Dorsal Cheilectomy for Hallux Rigidus: An Intraoperative Masterclass

Key Takeaway
Join us in the OR for a dorsal cheilectomy masterclass. We'll meticulously cover patient selection, detailed surgical anatomy, precise intraoperative techniques for osteophyte resection and joint debridement, and essential pearls to avoid complications. Learn critical steps from incision to closure, ensuring optimal outcomes for hallux rigidus patients. Postoperative rehabilitation and complication management are also thoroughly discussed.
Comprehensive Introduction and Patho-Epidemiology
Defining the Pathologic Entity
Hallux rigidus represents a progressive, debilitating, and highly prevalent degenerative arthropathy of the first metatarsophalangeal (MTP) joint. Distinct from a simple loss of flexibility, this condition is characterized by a predictable pattern of articular cartilage degradation, subchondral sclerosis, and the robust formation of periarticular osteophytes. The cardinal clinical hallmark is a marked restriction in sagittal plane kinematics, specifically limited dorsiflexion, which profoundly disrupts the normal propulsive phase of the human gait cycle. The term "hallux rigidus," originally coined by Cotterill in 1887, accurately describes the end-stage manifestation of the disease, though "hallux limitus" is often utilized to describe earlier stages where varying degrees of motion are preserved but painful.
Epidemiological Landscape
Epidemiologically, hallux rigidus is the most common osteoarthritic condition affecting the foot and ankle, and the second most common pathology of the first ray, superseded only by hallux valgus. It primarily afflicts adults in their fourth to sixth decades of life, though a distinct cohort of younger patients can present with the condition, often secondary to acute trauma, osteochondritis dissecans, or profound biomechanical anomalies. Bilateral involvement is observed in nearly 80% of patients, suggesting a strong intrinsic or genetic predisposition to the underlying pathomechanics. The condition exhibits a slight female predilection, though this disparity is significantly less pronounced than that seen in hallux valgus deformity.
Pathogenesis and Biomechanical Considerations
The core pathomechanical issue in hallux rigidus is the development of reactive dorsal and marginal osteophytes. This osteophytosis is generally the sequela of chronic, repetitive microtrauma, altered joint kinematics, inflammatory reactions, or direct chondral injury. A primary driver is thought to be an elevated first metatarsal (metatarsus primus elevatus), which forces the proximal phalanx into a relatively plantarflexed position, causing dorsal impingement during the propulsive toe-off phase of gait. If these abnormal shear and compressive stresses persist, the condition inexorably progresses from focal dorsal impingement to global, end-stage arthritic obliteration of the joint space. Initially, the limitation is predominantly in dorsiflexion due to the mechanical block created by the dorsal exostosis. While plantarflexion is typically preserved in the early stages, progressive capsular contracture and circumferential osteophyte formation will eventually restrict all planes of motion.
The Role of Dorsal Cheilectomy
The Dorsal Cheilectomy remains the gold-standard joint-sparing surgical intervention for mild to moderate hallux rigidus (Coughlin and Shurnas Grades 1 and 2, and select Grade 3 cases). The nomenclature derives from the Greek cheilos (lip) and ectomy (excision). The primary objective of this procedure is to meticulously resect the impinging dorsal osteophytes of the metatarsal head and proximal phalanx, alongside a portion of the dorsal articular surface, thereby alleviating the mechanical block to dorsiflexion. By decompressing the joint and removing the source of impingement, the surgeon aims to restore functional, pain-free range of motion, effectively delaying or entirely circumventing the need for a definitive arthrodesis or arthroplasty.
Detailed Surgical Anatomy and Biomechanics
Osteology and Articular Geometry
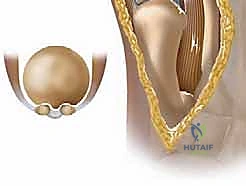
A profound understanding of the first MTP joint anatomy is non-negotiable for executing a successful cheilectomy. The joint is a complex hinge-type (ginglymus) synovial articulation. The first metatarsal head is unique; its articular surface extends further plantarly than dorsally, accommodating the sesamoid complex and facilitating the windlass mechanism. The dorsal aspect of the metatarsal head is the epicenter for our primary resection. The base of the proximal phalanx, which articulates with the metatarsal head, also frequently develops a dorsal osteophytic rim that must be addressed to prevent reciprocal impingement. The geometry of the joint dictates that even a minor dorsal prominence can severely restrict the rolling and gliding motion required for terminal dorsiflexion.
Ligamentous and Capsular Stabilizers
The stability of the first MTP joint relies heavily on its robust capsuloligamentous envelope. The collateral ligaments are the primary restraints to varus and valgus stress. They originate from the medial and lateral epicondyles of the metatarsal head and fan out to insert on the proximal phalanx (proper collateral ligament) and the plantar plate/sesamoid complex (accessory collateral ligament). During a dorsal cheilectomy, the surgeon must meticulously elevate the dorsal capsule while rigorously preserving the integrity of these collateral ligaments. Iatrogenic transection or over-resection of the metatarsal head that compromises the epicondylar origins will lead to catastrophic multiplanar instability. The dorsal capsule itself is a fibrous layer that becomes thickened and contracted in hallux rigidus, requiring thorough release.
Musculotendinous Dynamics
The dynamic stabilizers of the first ray must be respected during the surgical approach. The Extensor Hallucis Longus (EHL) tendon courses centrally over the dorsal aspect of the joint, tethered within the extensor hood, and inserts onto the distal phalanx. It is the primary dorsiflexor of the hallux. The standard surgical incision is placed just medial to the EHL tendon to avoid adherence to the scar. Deep to the EHL lies the Extensor Hallucis Brevis (EHB), which inserts onto the dorsal base of the proximal phalanx. Plantarly, the intrinsic muscles (Flexor Hallucis Brevis) and the extrinsic Flexor Hallucis Longus (FHL) tendon provide powerful plantarflexion, countering the dorsal forces and stabilizing the proximal phalanx against the metatarsal head during weight-bearing.
Neurovascular Anatomy and the Sesamoid Complex
The neurovascular anatomy dictates our superficial dissection. The dorsomedial cutaneous nerve, a terminal branch of the superficial peroneal nerve, frequently crosses the surgical field obliquely. Injury to this nerve results in painful neuromas or debilitating paresthesias along the dorsomedial hallux. Meticulous blunt dissection and gentle retraction are imperative. The plantar aspect of the joint houses the sesamoid complex—medial (tibial) and lateral (fibular) sesamoids embedded within the FHB tendons. This complex articulates with the plantar metatarsal head, acting as a critical fulcrum that enhances the mechanical advantage of the FHL. While not directly visualized during a standard dorsal cheilectomy, underlying sesamoid pathology must be ruled out preoperatively, as it can mimic or exacerbate MTP joint pain.
Exhaustive Indications and Contraindications
Clinical Evaluation and Decision Making
The decision to proceed with a dorsal cheilectomy hinges on a meticulous correlation of patient history, physical examination, and radiographic findings. The ideal candidate presents with pain primarily elicited at the extremes of dorsiflexion, a clear indicator of dorsal impingement. Pain localized to the dorsal aspect of the joint, often accompanied by a palpable dorsal prominence (the "dorsal bunion"), is classic. Conversely, pain throughout the entire arc of motion, or severe pain with plantarflexion, suggests more advanced, global arthrosis. The physical examination must quantify sagittal range of motion (ROM). A critical maneuver is the "grind test"—axial compression combined with rotation of the proximal phalanx against the metatarsal head. A strongly positive grind test indicates significant central cartilage loss and is a relative contraindication to joint-sparing surgery.
Non-Operative Optimization
Surgical intervention is strictly reserved for patients who have failed a comprehensive regimen of non-operative management. This conservative phase should include the judicious use of NSAIDs for inflammatory control, and the implementation of rigid-soled shoes or carbon fiber inserts to limit sagittal plane excursion of the MTP joint. Accommodative orthotics featuring a Morton's extension can effectively transfer stress away from the first ray. Intra-articular corticosteroid injections may provide diagnostic confirmation and temporary therapeutic relief, particularly in cases with acute inflammatory flares. Only when these modalities fail to provide acceptable functional relief should cheilectomy be entertained.
Establishing Surgical Candidacy
Indications for cheilectomy are generally confined to Coughlin and Shurnas Grades 1 and 2, characterized by mild to moderate dorsal osteophytosis, preservation of the joint space on the plantar half of the articulation, and pain primarily at terminal dorsiflexion. In highly selected Grade 3 cases, where the patient exhibits a relatively well-preserved plantar joint space and refuses arthrodesis, a cheilectomy may be offered as a temporizing measure, provided the patient is extensively counseled on the high likelihood of eventual progression to fusion.
Absolute and Relative Contraindications
Contraindications must be strictly observed to prevent disastrous clinical outcomes. Advanced hallux rigidus (Grade 4) with complete obliteration of the joint space, global crepitus, and a profoundly positive grind test is an absolute contraindication; these patients require an arthrodesis. Inflammatory arthropathies (e.g., rheumatoid arthritis) are generally contraindications for cheilectomy due to the systemic nature of the cartilage destruction and poor capsular tissue quality. Significant concurrent hallux valgus deformity is a relative contraindication, as a simple cheilectomy will not address the multiplanar instability and may exacerbate the valgus drift.
| Parameter | Indications for Dorsal Cheilectomy | Contraindications for Dorsal Cheilectomy |
|---|---|---|
| Clinical Grade | Coughlin & Shurnas Grade 1, Grade 2, select Grade 3 | Coughlin & Shurnas Grade 4 (Global Arthrosis) |
| Pain Profile | Pain primarily at extreme dorsiflexion | Pain throughout entire ROM; severe rest pain |
| Grind Test | Negative or mildly positive | Strongly positive (indicates central cartilage loss) |
| Radiographic | Dorsal osteophytes; preserved plantar joint space | Complete joint space obliteration; cystic changes |
| Systemic Disease | Primary osteoarthritis; post-traumatic (focal) | Inflammatory arthropathy (Rheumatoid, advanced Gout) |
| Deformity | Isolated sagittal plane pathology | Severe concomitant Hallux Valgus or multiplanar instability |
Pre-Operative Planning, Templating, and Patient Positioning
Standardized Radiographic Assessment
Comprehensive radiographic evaluation is the cornerstone of preoperative planning. Standard weight-bearing Anteroposterior (AP), Lateral, and Oblique views of the foot are mandatory. The AP radiograph is scrutinized for the presence of medial and lateral osteophytes, joint space narrowing, and any subtle hallux valgus or interphalangeus deformities. It is critical to recognize that dorsal osteophytes can superimpose over the joint space on an AP view, falsely suggesting complete joint obliteration.


The weight-bearing Lateral radiograph is the most critical view for templating a cheilectomy. It allows for the precise quantification of the dorsal osteophyte on both the metatarsal head and the proximal phalanx. Furthermore, it facilitates the assessment of metatarsus primus elevatus, which may necessitate concurrent proximal corrective procedures if severe.


Advanced Imaging Modalities
An Axial Sesamoid view should be routinely obtained to evaluate the integrity of the sesamoid complex, ruling out bipartite sesamoids, sesamoiditis, or frank arthrosis of the metatarsosesamoid articulation, which could compromise the post-operative outcome.


While Magnetic Resonance Imaging (MRI) is not a routine prerequisite for diagnosing hallux rigidus, it becomes an invaluable tool when the clinical pain is disproportionate to the radiographic findings. MRI is highly sensitive for detecting occult osteochondral lesions of the metatarsal head, early subchondral cystic changes, or profound marrow edema, which might pivot the surgical decision away from a simple cheilectomy toward an osteochondral grafting procedure or arthrodesis.
Pre-Operative Templating and Adjunct Planning
Templating involves estimating the volume of bone to be resected. The standard goal is to resect the dorsal 20% to 30% of the metatarsal head. Resecting more than 30% significantly increases the risk of destabilizing the joint by violating the collateral ligament origins. The surgeon must also plan for a potential Moberg osteotomy (a dorsal closing-wedge osteotomy of the base of the proximal phalanx). This is templated if the anticipated cheilectomy alone is unlikely to yield the desired 60-70 degrees of intraoperative dorsiflexion, particularly in patients with a long proximal phalanx or severe baseline stiffness.
Patient Positioning and Anesthesia
The procedure is typically performed on an outpatient basis. The patient is positioned supine on the operating table. A small bump may be placed under the ipsilateral hip to internally rotate the leg slightly, bringing the medial aspect of the foot into a directly superior, easily accessible orientation. Anesthesia is usually achieved via a regional ankle block (targeting the tibial, deep peroneal, superficial peroneal, saphenous, and sural nerves) combined with monitored anesthesia care (MAC) or light general anesthesia. A pneumatic tourniquet is applied either at the thigh or the calf, depending on surgeon preference, and inflated after exsanguination to ensure a bloodless surgical field, which is critical for identifying delicate neurovascular structures.
Step-by-Step Surgical Approach and Fixation Technique
Incision and Superficial Dissection
The surgical approach begins with a 4 to 5 cm longitudinal incision centered over the dorsomedial aspect of the first MTP joint. The incision extends from the mid-shaft of the first metatarsal to the mid-shaft of the proximal phalanx. The placement is deliberately medial to the Extensor Hallucis Longus (EHL) tendon to prevent postoperative tendon adhesions to the cutaneous scar.

Following skin incision, sharp dissection is minimized. Blunt dissection using tenotomy scissors is employed to identify and mobilize the superficial venous plexus and, crucially, the dorsomedial cutaneous branch of the superficial peroneal nerve. This nerve must be meticulously isolated and gently retracted medially or laterally, out of harm's way. The EHL tendon is identified within its sheath and retracted laterally using a Senn or Ragnell retractor.
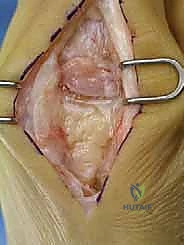

Capsulotomy and Joint Exposure
Once the extensor hood is visualized, a longitudinal capsulotomy is performed directly in line with the skin incision. The capsule and periosteum are then elevated off the dorsal aspect of the first metatarsal head and the base of the proximal phalanx using a sharp periosteal elevator (e.g., a Freer or Key elevator). This subperiosteal dissection must be meticulous to expose the entire dorsal osteophyte.
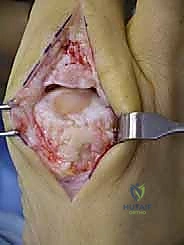

It is imperative to sweep the capsule medially and laterally just enough to expose the margins of the osteophyte, but the surgeon must absolutely avoid stripping the collateral ligaments from their epicondylar origins on the medial and lateral aspects of the metatarsal head. At this stage, the joint is plantarflexed to assess the extent of central cartilage wear and confirm the preoperative decision to proceed with joint preservation.


The Cheilectomy Resection
The actual cheilectomy is performed using a sagittal saw or a sharp, broad osteotome. The cut is initiated dorsally, just proximal to the osteophyte on the metatarsal neck, and directed distally and slightly plantarly to exit at the dorsal margin of the preserved articular cartilage. The rule of thumb is to resect approximately 20% to 30% of the dorsal metatarsal head.


Following the primary resection, a rongeur or rasp is utilized to smooth the remaining bony edges, ensuring no sharp prominences remain that could irritate the dorsal capsule or EHL tendon. Attention is then turned to the proximal phalanx. Any corresponding dorsal osteophytic lip on the phalangeal base is meticulously resected with a rongeur to prevent reciprocal impingement.


The joint is thoroughly irrigated with sterile saline to remove all bone debris. The surgeon then assesses the range of motion. The goal is to achieve at least 60 to 70 degrees of passive dorsiflexion without impingement or bony block.

Adjunctive Moberg Osteotomy and Closure
If, after adequate cheilectomy and capsular release, the dorsiflexion remains inadequate (typically less than 40-50 degrees), a Moberg osteotomy is indicated. This involves a dorsal closing-wedge osteotomy at the base of the proximal phalanx, approximately 1 cm distal to the joint line. The wedge is removed, the osteotomy is closed (effectively dorsiflexing the hallux), and it is rigidly fixed using a single small headless compression screw, a staple, or crossing K-wires. This shifts the arc of motion dorsally without altering the MTP joint mechanics further.


Once optimal motion is achieved and fixation (if utilized) is secure, the wound is closed. The dorsal capsule is reapproximated using an absorbable suture (e.g., 2-0 or 3-0 Vicryl) to prevent EHL subluxation and restore capsular tension. The subcutaneous tissue is closed, followed by a meticulous skin closure using non-absorbable monofilament or a subcuticular stitch. A bulky, compressive soft dressing is applied to control postoperative edema.
Complications, Incidence Rates, and Salvage Management
Neurologic and Soft Tissue Complications
Despite being a highly successful procedure, dorsal cheilectomy carries specific risks. The most frequent immediate complication is injury to the dorsomedial cutaneous nerve. This can range from transient neuropraxia due to traction, to complete transection resulting in a painful stump neuroma. The incidence of nerve-related symptoms is reported to be between 5% and 10%. Management of a painful neuroma initially involves desensitization therapy and gabapentinoids, but recalcitrant cases may require surgical excision and burying of the nerve stump into local muscle or bone. Wound healing issues and superficial infections occur in less than 2% of cases and are generally managed effectively with oral antibiotics and local wound care.
Bony and Biomechanical Failures
Under-resection of the dorsal osteophyte is the most common technical error leading to early clinical failure. If the surgeon is overly conservative and fails to remove an adequate volume of the metatarsal head, persistent dorsal impingement will continue to restrict motion and cause pain. Conversely, over-resection (removing >30% of the metatarsal head) is a catastrophic error. This violates the origins of the collateral ligaments, leading to iatrogenic multiplanar instability, dorsal subluxation
