Distal Radius Malunion Corrective Osteotomy: An Intraoperative Masterclass in Precision and Restoration

Key Takeaway
This masterclass guides you through corrective osteotomy for distal radius malunion. We'll meticulously cover indications, comprehensive surgical anatomy, precise preoperative planning, and detailed intraoperative execution, including specific instrument use and fluoroscopic guidance. Learn critical pearls, pitfalls, and postoperative management, ensuring optimal patient outcomes for complex wrist deformities. Precision and anatomical restoration are paramount in this advanced procedure.
Comprehensive Introduction and Patho-Epidemiology
Welcome, fellows and colleagues, to the operating theater and to this advanced masterclass. Today, we are tackling a challenging, yet incredibly rewarding procedure: a corrective osteotomy for distal radius malunion. This intervention is not merely an exercise in achieving radiographic symmetry; it is a profound endeavor to restore intricate wrist biomechanics, alleviate debilitating pain, and return our patients to their functional independence. The evolution of orthopedic surgery has moved us far beyond the historical acceptance of "functional deformity." Today, the expectation—both ours and our patients'—is the meticulous restoration of native anatomy. This demands rigorous preoperative planning, precise intraoperative execution, and a profound, three-dimensional understanding of wrist osteology and kinematics.
A distal radius malunion is defined not merely by an arbitrary degree of radiographic malalignment, but fundamentally by malalignment associated with significant, measurable dysfunction. This dysfunction typically manifests as an asymmetric loss of motion, diminished grip strength, and persistent, localized pain. Historically, some patients, particularly older, low-demand individuals, were thought to tolerate significant deformity without functional compromise. However, modern clinical evidence strongly refutes this complacency. Many patients desire optimal wrist alignment and function, regardless of chronological age. Our decision-making process must be dictated by physiological demand, bone quality, and specific symptomatology, never by chronological age alone.
The patho-epidemiology of distal radius malunion is deeply intertwined with the initial fracture pattern and the chosen method of primary management. Non-operative management of unstable fracture patterns remains the leading cause of malunion. We must remain vigilant regarding the key risk factors for fracture instability: age over 60 years, initial dorsal angulation exceeding 20 degrees, significant dorsal metaphyseal comminution, comminution extending to the volar metaphyseal cortex, associated ulnar styloid or neck fractures, and displaced intra-articular extensions. When these factors are present, the risk of secondary displacement within a cast approaches unacceptable levels, predisposing the patient to a cascade of biomechanical failures.
The biomechanical consequences of a malunited distal radius are profound and predictable. Normal load transfer across the radiocarpal joint dictates that approximately 80% of axial force is borne by the radius and 20% by the ulna. With progressive dorsal tilt and radial shortening, this ratio shifts dramatically. A dorsal tilt of merely 20 degrees can shift the load-bearing axis dorsally, increasing stress on the radiocarpal ligaments and predisposing the joint to midcarpal instability and early arthrosis. Furthermore, radial shortening leads to relative ulnar lengthening (positive ulnar variance), resulting in ulnocarpal abutment syndrome, characterized by attritional tears of the triangular fibrocartilage complex (TFCC) and chondromalacia of the lunate and ulnar head.




Nascent Versus Mature Malunions
The timing of intervention is a critical conceptual framework. Distal radius osteotomy for a mature malunion usually does not require urgent intervention. Ideally, the patient should have achieved maximal soft tissue equilibrium, demonstrated excellent exercise skills, regained full finger motion, and be free of significant nerve or tendon dysfunction or regional edema. This allows the surgeon to operate in a biologically quiet environment.
However, the concept of the "nascent malunion" fundamentally alters our timeline. For a nascent malunion—typically defined as a healing fracture with unacceptable alignment identified between 6 weeks and 6 months post-injury—intervening earlier takes precedence. In these cases, the fracture is not yet fully consolidated with mature lamellar bone. Early intervention allows us to leverage the existing fracture line, carefully taking down the woven bone callus, and utilizing the hyperemic, osteogenic environment to facilitate rapid healing following realignment. This often negates the need for structural autograft, relying instead on the robust local biology and rigid internal fixation.
Detailed Surgical Anatomy and Biomechanics
Before we make any incision, we must mentally navigate the critical anatomy of the distal forearm and wrist. This region is a highly constrained, complex interplay of osseous architecture, ligamentous stabilizers, tendinous units, and neurovascular structures. Understanding their precise three-dimensional relationships is paramount to safe exposure and effective biomechanical restoration. The distal radius is not merely a block of bone; it is a highly specialized articular platform.
The osteology of the distal radius dictates our reconstructive goals. We are primarily concerned with the distal metaphysis and the articular epiphysis. Key dorsal features include Lister's tubercle, a prominent bony landmark serving as a vital pulley for the Extensor Pollicis Longus (EPL) tendon. This serves as our central dorsal navigational beacon. Volarly, the watershed line represents the most distal margin of the pronator quadratus fossa; hardware placed distal to this line risks catastrophic flexor tendon attrition. The articular surface comprises the lunate and scaphoid facets, separated by the interfacet ridge. Ulnarly, the sigmoid notch forms the concavity that articulates with the ulnar head, forming the Distal Radioulnar Joint (DRUJ), the stability of which is entirely dependent on precise radial anatomy.

Radiographic Parameters and Kinematic Impact
We must rigorously quantify the deformity using standardized radiographic measurements. Dorsal or palmar tilt is measured on a true lateral radiograph as the angle between a line connecting the dorsal and palmar lips of the articular surface and a line perpendicular to the radial shaft. Normal anatomy dictates 11 to 12 degrees of palmar tilt. Ulnarward inclination (often colloquially but incorrectly termed radial inclination) is measured on the PA view, representing the angle between a line connecting the ulnar and radial limits of the articular surface and a line perpendicular to the shaft, normally 22 to 23 degrees.
Ulnar variance is arguably the most critical parameter regarding DRUJ and ulnocarpal kinematics. It is the distance between two lines perpendicular to the radial shaft, one at the ulnar corner of the lunate facet and the other at the distal articular limit of the ulnar head. Positive ulnar variance indicates relative radial shortening, a primary driver of ulnocarpal impaction. Articular incongruity, whether a gap, step-off, or subluxation, must be minimized to less than 2mm to mitigate the risk of post-traumatic osteoarthritis. The loss of these parameters directly alters the instantaneous center of rotation of the wrist, leading to obligate kinematic conflict during pronosupination and flexion-extension arcs.
Soft Tissue Envelopes and Neurovascular Landmines
The dorsal wrist houses six distinct extensor compartments, each critical to identify and protect during a dorsal or combined approach. The first compartment houses the APL and EPB. The second contains the ECRL and ECRB, which are typically retracted radially during dorsal exposure. The third compartment, containing the EPL, is the keystone; this tendon must be mobilized and transposed radially or ulnarly to access the dorsal metaphysis. The fourth compartment (EDC and EIP) is elevated subperiosteally as a single unit to preserve its vascularity and gliding tissue. The fifth (EDM) and sixth (ECU) are critical for ulnar-sided stability.
Neurovascular structures represent significant surgical landmines. The superficial radial nerve (SRN) is a purely sensory nerve running along the radial aspect of the distal forearm, arborizing over the dorsoradial wrist. It is highly vulnerable during skin incision, superficial dissection, and retractor placement. Iatrogenic injury can lead to debilitating, intractable neuromas that often overshadow the benefits of the bony correction. The radial artery, while typically volar, gives off the dorsal carpal branch which can be encountered and must be ligated or protected. On the ulnar side, the dorsal sensory branch of the ulnar nerve (DSBUN) mandates equal respect during any ulnar-sided or DRUJ-specific dissection.



Exhaustive Indications and Contraindications
The decision to proceed with a corrective osteotomy requires a highly nuanced evaluation. Surgery is strictly warranted when a clear, quantifiable radiographic deformity correlates directly with a specific, anatomically correctable clinical problem, and this deformity poses a substantial risk of progressive dysfunction or future arthrosis. We must be exceptionally wary of pain as the singular primary complaint. Pain relief is a predictable outcome only when it is consistent with an objective, mechanical conflict—such as focal ulnar-sided wrist pain clearly associated with positive ulnar variance and ulnocarpal impingement. Vague, diffuse, or disproportionate pain, especially when accompanied by trophic changes, should prompt a thorough re-evaluation for complex regional pain syndrome (CRPS) and typically contraindicates isolated osteotomy.
Defining the Threshold for Intervention
Specific indications include a symptomatic malunion with a dorsal tilt exceeding 10 degrees past neutral (i.e., >10 degrees of dorsal tilt), radial shortening greater than 4 to 5 millimeters, or an intra-articular step-off greater than 2 millimeters in a young, active patient. Loss of pronosupination directly attributable to DRUJ incongruity secondary to radial deformity is a prime indication. Furthermore, adaptive carpal instability, such as a dorsal intercalated segment instability (DISI) posture driven by a dorsally tilted distal radius, necessitates correction of the osseous platform to restore carpal alignment.
Contraindications must be strictly observed to prevent catastrophic outcomes. Absolute contraindications include active, severe CRPS, as surgical trauma will invariably exacerbate the neuroinflammatory cascade. Advanced, end-stage radiocarpal or midcarpal osteoarthritis is a contraindication for corrective osteotomy; these patients are better served by salvage procedures such as proximal row carpectomy (PRC) or total wrist arthrodesis. Relative contraindications include severe osteopenia or osteoporosis where hardware purchase is highly dubious, uncontrolled medical comorbidities, and patient non-compliance or inability to participate in rigorous postoperative rehabilitation.
| Category | Specific Factors | Clinical Rationale |
|---|---|---|
| Indications | Dorsal tilt > 10°, Volar tilt > 20° | Restores radiocarpal load distribution and prevents midcarpal instability. |
| Indications | Radial shortening > 4-5 mm | Alleviates ulnocarpal impaction and restores DRUJ kinematics. |
| Indications | Intra-articular step-off > 2 mm | Mitigates the onset of rapid post-traumatic osteoarthritis. |
| Contraindications (Absolute) | Active severe CRPS | Surgical trauma worsens the sympathetic dystrophy cascade. |
| Contraindications (Absolute) | Advanced Radiocarpal Arthrosis | Articular cartilage is already destroyed; osteotomy will not relieve pain. |
| Contraindications (Relative) | Severe Osteoporosis | High risk of hardware failure, loss of fixation, and graft collapse. |



Pre-Operative Planning, Templating, and Patient Positioning
Fellows, the success of a corrective osteotomy is dictated long before the first incision is made; it hinges entirely on exhaustive preoperative planning. This is the phase where we anticipate every anatomical anomaly and surgical contingency. Standard posteroanterior (PA) and true lateral radiographs are the baseline, but they are insufficient for complex reconstructions. We must obtain identical views of the uninjured, contralateral wrist. The uninjured wrist serves as our individualized, perfect "template" for desired angular, rotational, and length corrections.
Advanced imaging is non-negotiable in the modern era. A fine-cut CT scan, particularly with 3D surface-rendered reconstructions, is indispensable. Plain radiographs routinely underestimate the degree of articular incongruity and completely fail to accurately depict rotational deformities in the axial plane. The CT scan allows us to precisely evaluate the joint surfaces, map the topography of the malunion, assess the integrity of the sigmoid notch, and plan the exact trajectory of our osteotomy cuts to avoid intra-articular penetration.
The Art and Science of Surgical Templating
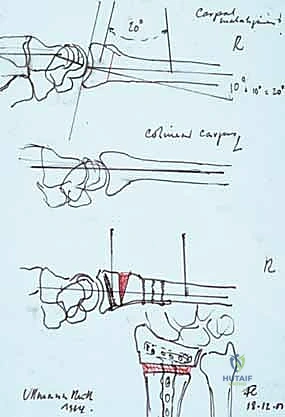
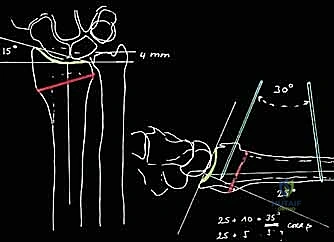
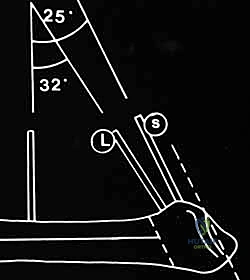
Templating is both an art and a strict geometric science. Using the patient's radiographs (or increasingly, digital templating software overlaying the contralateral anatomy), we draw a detailed reconstruction blueprint. We must determine the Center of Rotation of Angulation (CORA). By drawing the anatomical axis of the proximal radial shaft and the anatomical axis of the deformed distal segment, the intersection marks the CORA. Placing the osteotomy at the CORA prevents secondary translational deformities during angular correction.
The template dictates the exact location and orientation of the planned osteotomy, the precise amount of angular correction required to restore volar tilt and radial inclination, and the linear distraction needed to restore ulnar variance. Crucially, it calculates the exact size, shape, and volume of the structural bone graft required to fill the resulting defect (typically an opening wedge). We must also template the placement of provisional fixation (K-wires, external distractors) and the definitive volar or dorsal locking plate. This meticulous drawing ensures a predictable surgical course and minimizes intraoperative hesitation.




Step-by-Step Surgical Approach and Fixation Technique
Patient positioning is standardized but critical. The patient is placed supine with the operative arm extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. The fluoroscopy unit (C-arm) must be positioned to allow unhindered, orthogonal PA and lateral views without compromising the sterile field. If an autologous iliac crest bone graft (ICBG) is planned, the ipsilateral hip must be simultaneously prepped and draped.
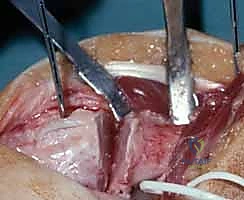
The choice of surgical approach—volar versus dorsal—depends on the direction of the deformity, the planned location of the plate, and the need for intra-articular access. For the classic dorsally angulated malunion (Colles' type), a volar approach utilizing the bed of the flexor carpi radialis (FCR) is currently favored due to the robust soft tissue coverage provided by the pronator quadratus and the mechanical advantages of volar fixed-angle locking plates. The FCR sheath is incised, the tendon retracted ulnarly, and the floor of the sheath is divided to expose the underlying flexor pollicis longus (FPL) and pronator quadratus. The pronator is elevated from its radial and distal borders, exposing the malunited metaphysis.
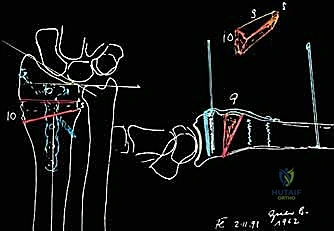
Execution of the Osteotomy and Structural Grafting
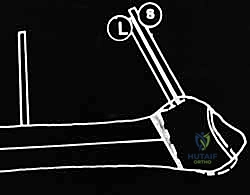
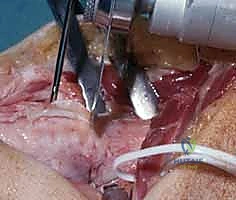
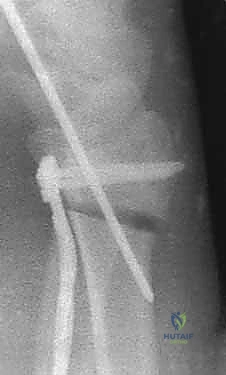
Once exposed, the planned osteotomy site is marked. Provisional K-wires can be placed parallel to the joint surface and perpendicular to the shaft to serve as visual guides for the correction angle. The osteotomy is initiated with an oscillating sagittal saw under continuous cold saline irrigation to prevent thermal necrosis of the bone. To protect the dorsal soft tissues (or volar tissues if a dorsal approach is used), the saw cut is intentionally left incomplete at the far cortex. The osteotomy is then carefully completed using sharp, wide osteotomes.
Following the osteotomy, the deformity is mobilized. This often requires significant soft tissue release, particularly of the brachioradialis insertion, which acts as a powerful deforming force tethering the distal fragment. A laminar spreader or a specialized articulated distractor is utilized to gently open the osteotomy site, restoring length, tilt, and inclination based on our preoperative template. Once the precise anatomical position is achieved and verified via fluoroscopy, the structural bone graft—either meticulously contoured tricortical ICBG or a structural allograft—is impacted into the defect.
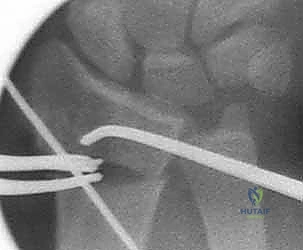
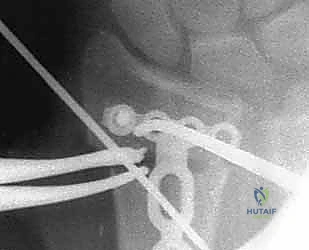
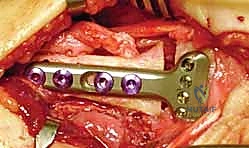
Definitive fixation is achieved with a modern, anatomically contoured locking compression plate. The plate is applied to the volar surface, ensuring it sits proximal to the watershed line to prevent flexor tendon attrition. Distal locking screws are inserted to secure the articular block, followed by proximal cortical screws to compress the plate to the diaphysis, locking the graft in place. Final fluoroscopic images in multiple planes are mandatory to confirm exact hardware placement, restoration of all radiographic parameters, and congruity of the DRUJ.


Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique and exhaustive planning, the corrective osteotomy of the distal radius carries a distinct complication profile. We must transparently discuss these risks and possess the armamentarium to manage them. Complications can be broadly categorized into approach-related soft tissue issues, hardware-related mechanical failures, and biological nonunions. The overall complication rate reported in the literature ranges from 10% to 25%, heavily dependent on the complexity of the initial deformity and patient comorbidities.
Tendon complications are among the most frequent and devastating. When a dorsal approach is utilized, the Extensor Pollicis Longus (EPL) is at high risk of attritional rupture due to friction against dorsal hardware or the bony prominence of the healing osteotomy. Conversely, with volar plating, flexor tendon irritation and rupture (particularly the FPL) occur if the plate is positioned distal to the watershed line or if prominent screw tips penetrate the dorsal cortex. Management of tendon ruptures typically requires prompt diagnosis, hardware removal, and tendon transfer (e.g., EIP to EPL transfer).
Neurologic, Osseous, and Articular Salvage
Neurologic complications primarily involve the superficial radial nerve (SRN) or the palmar cutaneous branch of the median nerve. Traction neuritis or direct laceration can result in severe neuropathic pain. Prevention via meticulous, blunt superficial dissection is paramount. If a symptomatic neuroma develops
Clinical & Radiographic Imaging Archive