Dorsal Capsulodesis for Scapholunate Instability: A Masterclass

Key Takeaway
This masterclass provides a comprehensive, step-by-step guide to dorsal capsulodesis for scapholunate instability. Fellows will learn intricate surgical anatomy, precise intraoperative techniques, and critical decision-making from a seasoned orthopaedic surgeon. We cover patient positioning, meticulous dissection, K-wire stabilization, capsular flap creation, and postoperative management, ensuring a deep understanding of this essential wrist procedure.
Comprehensive Introduction and Patho-Epidemiology
Fellows, welcome to the operating theater. Today, we are addressing a common yet frequently underestimated wrist pathology: scapholunate instability. Specifically, we will be performing a dorsal capsulodesis, a cornerstone procedure for restoring stability to the scaphoid and lunate. This is not merely an exercise in suturing a torn ligament; it is a profound intervention aimed at restoring the intricate kinematics of the carpus and preventing the devastating cascade of degenerative changes known as Scapholunate Advanced Collapse (SLAC). Understanding the pathomechanics of this condition is the absolute prerequisite to executing a successful surgical reconstruction.
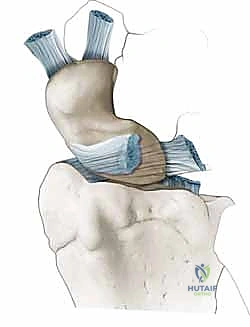
Scapholunate dissociation (SLD) represents the most common form of carpal instability, typically resulting from a fall on an outstretched hand with the wrist in extension, ulnar deviation, and intercarpal supination. This specific vector of force drives the capitate proximally between the scaphoid and lunate, violently disrupting their ligamentous linkage. The resulting instability is not a static event but a progressive deterioration of carpal mechanics. When the crucial anatomic linkage between the scaphoid and lunate is ruptured, the scaphoid naturally tends to flex and pronate under the axial loads of daily use, while the lunate, freed from its scaphoid tether, extends in concert with the triquetrum, leading to the classic Dorsal Intercalated Segment Instability (DISI) deformity.
The sequence of ligamentous failure in SLD is critical to grasp, as it dictates our surgical decision-making. According to Mayfield’s progressive perilunar destabilization model, the injury typically initiates volarly. The volar scapholunate ligament, being the weaker of the two primary stabilizers, tears first. This is subsequently followed by the rupture of the more robust dorsal scapholunate ligament. Early, subtle injuries—often termed "predynamic" or "dynamic" instability—may not manifest classical radiographic signs on standard static views. However, these early stages are precisely when interventions like dorsal capsulodesis are most effective, halting the progression before secondary stabilizers fail and fixed deformities develop.
Once the primary scapholunate ligaments are compromised, the secondary stabilizers of the scaphoid are forced to bear exponentially increased loads. These secondary restraints include the scaphotrapezial-trapezoid (STT) ligament, the scaphocapitate (SC) ligament, and the radioscaphocapitate (RSC) ligament. Their eventual attenuation and failure, driven by repeated cyclical loading of the wrist, lead to overt carpal malalignment and static instability. If this altered, incongruent motion persists, abnormal shear forces are generated across the articular cartilage. This initiates the highly predictable SLAC sequence: beginning with arthrosis at the radial styloid (Stage I), progressing to the entire scaphoid fossa of the radius (Stage II), and ultimately involving the capitolunate articulation (Stage III). Once established arthrosis is present, soft tissue ligament reconstruction is universally contraindicated, underscoring the absolute necessity of timely, precise intervention.
Detailed Surgical Anatomy and Biomechanics
To successfully perform a dorsal capsulodesis, one must possess a three-dimensional, intimate understanding of carpal anatomy and the biomechanical interplay of its stabilizing structures. The radiocarpal and midcarpal joints operate as an extraordinarily complex, interconnected gear system.
The Scapholunate Ligament Complex
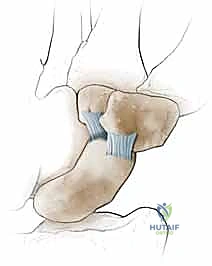
The primary stabilizer of the scapholunate articulation is the interosseous scapholunate ligament (SLIL), which is anatomically and biomechanically divided into three distinct regions. The dorsal ligament is the thickest (2-3 mm) and shortest (2-5 mm) component. Biomechanically, it is the strongest and most resistant to failure under load, serving as the primary restraint to volar-dorsal translation and rotational distraction. Its integrity is paramount for normal carpal kinematics.
The volar ligament, in contrast, is thinner and weaker, often the first to tear during the initial traumatic event. It primarily resists rotational forces but provides significantly less tensile strength than its dorsal counterpart. Finally, the proximal membranous portion is a thin, fibrocartilaginous zone that provides negligible biomechanical strength but functions critically as a synovial seal between the radiocarpal and midcarpal joints. When we assess a tear arthroscopically, we are often looking at the disruption of this proximal membrane, but true instability requires the failure of the dorsal and volar bands.
Secondary Static Stabilizers
The scaphoid's spatial orientation and its relationship with the lunate and the distal carpal row are maintained not only by the SLIL but also by a robust network of secondary extrinsic stabilizers. Volarly, these include the scaphotrapezial-trapezoid (STT), scaphocapitate (SC), and radioscaphocapitate (RSC) ligaments. The RSC ligament acts as a crucial sling, supporting the waist of the scaphoid and preventing excessive flexion.
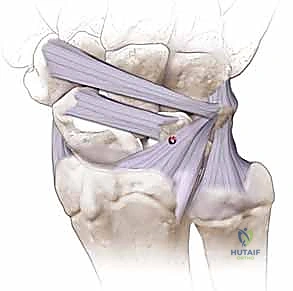
Dorsally, the dorsal intercarpal (DIC) and dorsal radiocarpal (DRC) ligaments form a critical V-shaped stabilizing complex. The DIC ligament, originating from the triquetrum and inserting onto the dorsal ridge of the scaphoid and the trapezium, acts as a secondary restraint to scaphoid flexion. In a dorsal capsulodesis, we are essentially harnessing the local capsular tissues to recreate the tethering effect of these dorsal secondary stabilizers, preventing the scaphoid from rotating into its pathological flexed posture.
Dynamic Stabilizers and Neurovascular Considerations
Beyond static ligaments, we must account for the dynamic stabilizers of the carpus. The flexor carpi radialis (FCR) tendon is intimately related to the volar aspect of the scapholunate joint. During grip and active wrist motion, the FCR acts as a critical dynamic stabilizer, generating forces that counteract excessive scaphoid flexion and pronation.

Surgically, we must also meticulously navigate the regional neurovascular anatomy. The superficial radial nerve (SRN) runs subcutaneously on the dorsoradial aspect of the wrist. We must identify, mobilize, and protect its terminal sensory branches during the initial dissection to prevent debilitating neuromas. Deep to the extensor retinaculum lies the posterior interosseous nerve (PIN), the terminal motor branch of the radial nerve, which provides significant sensory innervation to the dorsal wrist capsule. A neurectomy of the PIN is routinely performed during this exposure to provide long-term pain relief. Finally, the dorsal carpal arch, a vascular arcade lying just beneath the extensor retinaculum, must be preserved or meticulously ligated to maintain the viability of the capsular flap we intend to raise.
Exhaustive Indications and Contraindications
Patient selection is arguably the most critical determinant of success in dorsal capsulodesis. This procedure, originally popularized by Blatt and subsequently modified by many, is not a panacea for all stages of scapholunate instability. It is specifically designed to address a highly specific window in the natural history of the disease.
The ideal candidate for a dorsal capsulodesis is a patient presenting with symptomatic, dynamic or early static scapholunate instability. Clinically, these patients complain of dorsal radial wrist pain, weakness in grip strength, and a positive Watson scaphoid shift test. Radiographically, they may have normal static views, but demonstrate a widened scapholunate interval on clenched-fist views, or they may have a reducible DISI deformity. Crucially, the articular cartilage of the radiocarpal and midcarpal joints must be pristine.
Conversely, dorsal capsulodesis is strictly contraindicated in the presence of established osteoarthritis, specifically any stage of SLAC wrist. Once cartilage degradation has commenced at the radial styloid or the scaphoid fossa, tethering the scaphoid will not alleviate pain and may, in fact, accelerate the degenerative process by altering joint contact pressures. Furthermore, a fixed, irreducible carpal malalignment is an absolute contraindication. If the scaphoid cannot be anatomically reduced into the scaphoid fossa of the radius, a capsulodesis will fail. In such cases, salvage procedures such as a proximal row carpectomy (PRC) or a scaphoid excision and four-corner fusion are required.
| Parameter | Indications for Dorsal Capsulodesis | Absolute Contraindications |
|---|---|---|
| Instability Type | Dynamic or early reducible static SLD | Fixed, irreducible static SLD (Fixed DISI) |
| Cartilage Status | Pristine radiocarpal and midcarpal cartilage | Any evidence of SLAC arthrosis (Stages I-III) |
| Ligament Status | Repairable dorsal SL ligament / Intact secondary stabilizers | Massive tissue loss / Failed prior reconstructions |
| Patient Profile | High-demand patient, compliant with rigorous rehab | Non-compliant patient, severe baseline wrist stiffness |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning ensures that the surgical execution is seamless and that intraoperative surprises are minimized. This begins with a meticulous review of all diagnostic modalities.
Clinical Evaluation and Radiographic Assessment
The clinical examination hinges on the Watson scaphoid shift test, which assesses the dynamic stability of the scaphoid. A palpable "clunk" accompanied by pain as the wrist is moved from ulnar to radial deviation indicates a failure of the scaphoid to smoothly transition into flexion, subluxating dorsally over the dorsal rim of the radius instead. Radiographically, we scrutinize the standard Posteroanterior (PA), lateral, and specialized clenched-fist views.

On the PA view, we assess Gilula’s lines for disruptions and look for the "Terry Thomas" sign—a scapholunate gap greater than 3 mm. The clenched-fist view accentuates this gap by driving the capitate proximally. On the lateral view, we measure the scapholunate angle. A normal angle is between 30 and 60 degrees; an angle greater than 60 degrees is highly indicative of a DISI deformity and significant ligamentous disruption.
Advanced Imaging and Arthroscopic Staging
While plain radiographs provide the foundation, advanced imaging is often necessary for surgical templating. Computed Tomography (CT) scans, particularly sagittal reconstructions, are invaluable for precisely quantifying the degree of dorsal scaphoid subluxation and ruling out occult osseous anomalies, such as subtle scaphoid fractures or impacted distal radius fractures that might mimic or exacerbate instability.

However, wrist arthroscopy remains the undisputed gold standard for diagnosing and staging SLD. It allows us to directly visualize the ligamentous disruption, probe the interosseous interval, and, most importantly, directly inspect the articular surfaces to definitively rule out early SLAC changes. We utilize the Geissler classification to grade the instability. A Geissler Grade 3 or 4 tear—where a probe can be passed freely between the scaphoid and lunate, indicating complete disruption of both palmar and dorsal components—is the classic indication for an open reconstruction and capsulodesis, provided the cartilage remains intact.
Operating Room Setup and Patient Positioning
The patient is brought into the operating theater and placed under general or regional anesthesia. Positioning is critical for surgeon ergonomics and optimal exposure. The patient is positioned supine, with the hips and knees flexed slightly to alleviate lower back strain during what can be a meticulous, time-consuming procedure.
The affected upper extremity is prepped and draped entirely free and placed on a specialized, radiolucent hand table. The arm is positioned in pronation, presenting the dorsal aspect of the wrist directly to the surgical field. A pneumatic tourniquet is applied to the proximal arm and inflated to 250 mmHg after exsanguination with an Esmarch bandage, ensuring a completely bloodless field. This is non-negotiable, as identifying the delicate dorsal capsular structures and terminal nerve branches requires pristine visualization. Finally, the fluoroscopy C-arm is positioned perpendicular to the table, allowing the surgeon to bring the machine in and out of the field effortlessly for orthogonal intraoperative imaging without needing to awkwardly reposition the patient's arm.
Step-by-Step Surgical Approach and Fixation Technique
We are now ready to commence the reconstruction. Precision in soft tissue handling and rigid osseous fixation are the hallmarks of a successful dorsal capsulodesis.
Incision, Interval, and Neurologic Protection
We begin by palpating our primary bony landmarks: Lister's tubercle on the distal radius and the radial styloid. The skin incision is oblique, measuring approximately 4 to 5 centimeters. It originates roughly 1 cm distal and ulnar to Lister's tubercle and extends distally and radially toward the base of the second metacarpal, passing about 1 cm distal to the radial styloid.
This oblique orientation is highly deliberate; it provides expansive exposure of the radiocarpal joint while running parallel to Langer's lines, optimizing cosmetic healing and minimizing tension on the wound edges during post-operative wrist flexion.
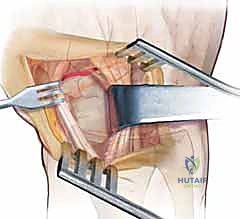
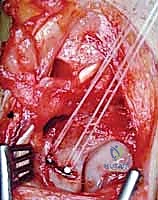
Immediately upon incising the dermis, we must utilize blunt dissection to identify and protect the terminal sensory branches of the superficial radial nerve (SRN). These branches are delicately mobilized and retracted radially. Retraction must be gentle to avoid neuropraxia. We then identify the extensor retinaculum and sharply incise it over the third dorsal compartment, releasing the Extensor Pollicis Longus (EPL) tendon. We transpose the EPL radially and retract the Extensor Digitorum Communis (EDC) tendons ulnarly. Deep within the floor of the fourth compartment, we identify the posterior interosseous nerve (PIN) lying on the interosseous membrane. A 1-cm segment of the PIN is sharply excised, and the proximal stump is allowed to retract into the deep musculature to prevent painful neuroma formation, effectively denervating the dorsal capsule to provide long-term analgesia.
Extensor Retinaculum and Capsular Flap Creation
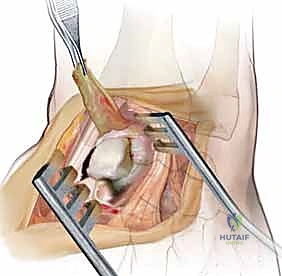
With the extensor tendons retracted, the dorsal wrist capsule is fully exposed.
Here, we design our proximally based capsular flap, the critical element of the Blatt procedure. The flap is typically 1 cm wide. We make two parallel longitudinal incisions through the dorsal capsule, centered over the scapholunate interval. The distal release is made transversely at the level of the midcarpal joint, preserving the dorsal intercarpal (DIC) ligament if possible.
We carefully elevate this robust flap of tissue from distal to proximal, leaving its proximal attachment firmly anchored to the dorsal rim of the distal radius. This flap incorporates portions of the dorsal radiocarpal ligament. Extreme care must be taken during elevation to preserve the vascularity of the flap, avoiding excessive thinning or trauma to the dorsal carpal arch vessels that supply it.
Joint Preparation, Reduction, and K-Wire Fixation
Elevation of the capsular flap exposes the radiocarpal joint and the pathology itself: the disrupted scapholunate interval. We use a rongeur and a curette to meticulously debride the frayed, non-viable remnants of the dorsal SL ligament down to bleeding bone on both the scaphoid and lunate articular margins. This decortication is essential to promote a robust healing response.
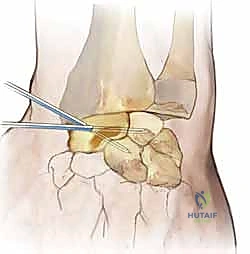
Next, we must anatomically reduce the carpus. This requires a coordinated maneuver: the scaphoid, which is pathologically flexed and pronated, must be extended and supinated. Simultaneously, the lunate, which is extended in a DISI posture, must be flexed back into a neutral alignment with the radius. We achieve this using two 0.062-inch K-wires as "joysticks," driving one into the dorsal pole of the scaphoid and another into the lunate.

Once anatomical reduction is confirmed visually and via fluoroscopy (aiming for a scapholunate angle of 45 degrees), we secure the reduction. A 0.045-inch or 0.062-inch K-wire is driven from the radial aspect of the scaphoid directly into the lunate.
To neutralize the massive forces across the midcarpal joint and protect our repair, a second K-wire is driven from the scaphoid into the capitate. This scaphocapitate wire is critical for maintaining the scaphoid in its extended posture while the capsulodesis heals.
Flap Inset and Soft Tissue Closure
With the carpus rigidly pinned in anatomical alignment, we prepare the recipient site for the capsular flap. Using a small rongeur or a high-speed burr, we create a transverse bony trough in the dorsal aspect of the distal scaphoid pole, strictly distal to its axis of rotation.

The distal end of our proximally based capsular flap is then advanced distally and seated firmly into this scaphoid trough.

Fixation of the flap into the trough can be achieved using intraosseous suture anchors or via transosseous drill holes utilizing non-absorbable, heavy braided suture (e.g., #2-0 FiberWire).

The tension on the flap must be precise—tight enough to tether the scaphoid and prevent it from flexing, but not so tight that it induces a fixed extension contracture of the wrist.

Once the flap is securely anchored, we confirm our final construct under fluoroscopy. The remaining dorsal capsule is closed with absorbable sutures.

The extensor retinaculum is repaired, but we leave the EPL tendon transposed subcutaneously to prevent attrition and subsequent rupture over the hardware or the healing capsular repair. The skin is closed meticulously, and the wrist is placed in a bulky, well-padded volar surgical splint.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, dorsal capsulodesis is not without its potential complications. As orthopedic surgeons, we must counsel our patients extensively regarding these risks and be prepared to manage them effectively.
The most universal and predictable "complication"—which is more accurately described as an inherent biomechanical trade-off of the procedure—is a permanent loss of terminal wrist flexion. By design, we are tethering the distal pole of the scaphoid to the dorsal radius. This prevents pathological scaphoid flexion, but it also invariably limits physiological wrist flexion. Patients can expect an average loss of 20 to 30 degrees of palmar flexion compared to their contralateral side. Grip strength, however, typically improves as the painful instability is resolved.

Recurrent instability or stretching out of the capsulodesis over time is a significant concern, occurring in 15% to 25% of cases in long-term follow-up. This is often due to biological failure of the capsular tissue to withstand the massive shear forces of the carpus, particularly in heavy laborers or athletes who return to high-impact activities prematurely. Pin tract infections from the percutaneous K-wires, hardware migration, and superficial radial nerve neuritis are also documented risks that require vigilant post-operative monitoring.
If a dorsal capsulodesis fails, resulting in recurrent severe pain or the progression to SLAC arthrosis, salvage procedures become necessary. Because the capsulodesis does not burn any bridges regarding future bony procedures, we can seamlessly transition to a proximal row carpectomy (PRC) or a scaphoid excision with four-corner arthrodesis. These salvage operations provide reliable pain relief, albeit at the cost of further reducing wrist range of motion.
| Complication | Estimated Incidence | Prevention and Management Strategies |
|---|---|---|
| Loss of Wrist Flexion | 90-100% (Expected) | Pre-op counseling; precise tensioning of the flap (avoid over-tightening). |
| Recurrent Instability | 15-25% | Rigid K-wire fixation for 8 weeks; strict adherence to rehab protocols; avoiding early heavy loading. |
Clinical & Radiographic Imaging Archive

