deep tissue biopsies, holding cultures for 14 days. 4) Management: Differentiating between aseptic loosening (revision) and septic loosening (two-stage revision with antibiotic-impregnated spacers).
