Distal Ulnar Resection Arthroplasty (Darrach Procedure): An Intraoperative Masterclass

Key Takeaway
Welcome, fellows, to an immersive masterclass on the Darrach procedure, a vital technique for distal radioulnar joint arthrosis. We'll meticulously cover surgical anatomy, patient positioning, and the granular, real-time execution of the procedure. Expect detailed insights into incision, dissection, and osteotomy, alongside crucial pearls, potential pitfalls, and comprehensive postoperative management to ensure optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
The distal radioulnar joint (DRUJ) is a remarkably complex articulation that serves as the foundation for forearm rotation and load transmission across the wrist. When conservative measures fail to alleviate the debilitating pain and functional deficits associated with DRUJ pathology, surgical intervention becomes necessary. The distal ulnar resection arthroplasty, universally known as the Darrach procedure, was first described by Dr. William Darrach in 1912 for the treatment of an unreduced volar dislocation of the distal ulna. Over a century later, this operation remains a cornerstone in the orthopedic surgeon's armamentarium. While the advent of alternative techniques—such as Bowers’ hemiresection-interposition technique (HIT), Watson’s matched resection, the Sauvé-Kapandji procedure, and modern implant arthroplasty—has narrowed its universal application, the Darrach procedure maintains a vital, undisputed role in specific patient populations.
Historically, the Darrach procedure was applied liberally to almost any painful condition of the DRUJ, leading to a recognized cohort of patients suffering from postoperative instability and radioulnar convergence. Modern patho-epidemiology dictates a much more refined application. Today, the classic indication is primarily found in the context of inflammatory arthropathies, most notably rheumatoid arthritis (RA). In the rheumatoid wrist, synovial hypertrophy leads to attritional destruction of the triangular fibrocartilage complex (TFCC) and the secondary capsuloligamentous stabilizers, culminating in the classic caput ulnae syndrome. Here, the Darrach procedure, often combined with a radiolunate arthrodesis or total wrist arthroplasty, effectively eliminates pain and restores a functional arc of motion.
Beyond inflammatory conditions, the patho-epidemiology encompasses post-traumatic osteoarthritis, severe distal radius fracture malunions, and primary osteoarthritis. In the setting of a distal radius malunion, particularly those with severe radial shortening and dorsal angulation, the biomechanical relationship of the DRUJ is profoundly altered. The ulna becomes relatively positive, leading to ulnocarpal impaction and incongruity at the sigmoid notch. When such deformities occur in low-demand, elderly patients where a corrective osteotomy of the radius is deemed excessively morbid or biologically unfavorable, a Darrach resection provides an elegant, definitive salvage solution.
The fundamental biomechanical consequence of any DRUJ pathology is the alteration of load transfer. In a healthy wrist, approximately 20% of the axial load is transmitted through the ulnocarpal axis. When the DRUJ is arthritic or unstable, this load transmission becomes exquisitely painful. The goal of the Darrach procedure is to completely ablate this painful articulation. However, the surgeon must possess a profound understanding of the resulting biomechanical void. By excising the ulnar head, the surgeon removes the osseous fulcrum of the forearm, shifting the entirety of the axial and rotational load-bearing responsibilities to the radius and the remaining interosseous membrane. Understanding this shift is paramount to patient selection and operative success.
Detailed Surgical Anatomy and Biomechanics
Mastery of the Darrach procedure demands an intimate understanding of the osseous architecture and the intricate soft-tissue envelope of the distal forearm. The DRUJ is a diarthrodial, trochoid joint comprising the convex head of the ulna and the concave sigmoid notch of the radius. The sigmoid notch is located on the medial aspect of the distal radius, possessing an arc of curvature that typically ranges between 47 and 80 degrees, with an average radius of 12 to 18 millimeters. Conversely, the articular cartilage-covered "cap" of the distal ulna features a "seat" with an arc of curvature ranging between 90 and 135 degrees and an average radius of 8 to 13 millimeters. This inherent mismatch in the radii of curvature dictates that the DRUJ is not a highly constrained ball-and-socket joint, but rather a loosely constrained articulation that relies heavily on soft tissues for stability.
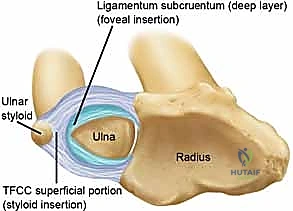
The primary stabilizer of the DRUJ is the Triangular Fibrocartilage Complex (TFCC). For the operating surgeon, the critical anatomical distinction lies within the ulnar attachments of the TFCC. The superficial layer attaches to the tip and side of the ulnar styloid, while the deep layer—the ligamentum subcruentum—attaches to the fovea at the base of the ulnar styloid. The foveal attachment is the true isometric center of rotation and the primary restraint to dorsal-palmar translation. Furthermore, the volar and dorsal radioulnar ligaments form the thickened margins of the TFCC, providing critical stability at the extremes of pronation and supination. When performing a Darrach resection, the surgeon inherently detaches the radius from the ulna, destroying these ligamentous connections.
Kinematically, the DRUJ allows for approximately 150 degrees of forearm rotation. During this arc of motion, the radius rotates around the relatively stationary ulna. Because of the differing arcs of curvature between the sigmoid notch and the ulnar head, there is an obligatory proximal-distal migration and dorsal-palmar translation of the ulna relative to the radius. The interosseous membrane (IOM), specifically its distal oblique bundle (DOB), acts as a secondary stabilizer. Following a Darrach resection, the integrity of the IOM becomes the primary defense against radioulnar convergence. If the IOM is attenuated or if the resection is carried too proximally, the dynamic forces of the pronator quadratus and the brachioradialis will draw the distal radial stump into the resected ulna, causing debilitating impingement.

Neurovascular and muscular topography dictates our surgical approach. The dorsal sensory branch of the ulnar nerve (DSUN) is the structure at highest risk during the superficial dissection. It emerges from beneath the flexor carpi ulnaris (FCU) approximately 5 to 8 centimeters proximal to the pisiform, traveling dorsally and distally to innervate the ulnar aspect of the dorsum of the hand. Deep to the subcutaneous tissues, the extensor retinaculum defines the muscular intervals. The standard approach utilizes the interval of the fifth extensor compartment, housing the extensor digiti minimi (EDM). The surgeon must meticulously preserve the sixth dorsal compartment, specifically the linea jugata—the fibro-osseous tunnel stabilizing the extensor carpi ulnaris (ECU). Disruption of the ECU subsheath leads to chronic, painful snapping and subluxation of the tendon over the ulnar stump.

Exhaustive Indications and Contraindications
The decision to proceed with a Darrach procedure requires a rigorous assessment of the patient's physiological demands, the specific etiology of the DRUJ pathology, and the integrity of the surrounding wrist structures. The classic, most universally accepted indication is advanced rheumatoid arthritis with severe destruction of the DRUJ, often presenting as caput ulnae syndrome. In these patients, the ulnar head is frequently subluxated dorsally, the TFCC is incompetent, and the extensor tendons are at severe risk of attritional rupture. A distal ulnar resection in this cohort not only relieves pain but also serves as a critical prophylactic measure against extensor tendon rupture.

Beyond inflammatory arthropathy, the Darrach is indicated in low-demand, elderly patients suffering from post-traumatic osteoarthritis or severe, symptomatic malunions of the distal radius. In cases where a distal radius fracture heals with profound shortening and dorsal tilt, the resulting DRUJ incongruity and ulnocarpal impaction can be devastating. If the patient's physiological age or comorbidities preclude a complex corrective osteotomy of the radius, a Darrach resection offers a reliable, single-stage salvage. Furthermore, it serves as a fallback for failed previous DRUJ interventions, such as a failed Bowers hemiresection or a non-uniting Sauvé-Kapandji procedure, provided the patient understands the postoperative lifting restrictions.

Contraindications are equally vital to master, as inappropriate application of the Darrach procedure guarantees catastrophic failure. The absolute contraindication is a young, high-demand patient, particularly heavy laborers or athletes. These individuals require the osseous buttress of the ulnar head to support the immense compressive and rotational forces transmitted across the wrist during power grip and lifting. Resecting the distal ulna in a 30-year-old manual laborer will inevitably lead to painful radioulnar convergence and profound grip weakness. Additionally, the Darrach is contraindicated in the presence of longitudinal radioulnar instability, such as an Essex-Lopresti injury (radial head fracture combined with IOM rupture). Without the radial head and IOM, resecting the distal ulna removes the final restraint to proximal migration of the radius, leading to ulnocarpal impingement and elbow pain.
Pre-existing ulnar translation of the carpus is a relative contraindication, particularly in the rheumatoid patient. The ulnar head provides a critical buttress preventing the carpus from sliding down the ulnar slope of the distal radius. If this translation is already present, a Darrach will accelerate the deformity unless combined with a radiolunate arthrodesis.
Clinical Decision Matrix: Darrach Procedure
| Parameter | Favorable Indication for Darrach | Contraindication for Darrach |
|---|---|---|
| Patient Age/Demand | Elderly, low-demand, sedentary | Young, heavy laborers, athletes |
| Underlying Pathology | Rheumatoid Arthritis, severe OA | Isolated TFCC tear, mild instability |
| IOM Integrity | Intact interosseous membrane | Essex-Lopresti injury (torn IOM) |
| Carpal Alignment | Well-aligned carpus over radius | Severe ulnar translation of the carpus |
| Previous Surgery | Failed alternative arthroplasty | Salvageable by ulnar shortening |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative evaluation dictates the technical execution of the surgery. The clinical examination must differentiate isolated DRUJ pathology from concomitant ulnocarpal or radiocarpal issues. The surgeon should assess for the "foveal sign"—tenderness in the soft spot between the ulnar styloid and the FCU tendon—which indicates TFCC pathology. The "piano key maneuver" is essential: the examiner stabilizes the radius and attempts to ballot the distal ulna dorsally and volarly. Visible dorsal winging that reduces with pressure but spontaneously subluxates upon release confirms a loss of structural support. Grip strength should be measured dynamically; a significant drop in grip strength when the forearm is fully pronated compared to neutral often highlights DRUJ instability and arthrosis.

Imaging requires strict adherence to standardized protocols. Standard posteroanterior (PA) and lateral radiographs are insufficient if not properly controlled for rotation. The surgeon must demand a "zero-rotation view." This is obtained with the patient’s shoulder abducted 90 degrees, the elbow flexed 90 degrees, and the wrist in neutral rotation (PA position). In this true lateral of the wrist, the ulnar styloid is seen in full profile. This view is mandatory to accurately assess ulnar variance, the morphology of the sigmoid notch, and the degree of dorsal or volar subluxation of the ulnar head. Advanced imaging, such as thin-cut Computed Tomography (CT), is invaluable for assessing the 3D architecture of distal radius malunions and the exact degree of sigmoid notch arthritis. Magnetic Resonance Imaging (MRI) is rarely needed for the osseous resection itself but is critical if soft-tissue pathology (like an ECU tendon tear) is suspected.
Templating the resection is the most critical preoperative step. The dogma of "more is better" is entirely fallacious in DRUJ resection. The goal is a minimal resection—removing just enough bone to clear the sigmoid notch and prevent impingement during rotation, but leaving as much ulnar shaft as possible to preserve the attachments of the pronator quadratus and the distal interosseous membrane. Typically, this equates to 10 to 20 millimeters of bone resection measured from the ulnar articular surface. Templating on the zero-rotation PA radiograph allows the surgeon to mark the exact level of the proximal margin of the sigmoid notch, which serves as the distal-most acceptable level of the ulnar cut.
Patient positioning is standardized but requires attention to detail. The patient is placed supine with the operative arm extended on a radiolucent hand table. A well-padded upper arm tourniquet is applied. Regional anesthesia (supraclavicular or axillary block) is preferred, as it provides excellent intraoperative muscle relaxation and prolonged postoperative analgesia, facilitating early mobilization. The arm is prepped and draped in a standard sterile fashion, ensuring the elbow is free to allow full assessment of forearm pronation and supination intraoperatively. A mini C-arm fluoroscopy unit should be draped and positioned perpendicular to the hand table, ready to confirm the level of the osteotomy before the final cut is made.
Step-by-Step Surgical Approach and Fixation Technique
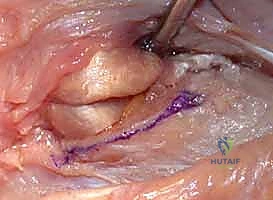
The operation begins with a 5 to 6-centimeter longitudinal incision over the dorsal aspect of the distal ulna, centered directly over the ulnar head. The incision is carried through the skin and subcutaneous tissue with meticulous hemostasis. The surgeon must remain acutely aware of the dorsal sensory branch of the ulnar nerve (DSUN). Blunt dissection with spreading scissors is utilized in the subcutaneous fat to identify and protect the longitudinal venous structures and the branching network of the DSUN, retracting them gently with vessel loops.

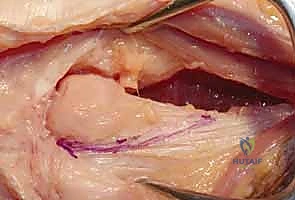
Once the extensor retinaculum is exposed, the anatomical intervals must be respected. The deep fascia is incised in line with the skin incision over the fifth extensor compartment, which houses the extensor digiti minimi (EDM). The EDM is mobilized and retracted radially. This exposes the dorsal capsule of the DRUJ. It is absolutely critical to avoid violating the sixth extensor compartment. The ECU subsheath and the linea jugata must remain pristine; iatrogenic destabilization of the ECU is a frequent cause of postoperative failure and chronic ulnar-sided pain.

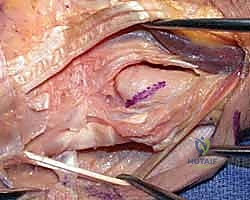
The dorsal capsule of the DRUJ is incised longitudinally, creating a radially based flap that will be utilized later for soft-tissue interposition or capsular plication. Subperiosteal dissection is then carried out around the neck of the ulna. Curved Hohmann retractors are carefully passed volarly and dorsally around the ulnar neck to protect the volar structures, specifically the ulnar neurovascular bundle and the flexor tendons. The level of the osteotomy is confirmed with fluoroscopy. The cut should be made just proximal to the sigmoid notch. Using a microsagittal saw under constant saline irrigation to prevent thermal necrosis, the osteotomy is performed.

The osteotomy cut should not be purely transverse. It is best performed with a slight oblique angle, sloping from proximal-ulnar to distal-radial, or by meticulously rounding the edges of the remaining ulnar stump with a rongeur and rasp. This prevents a sharp cortical edge from impinging on the radius during pronation. Once the cut is complete, the ulnar head is grasped with a towel clip or tenaculum. Sharp dissection is required to detach the remaining capsular and TFCC attachments from the ulnar styloid and fovea, allowing the head to be delivered from the wound.
The final, and arguably most crucial, step is soft-tissue stabilization of the ulnar stump. The empty space left by the resected head allows the distal ulna to translate dynamically. To mitigate this, the dorsal capsular flap is brought over the raw cancellous surface of the ulnar stump and sutured to the volar capsule or the TFCC remnants. If the stump exhibits excessive dorsal instability (the "window wiper" effect), a stabilizing tenodesis is required. This is frequently achieved by taking a distally based slip of the ECU tendon, passing it through a drill hole in the distal ulnar stump, and suturing it back onto itself under tension. Alternatively, the pronator quadratus can be mobilized and interposed between the radius and ulna. The extensor retinaculum is then repaired over the EDM, ensuring the ECU remains securely in its groove, and the skin is closed in layers.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, the Darrach procedure carries a known complication profile, primarily stemming from the unavoidable biomechanical alterations of excising the ulnar load-bearing column. The most notorious and functionally devastating complication is radioulnar convergence, also known as radioulnar impingement. This occurs when the dynamic forces of the forearm musculature—specifically the pronator quadratus, brachioradialis, and the interosseous membrane—pull the radius and the resected ulnar stump together during grip and rotation. Without the ulnar head to act as a spacer, the distal radius impacts the ulnar stump, causing severe, deep aching pain.

Ulnar stump instability is another frequent complication, presenting as the "window wiper" effect. The resected end of the ulna subluxates dorsally and volarly during forearm rotation. This instability is highly symptomatic, causing a visible and painful clunk as the stump snaps against the overlying extensor tendons. Furthermore, if the ECU subsheath was violated during the approach, the ECU tendon itself may subluxate volarly during supination, exacerbating the ulnar-sided wrist pain and leading to attritional tendinopathy. In
Clinical & Radiographic Imaging Archive