Wrist Implant Arthroplasty
Comprehensive Introduction and Patho-Epidemiology
Historically, the gold standard for the treatment of end-stage wrist degeneration and debilitating radiocarpal and midcarpal pain was total wrist arthrodesis. As a reliable salvage procedure, fusion of the wrist joint can provide reasonable pain relief, correct profound deformity, and offer relative preservation of upper extremity function, particularly for heavy laborers. Unfortunately, arthrodesis of the painful wrist does not guarantee complete pain relief, nor does it come without significant functional impairment. The loss of the dart-thrower's motion and the inability to position the hand in space can severely limit a patient's ability to perform activities of daily living, particularly personal hygiene and tasks requiring fine motor dexterity in confined spaces.
In contrast, total wrist arthroplasty (TWA) provides an attractive, motion- and function-sparing alternative to wrist arthrodesis. Multiple longitudinal studies have unequivocally demonstrated that patients consistently prefer motion-sparing procedures over rigid fixation. Pain relief is reliably achieved, along with the preservation of a functional arc of wrist motion. In much the same vein as arthroplasty efforts in other major appendicular joints, early wrist replacement designs were initially successful in relieving pain; however, they suffered from significant biomechanical design flaws. Early prostheses failed to achieve the long-term survivorship results provided by joint replacements in the shoulder, hip, and knee, primarily due to difficulties with implant centering, soft tissue balance, and catastrophic distal fixation failure.

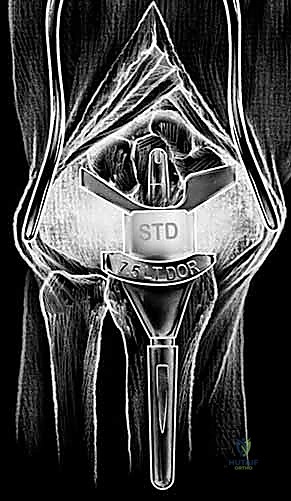
The evolution of modern implant design has capitalized on modularity, superior tribology, and improved anatomic geometries to provide enhanced longevity. A great debt of gratitude is owed to Dr. Jay Menon for popularizing stable distal screw fixation into the carpus, fundamentally altering the biomechanical paradigm by avoiding the destructive lever arm created by a long intramedullary stem inserted into the third metacarpal. Today, the three most popular wrist designs utilized in the United States are the Universal 2 (KMI/Integra), the Re-Motion (Small Bone Innovations [SBI]), and the Maestro (Biomet). The Universal 2 Total Wrist prosthesis, an improved version of Dr. Menon's original design, utilizes a flat carpal cut, screw fixation distally into both the second metacarpal and hamate, and a modular, distally based polyethylene cap that articulates with a proximal cobalt chrome radial component.


End-stage wrist degeneration is the common endpoint of multiple pathophysiologic pathways, universally involving the loss of articular joint space and progressive carpal collapse. The classic pattern of deformity and destruction, particularly in rheumatoid arthritis, involves the radiocarpal and midcarpal joints alongside the distal radioulnar joint (DRUJ). Attenuation of the extrinsic wrist ligaments destabilizes the carpus, often resulting in profound ulnar and volar translation of the carpus relative to the radius. The excitement over modern wrist replacement systems has stimulated continuous investigation, with current designs striving to achieve a more anatomic wrist joint through sophisticated component design and precision instrumentation that respects the native kinematics of the radiocarpal articulation.
Detailed Surgical Anatomy and Biomechanics
The wrist joint is a highly complex, multi-articulated structure consisting of the distal radial articular surface, the distal ulna, the triangular fibrocartilage complex (TFCC), eight carpal bones arranged into proximal and distal rows, and the bases of the five metacarpals. Four significant articulations dictate the kinematics of the wrist: the radiocarpal joint, the midcarpal joint, the carpometacarpal (CMC) joints, and the DRUJ. A sophisticated combination of interosseous, intrinsic, and extrinsic ligaments provides dynamic and static stabilization. Understanding this intricate anatomy is paramount for the arthroplasty surgeon, as the success of the implant relies heavily on restoring the native centers of rotation and balancing the surrounding soft tissue envelope.

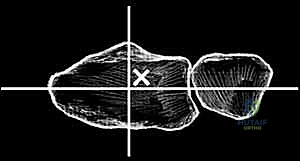
The proximal row of the carpus (scaphoid, lunate, triquetrum) articulates with the distal radius to form the radiocarpal joint, functioning largely as an intercalated segment whose motion is dictated by the surrounding osseous contours and ligamentous tethers. The distal carpal row articulations with the metacarpal bases form the relatively rigid CMC joints. Within the distal carpal row, the primary center of wrist motion is located at the head of the capitate, slightly palmar to the geometric center of the head. This center of rotation may or may not be perfectly colinear with the third metacarpal shaft, depending on the unique anatomic variance of each patient. Proximally, the center of wrist motion lies slightly ulnar to the central axis of the radial intramedullary canal.

Normal anatomic parameters of the distal radial articular surface include a volar tilt of approximately 11 degrees and a radial inclination of 22 degrees. Recreating these spatial relationships is a fundamental goal of modern implant systems. The Re-Motion Total Wrist, for instance, is fundamentally designed to resurface the distal radius while allowing about 15 degrees of intended "wiggle" or toggle built into the snap fit of the polyethylene cap with the carpal plate, compensating for minor kinematic mismatches. Conversely, the Maestro Wrist utilizes a metal convex component articulating with a concave polyethylene component, mimicking successful total hip and shoulder designs, and features a modular titanium stem designed to achieve diaphyseal fill and rotational stability.


The sigmoid notch of the distal radius provides the articulation for the DRUJ. Strong dorsal and palmar radioulnar ligaments provide critical DRUJ stability. While earlier designs like the Re-Motion made no specific attempt to preserve the DRUJ, modern iterations and systems like the Universal 2 and Maestro feature instrumentation and radial component geometries specifically designed to preserve the DRUJ and the ulnar head. In cases where the DRUJ is irreparably damaged, many wrist replacements are performed in conjunction with ulnar head replacement arthroplasty or a Darrach procedure, though preservation of the ulnar head is always preferred to maintain the ulnocarpal ligamentous complex and provide a buttress against ulnar translation.
Exhaustive Indications and Contraindications
The primary indication for total wrist arthroplasty remains joint destruction secondary to the profound inflammatory effects of rheumatoid arthritis. However, as implant survivorship has improved, indications have expanded to manage the pain, deformity, and loss of motion coincident with end-stage arthritis resulting from osteoarthritis, posttraumatic arthritis, or avascular necrosis (such as Kienböck's or Preiser's disease). Total wrist arthroplasty also provides an excellent salvage option for functional deformities such as scapholunate advanced collapse (SLAC), scaphoid nonunion advanced collapse (SNAC), or irreparable intra-articular trauma to the distal radius or carpus.
Patients considered for arthroplasty must be thoroughly vetted. The ideal patient is typically an older, lower-demand individual with significant wrist pain and loss of a functional range of motion, but who retains adequate bone stock, a reasonably balanced soft tissue envelope, and intact extrinsic flexor and extensor tendons. Instability and gross misalignment are frequently present, particularly in the rheumatoid population where carpal collapse, ulnar translation, or volar subluxation can be dramatic. If these deformities, along with motor power deficits or localized bone loss, can be surgically corrected during the procedure, wrist replacement can be highly successful.
Previous surgical interventions, including proximal row carpectomy (PRC) and even previous partial or total arthrodesis, are not absolute contraindications to wrist replacement. In the setting of a failed PRC or painful partial fusion, conversion to a TWA can restore function, though the surgeon must counsel the patient that they should not expect the same postoperative range of motion as a primary arthroplasty. The presence of functional motors, particularly the extensor carpi radialis longus and brevis (ECRL/ECRB) and the extensor carpi ulnaris (ECU), is mandatory to provide dynamic stability to the unconstrained or semi-constrained prosthesis.
Absolute contraindications to wrist replacement are ongoing or deep infection, a history of recalcitrant septic arthritis of the wrist, and profound, uncorrectable loss of the extrinsic motor tendons. Relative contraindications include highly unstable and markedly collapsed wrists with severe osteopenia, significant segmental bone loss that precludes stable implant fixation, and high-demand patients (e.g., heavy manual laborers, active wheelchair users, or patients relying on walking aids that load the wrist). In these populations, total wrist arthrodesis remains the most prudent and durable surgical choice.
| Category | Specific Conditions | Clinical Considerations |
|---|---|---|
| Primary Indications | Rheumatoid Arthritis, Primary Osteoarthritis, Post-traumatic Arthritis (SLAC/SNAC) | Severe pain, failed conservative management, desire to maintain functional ROM. |
| Salvage Indications | Failed Proximal Row Carpectomy, Failed Partial Arthrodesis, Avascular Necrosis | Requires careful preoperative templating to ensure adequate remaining bone stock for distal fixation. |
| Absolute Contraindications | Active deep infection, Charcot arthropathy, Absent/irreparable wrist motors | High risk of catastrophic failure, dislocation, or systemic spread of infection. |
| Relative Contraindications | High-demand laborers, crutch/walker dependence, severe uncorrectable bone loss | Arthrodesis is strongly preferred to prevent early aseptic loosening and implant failure. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of a successful wrist implant arthroplasty. The clinical evaluation must document active and passive range of motion, grip strength, and the integrity of the extensor and flexor tendons. Pain should be characterized; pain throughout the arc of motion suggests global articular wear, while pain strictly at the endpoints may indicate impingement. Nonoperative management, consisting of activity modification, nonsteroidal anti-inflammatory medications, localized corticosteroid injections, and supportive bracing, should be exhausted. Persistent pain and loss of function despite these conservative measures constitute a failure of nonoperative treatment and a definitive indication for surgical intervention.
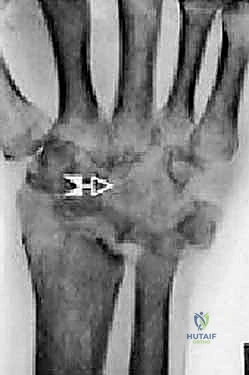
Imaging studies are critical for both diagnosis and templating. Standard posteroanterior (PA), lateral, and oblique wrist radiographs provide sufficient imaging for the vast majority of preoperative planning. In cases of severe deformity, prior trauma, or suspected massive bone loss, a non-contrast computed tomography (CT) scan with 3D reconstructions is highly recommended to assess the precise geometry of the distal radius and the integrity of the capitate and metacarpal bases. Digital or acetate templating is utilized to determine the appropriate size for the radial body and stem, the capitate stem, the carpal plate and body, the scaphoid augment (if utilized), and the lengths of the radial and ulnar fixation screws.
A gross estimate of the amount of distal radius to be resected must be made preoperatively to ensure the joint line is restored without over-tensioning the soft tissues or causing relative lengthening of the ulna, which could lead to ulnocarpal impingement. The surgeon must also plan for the management of the DRUJ; if the DRUJ is arthritic but the ulnar head is structurally sound, a matched ulnar head replacement or a hemiresection may be templated alongside the TWA.

The procedure is performed with the patient in the supine position. The operative extremity is placed on a standard hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. The procedure can be performed under general anesthesia or regional anesthesia (brachial plexus block), depending on patient comorbidities and anesthesiologist preference. Intravenous antibiotics are administered prior to tourniquet inflation. The arm is prepped and draped in a standard sterile fashion, ensuring that the elbow is free to allow for assessment of forearm rotation and that the fluoroscopy unit (C-arm) can easily enter the surgical field from the distal or lateral aspect of the hand table.
Step-by-Step Surgical Approach and Fixation Technique
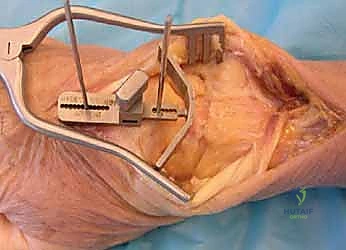
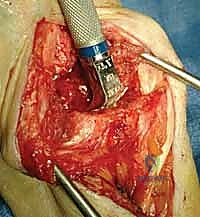
A longitudinal dorsal incision, positioned slightly radial to the midline, is made extending from approximately 4 cm proximal to the radiocarpal joint down to the midpoint of the third metacarpal shaft. Sharp dissection is carried down through the subcutaneous tissues to the level of the extensor retinaculum, taking meticulous care to identify and protect the sensory branches of the superficial radial nerve and the dorsal sensory branch of the ulnar nerve. The third dorsal compartment is opened, and the extensor pollicis longus (EPL) tendon is exposed, mobilized, and retracted radially. The retinaculum is then elevated as a continuous flap. The radial wrist extensors (ECRL and ECRB) are exposed and mobilized radially, while the first compartment tendons are mobilized from the distal radius and protected. The tendons of the fourth and fifth compartments are mobilized ulnarly, ideally without opening their respective synovial compartments to prevent postoperative adhesions.

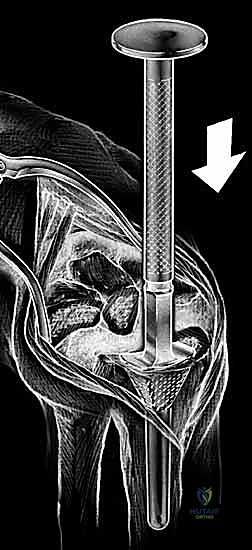
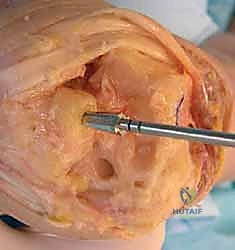
With the extensor tendons mobilized and safely retracted, a longitudinally based capsulotomy is performed. The capsule is reflected as radially and ulnarly based full-thickness flaps, exposing the distal radius and the entire carpus down to the base of the third metacarpal. Preparation of the distal radius involves scoring a reference line to ensure the DRUJ is preserved. The radial canal is sequentially broached to accept the modular radial stem. The modular radial stem component is designed to fill the distal radius canal to prevent loosening and provide rotational stability. While approved for implantation with bone cement (PMMA), most modern wrists are implanted with press-fit, cementless fixation to encourage osteointegration. Cement is generally reserved for cases of significantly compromised bone stock, severe osteopenia, or revision scenarios.


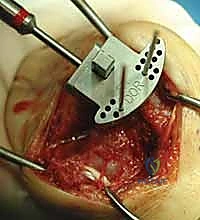
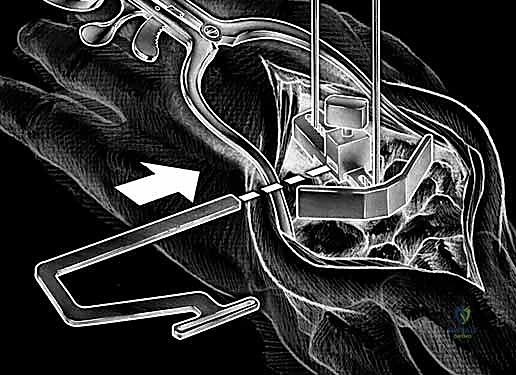
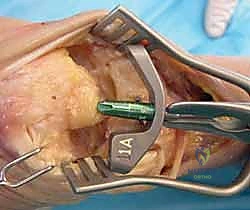
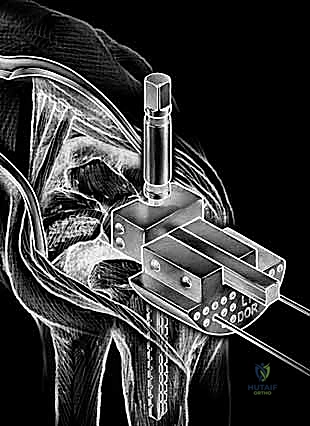
Carpal preparation requires exacting precision. Using the Maestro system as the archetype, the carpal resection guide is positioned to allow resection of 2 to 3 mm of the capitate head. It is provisionally held in position with two 0.062-inch Kirschner wires. The first wire is placed into the capitate neck and the second into the metaphysis of the third metacarpal, ensuring that the guide is perfectly parallel to the third metacarpal axis. With proper placement, the ulnar guide wing will lie close to the triquetrum–hamate articulation, and the radial wing will bisect the scaphoid at its distal third.
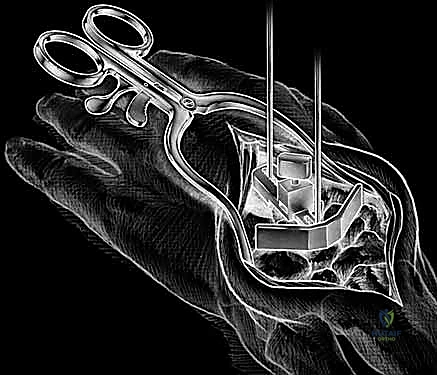
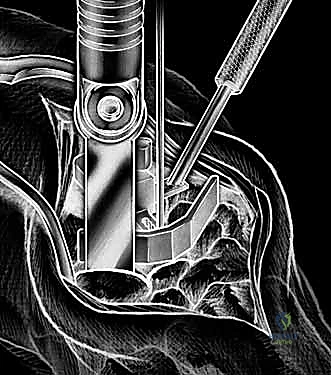
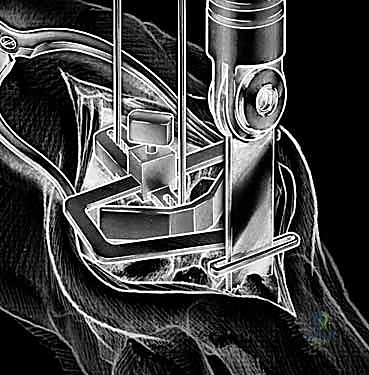

With the wrist held in neutral, the radius is scored through the cutting slot in the guide to provide a reference for the distal radial resection. The thumbscrew on the carpal resection guide is loosened to allow insertion of the radial resection guide boom. Following radial resection, the scaphoid, capitate head, hamate edge, and triquetrum are resected at a precise 90-degree angle to the axis of the forearm jig. The trial carpal plate is provisionally determined by the curvature and width of the remaining proximal carpal surface; it must lie flush with the hamate and proximal capitate surfaces. Unlike older designs, it is not always necessary to attempt fusion of the distal pole of the scaphoid to the surrounding carpus. The Maestro Wrist has a provision to replace the entire scaphoid using a carpal plate incorporating a modular radial augment, of which three separate sizes are available.




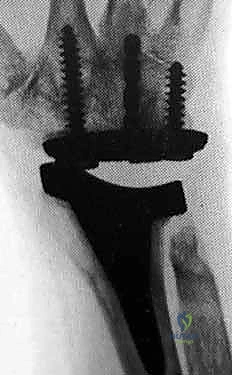
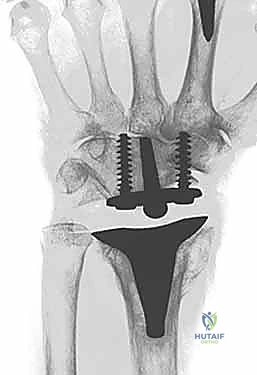
Following capitate reaming, the chosen carpal plate and stem are assembled and inserted into the capitate and seated onto the resected carpal surface. The carpal plate is anchored to the carpus with a radial screw that optimally does not penetrate the second metacarpal, and a second screw placed ulnarly into the hamate. This construct ensures stable distal fixation while avoiding the deleterious lever arm of a long metacarpal stem. Trial reductions are performed to assess stability, range of motion, and impingement. Once kinematics are confirmed, the definitive ultra-high-molecular-weight polyethylene (UHMWPE) body—which is direct compression molded onto a cobalt chrome alloy radial body—is impacted. The capsule and extensor retinaculum are meticulously repaired to prevent extensor tendon bowstringing and provide a robust soft tissue envelope over the implant.
Complications, Incidence Rates, and Salvage Management
Despite significant advancements in implant design and surgical technique, total wrist arthroplasty remains a technically demanding procedure with a distinct complication profile. The most prevalent long-term complication is aseptic loosening, primarily affecting the distal (carpal) component. Early generation implants with long metacarpal stems experienced loosening rates exceeding 30% at ten years due to the massive cantilever forces exerted during flexion and extension. Modern designs utilizing carpal plate and screw fixation have drastically reduced this incidence, though osteolysis and subsidence can still occur, particularly in patients who exceed postoperative weight-bearing restrictions.
Instability and dislocation represent another major mode of failure, often stemming from inadequate soft tissue balancing, improper restoration of the joint line, or undersizing of the radial or carpal components. Volar dislocation is the most common pattern, frequently associated with attenuation of the volar capsule or excessive dorsal tilt of the radial component. Deep periprosthetic joint infection (PJI) occurs in approximately 1-3% of cases. The rheumatoid population is at a inherently higher risk due to systemic immunosuppression and the use of disease-modifying antirheumatic drugs (DMARDs) and biologic agents.
When catastrophic failure occurs—whether due to aseptic loosening, unremitting instability, or infection—salvage management is required. In cases of aseptic loosening with preserved bone stock, revision arthroplasty with a larger stemmed component or the use of structural allograft may be attempted. However, the most reliable salvage procedure for a failed total wrist arthroplasty is conversion to a total wrist arthrodesis. This typically requires the removal of all hardware, aggressive debridement of metallosis and fibrous tissue, and the use of a robust structural autograft (usually from the iliac crest) to span the intercalary defect left by the explanted prosthesis, stabilized with a dorsal spanning locking plate.
| Complication | Estimated Incidence | Etiology / Risk Factors | Management Strategy |
|---|---|---|---|
| Aseptic Loosening | 5% - 15% (at 10 years) | Stress shielding, particulate wear debris, excessive loading. | Revision arthroplasty if bone stock allows; conversion to arthrodesis. |
| Instability / Dislocation | 2% - 5% | Soft tissue imbalance, component malposition, extensor tendon rupture. | Closed reduction and bracing (acute); Revision for component realignment or soft tissue reconstruction. |
| Periprosthetic Infection | 1% - 3% | Immunosuppression (RA patients), poor soft tissue envelope. | Irrigation and debridement, implant retention (acute); Two-stage explantation and arthrodesis (chronic). |
| Tendon Rupture | < 2% | Prominent hardware, attrition over un-repaired retinaculum. | Tendon transfer (e.g., EIP to EPL) or primary repair if feasible. |
Phased Post-Operative Rehabilitation Protocols
The success of a wrist implant arthroplasty is inextricably linked to a rigid, well-structured postoperative rehabilitation protocol. The immediate postoperative phase (Phase I: 0-2 weeks) focuses on strict immobilization, edema control, and the prevention of digital stiffness. The wrist is immobilized in a bulky, well-padded volar splint in neutral alignment. Patients are instructed to keep the extremity elevated and to perform aggressive active range of motion exercises of the fingers, thumb, elbow, and shoulder to promote venous return and prevent tendon adhesions.
Phase II (2-6 weeks) begins with the first postoperative clinic visit. The surgical dressings and sutures are removed. A custom-fabricated thermoplastic volar wrist orthosis is constructed by a certified hand therapist. The patient is permitted to remove the splint multiple times a day to initiate a gentle, therapist-guided active and active-assisted range of motion program for the wrist. Emphasis is placed on restoring the dart-thrower's motion (radial extension to ulnar flexion) and forearm pronation and supination. Passive stretching and forceful manipulation are strictly contraindicated during this phase to protect the capsular repair and allow for early osteointegration of the cementless components.
Phase III (6-12 weeks) involves progressive weaning from the thermoplastic splint, initially transitioning to use only during sleep or strenuous activities. Gentle isometric strengthening is introduced, progressing to light isotonic exercises. The patient is educated on the permanent lifelong restrictions required to protect the implant. Heavy lifting, impact loading, and the use of vibrating hand tools must be avoided. A permanent lifting restriction of 10 to 15 pounds is universally recommended. Patients are counseled that the goal of the surgery is a functional, pain-free arc of motion—typically 30 to 40 degrees of extension and 30 to 40 degrees of flexion—rather than a return to normal, unimpeded kinematics.
Summary of Landmark Literature and Clinical Guidelines
The body of literature supporting the use of modern, third- and fourth-generation total wrist arthroplasty systems is robust and growing. The Uni2 wrist is the prosthesis with which there is the greatest long-term clinical experience to date, with multiple series demonstrating survivorship rates exceeding 85% at 10 years. The results are highly encouraging, particularly regarding the maintenance of pain relief and the preservation of the DRUJ. Similarly, preliminary and mid-term results with the Re-Motion and Maestro wrists have demonstrated excellent patient-reported outcome measures (PROMs), including significant improvements in the Patient-Rated Wrist Evaluation (PRWE) and the Disabilities of the Arm, Shoulder and Hand (DASH) scores.
Biomechanical studies have definitively validated the paradigm shift away from metacarpal intramedullary stems. Finite element analysis and cadaveric kinematic studies have shown that distal screw fixation into the carpus, combined with a broad carpal plate, more evenly distributes compressive loads across the midcarpal joint and vastly reduces the shear forces that lead to early osteolysis. Furthermore, comparative cohort studies have repeatedly demonstrated that patients who undergo TWA report higher satisfaction rates and better ability to perform personal hygiene tasks compared to matched cohorts undergoing total wrist arthrodesis.
Future directions in wrist implant arthroplasty are
Clinical & Radiographic Imaging Archive