Distal Scaphoid Pole Excision for Scaphoid Nonunion Advanced Collapse (SNAC) Wrist: An Intraoperative Masterclass
Key Takeaway
Join us in the OR for a detailed masterclass on distal scaphoid pole excision, a low-morbidity option for SNAC wrist stage I. We'll cover intricate anatomy, meticulous preoperative planning, and step-by-step intraoperative execution via both volar and dorsal approaches. Learn critical pearls, potential pitfalls, and comprehensive postoperative management to ensure optimal patient outcomes for this challenging condition.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to the operating theater. Today, we are undertaking a rigorous examination of a challenging yet critically important salvage procedure: the Distal Scaphoid Pole Excision for Scaphoid Nonunion Advanced Collapse (SNAC) Wrist. This operation stands as a testament to thoughtful, biomechanically sound surgical salvage, offering significant pain relief and functional improvement for a carefully selected cohort of patients. The scaphoid is the most frequently fractured bone in the carpus, accounting for up to 70% of all carpal fractures. While acute, non-displaced fractures boast union rates exceeding 90% when appropriately immobilized, missed diagnoses, delayed presentations, or inadequate initial stabilization invariably lead to nonunion. The ensuing cascade of carpal destabilization is predictable, devastating, and biomechanically unforgiving.
Here, we observe a classic presentation of a failed open reduction and internal fixation (ORIF) of a scaphoid nonunion. Despite surgical intervention, the biological and mechanical environment was insufficient to achieve osteosynthesis, leading to hardware failure and persistent nonunion.

Figure 1A: Failed ORIF of a scaphoid nonunion (PA view) demonstrating hardware loosening and persistent radiolucency at the fracture site.

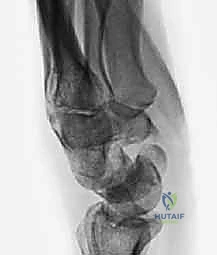
Figure 1B: Failed ORIF of a scaphoid nonunion (Lateral view) illustrating the early signs of carpal collapse and dorsal intercalated segment instability (DISI).
When primary treatments fail, and the patient presents with persistent, debilitating pain coupled with post-traumatic arthritis localized to the distal pole of the scaphoid and the radial styloid, we classify this as SNAC wrist Stage I. In these specific scenarios, partial scaphoid excision emerges as a compelling, low-morbidity alternative to more radical salvage procedures. This approach is particularly relevant given the current lack of biomechanically acceptable and biologically inert prostheses for total scaphoid replacement. Traditional revision ORIF with vascularized or non-vascularized structural bone grafting, while theoretically an option, carries a documented failure rate approaching 50% in the presence of proximal pole avascular necrosis or long-standing nonunion. This high failure rate pushes the reconstructive surgeon towards more reliable, palliative salvage procedures that preserve motion while eliminating the painful arthritic articulation.
The pathogenesis of the SNAC wrist is rooted in the uncoupling of the scaphoid's integrated biomechanical function. A scaphoid nonunion inevitably leads to the development of post-traumatic arthritis, primarily affecting the radioscaphoid joint. The progression timeline varies based on patient activity level and the specific morphology of the nonunion, but the vast majority of patients will demonstrate radiographic evidence of degenerative changes within 5 to 10 years post-injury. The fundamental cause is the abnormal, asynchronous motion between the ununited, frequently flexed distal scaphoid fragment and the articular surface of the radial styloid. This focal point of abnormal biomechanics leads to accelerated cartilage wear, subchondral sclerosis, and eventual joint space obliteration.
We classify this progressive arthropathy into four distinct stages, which dictate our surgical decision-making:
Staging of Scaphoid Nonunion Advanced Collapse
The progression of SNAC wrist follows a predictable spatial pattern of articular degeneration, moving from radial to ulnar and from distal to proximal within the carpus. Recognizing these stages is paramount, as distal scaphoid excision is strictly contraindicated in advanced stages.
SNAC Wrist Stage I: The arthritic process is initially confined to the articulation between the distal pole of the scaphoid and the radial styloid. The proximal pole of the scaphoid, still attached to the lunate via the intact scapholunate interosseous ligament, maintains a relatively congruous, albeit altered, relationship with the scaphoid fossa of the radius. This is the ideal stage for distal pole excision.
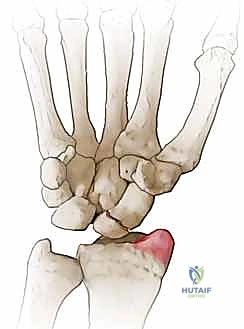
Figure 3A: Arthritis localized between the distal pole of the scaphoid and the radial styloid (SNAC grade I).
SNAC Wrist Stage II: As the abnormal kinematics persist, the degenerative changes progress proximally to involve the entire radioscaphoid articulation. The proximal pole, previously spared, now exhibits chondral wear against the scaphoid fossa of the distal radius. Distal pole excision may still be considered here if the proximal pole wear is minimal, but outcomes are less predictable than in Stage I.

Figure 3B: Progression to SNAC grade II, showing more diffuse radioscaphoid joint space narrowing.
SNAC Wrist Stage III: The destabilization of the carpus eventually leads to midcarpal arthritis. Specifically, the capitate migrates proximally into the space created by the collapsed scaphoid, leading to capitolunate and capitoulnar (capitohamate) arthropathy. At this stage, distal scaphoid excision is absolutely contraindicated, as it will not address the midcarpal pain.

Figure 3C: Progression to SNAC grade III, with evident midcarpal degenerative changes.
SNAC Wrist Stage IV: The final common pathway is pancarpal arthritis. The radiolunate joint, which is classically spared in both Scapholunate Advanced Collapse (SLAC) and early SNAC wrists due to the concentric, spherical nature of the articulation, finally succumbs to the massive biomechanical derangement.

Figure 3D: Progression to SNAC grade IV, demonstrating diffuse pancarpal arthropathy including the radiolunate joint.
Detailed Surgical Anatomy and Biomechanics
To execute a distal scaphoid excision with precision, the surgeon must possess an intimate understanding of carpal osteology, ligamentous constraints, and local neurovascular topography. The carpus is elegantly divided into two functional rows. The proximal carpal row (scaphoid, lunate, triquetrum) acts as an intercalated segment with no direct tendon insertions, moving entirely in response to the mechanical forces exerted by the surrounding articulations and ligaments. The distal carpal row (trapezium, trapezoid, capitate, hamate) functions as a rigid unit, strongly bound to the metacarpal bases.
The scaphoid is anatomically and biomechanically unique; it acts as an oblique bridge connecting these two functional rows. Its precarious position, spanning the midcarpal joint, coupled with its largely cartilaginous surface (over 80% articular cartilage), makes it mechanically vulnerable to fracture, particularly with forced dorsiflexion and ulnar deviation injuries. When the scaphoid fractures and fails to unite, the proximal and distal rows become mechanically uncoupled. The distal scaphoid fragment tends to flex along with the distal carpal row, while the proximal fragment extends with the lunate, leading to the classic "humpback" deformity and secondary DISI.
Crucially, the scaphoid's vascular anatomy plays a definitive role in its propensity for nonunion and dictates our surgical approaches. Taleisnik and Kelly meticulously described the intraosseous blood supply, highlighting its retrograde nature. The primary vascular contributors are the laterovolar and dorsal vessels.
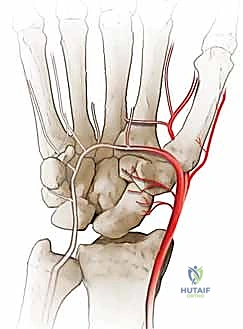
Figure 2A: Volar intraosseous blood supply to the scaphoid, demonstrating the laterovolar vessels entering distal to the waist.
The laterovolar vessels enter the scaphoid at the level of the distal third and waist, supplying the distal pole and the volar aspect of the waist. Because the intraosseous vascular network courses from distal to proximal, fractures at the waist or proximal pole critically disrupt the blood supply to the proximal fragment, leading to avascular necrosis (AVN) in up to 30-40% of proximal pole fractures.

Figure 2B: Dorsal intraosseous blood supply to the scaphoid, which enters via the dorsal ridge and supplies the proximal pole.
Ligamentous Constraints and Neurovascular Topography
The scaphoid is stabilized by a complex network of intrinsic and extrinsic ligaments that must be respected and, when necessary, meticulously repaired during surgical exposure. The extrinsic volar ligaments are thick, stout structures critical for carpal stability. The radioscaphocapitate (RSC) ligament is the most critical volar stabilizer. It originates from the radial styloid, courses over the waist of the scaphoid (acting as a fulcrum), and inserts onto the capitate. During a volar approach, the RSC must be carefully incised and meticulously repaired to prevent postoperative ulnar translation of the carpus. The long radiolunate (LRL) ligament lies ulnar to the RSC and provides essential support to the radiolunate articulation.
The intrinsic ligaments connect the carpal bones directly. The scapholunate (SL) interosseous ligament is the primary stabilizer of the proximal row. In a SNAC wrist, the SL ligament is typically intact, tethering the proximal scaphoid fragment to the lunate. This is a critical distinction from a SLAC wrist, where the SL ligament is ruptured. The scaphotrapezial-trapezoid (STT) ligaments connect the distal pole of the scaphoid to the distal carpal row. These are inherently sacrificed or released during a distal pole excision.
Navigating the neurovascular structures requires vigilance. The radial artery courses dorsally and radially through the anatomic snuffbox, giving off the dorsal carpal branch which supplies the dorsal scaphoid ridge. During a dorsal approach, this artery and its branches must be mobilized and protected. The superficial sensory branch of the radial nerve (SRN) crosses the surgical field superficially. It is highly susceptible to traction injury or iatrogenic transection, which can result in a debilitating, painful neuroma that often overshadows the benefits of the bony procedure. On the volar aspect, the Flexor Carpi Radialis (FCR) tendon serves as our primary surgical landmark. The FCR tendon sheath is incised, and the tendon is retracted ulnarly to expose the deep volar capsule. The median nerve lies ulnar to the FCR and is generally safely out of the operative field, provided retractors are placed judiciously.
Exhaustive Indications and Contraindications
Patient selection is the single most critical determinant of success in distal scaphoid pole excision. The typical patient is a young to middle-aged male laborer or athlete who sustained a hyperextension injury to the wrist months or years prior. They present with a history of chronic, deep, aching wrist pain that is exacerbated by heavy lifting, gripping, and forced extension. Progressive loss of motion, particularly in extension and radial deviation, is universally noted alongside a measurable decrease in grip strength.

Figure 4: Chronic nonunion of the scaphoid with advanced collapse in a patient with no previous surgical treatment.
Physical examination reveals localized tenderness within the anatomic snuffbox and over the STT joint volarly. A classic finding is a palpable dorsal fullness or a hard bony excrescence during palmar flexion, representing the hypertrophic, dorsally displaced distal scaphoid pole and associated reactive synovitis. Watson's scaphoid shift test may be positive, eliciting a painful clunk as the unstable proximal fragment subluxates over the dorsal rim of the radius, though this is often masked by severe stiffness and guarding.
Decision Matrix for Distal Pole Excision
The decision to proceed with distal pole excision rests on a precise understanding of the pathomechanics and the extent of arthritic progression. Below is a comprehensive matrix outlining the strict indications and absolute contraindications for this procedure.
| Parameter | Indications for Distal Pole Excision | Contraindications for Distal Pole Excision |
|---|---|---|
| Pathologic Stage | SNAC Stage I (Arthritis limited to radial styloid/distal pole). | SNAC Stage III or IV (Midcarpal or Pancarpal arthritis). |
| Alternative Pathology | Symptomatic scaphoid nonunion where bone grafting has failed or is deemed biologically futile (e.g., severe proximal pole AVN). | Scapholunate Advanced Collapse (SLAC) wrist. The proximal pole is unstable without the SL ligament. |
| Carpal Stability | Intact Scapholunate (SL) ligament. The proximal pole must remain congruous with the lunate. | Significant Ulnar Translocation of the carpus. |
| Patient Profile | Low to moderate demand patients; individuals seeking pain relief with preservation of functional, albeit limited, motion. | Heavy manual laborers requiring maximum grip strength (consider total wrist fusion instead). |
| Joint Status | Preserved capitolunate and radiolunate cartilage spaces on advanced imaging. | Active joint infection, severe osteopenia, or inflammatory arthropathy (e.g., Rheumatoid Arthritis). |
Distal pole excision is essentially an excisional arthroplasty. By removing the arthritic, impinging distal fragment, we eliminate the source of pain (the stylo-scaphoid impingement) and decompress the radioscaphoid joint. However, because the proximal fragment is left in situ, the SL ligament must be intact to prevent the remaining proximal scaphoid and lunate from collapsing into a severe, uncorrectable DISI deformity.
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning relies heavily on high-quality orthogonal imaging. Standard posteroanterior (PA), true lateral, and scaphoid-specific views (PA with ulnar deviation and slight extension) are mandatory. These plain radiographs are assessed for the presence and location of the nonunion, the degree of cystic resorption, and the specific location of osteophyte formation and joint space narrowing.
The true lateral radiograph is critical for assessing carpal alignment and measuring the degree of Dorsal Intercalated Segment Instability (DISI). The scapholunate angle is calculated by drawing a line down the longitudinal axis of the scaphoid and intersecting it with a line perpendicular to the distal articular surface of the lunate. A normal scapholunate angle ranges from 30 to 60 degrees. An angle exceeding 60 degrees, coupled with a radiolunate angle greater than 15 degrees of extension, confirms a significant DISI deformity.

Figure 5A: Lateral plain radiograph displaying a severe DISI deformity, characterized by an extended lunate and a flexed distal scaphoid fragment.
Advanced Imaging and Operative Preparation
While plain radiographs often suffice for the diagnosis of SNAC I, advanced imaging is highly recommended to confirm the absence of midcarpal arthritis, which would contraindicate the procedure. A non-contrast Computed Tomography (CT) scan with sagittal and coronal reconstructions is the gold standard for defining the exact bony architecture of the nonunion, quantifying the size of the proximal pole, and meticulously evaluating the capitolunate articulation for occult degenerative changes. Magnetic Resonance Imaging (MRI) is less critical for evaluating the arthritis but is highly sensitive for assessing the vascularity of the proximal pole; however, in the context of a planned distal excision, the viability of the proximal pole is less relevant than its structural integrity and ligamentous attachments.
Patient positioning is standardized but requires attention to detail. The patient is placed supine on the operating table with the affected extremity extended on a radiolucent hand table. A well-padded upper arm tourniquet is applied. Regional anesthesia (supraclavicular or axillary brachial plexus block) is the preferred modality, offering excellent intraoperative muscle relaxation and prolonged postoperative analgesia, which significantly reduces the need for systemic opioids. The arm is prepped and draped in a standard sterile fashion, ensuring exposure from the fingertips to the mid-forearm. Intraoperative fluoroscopy (C-arm) is brought into the field from the contralateral side or the head of the table, ensuring unobstructed AP and lateral imaging capabilities throughout the procedure.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of a distal scaphoid pole excision can be performed via a dorsal or a volar approach. The choice often depends on the exact location of the nonunion and the surgeon's preference. However, the volar approach (modified Russe) is highly favored as it provides direct, unparalleled access to the distal pole, the STT joint, and allows for excellent visualization of the volar radioscaphocapitate (RSC) ligament, which must be protected.
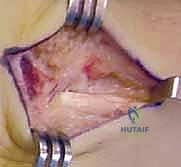
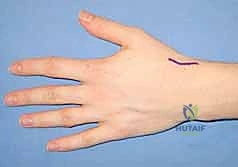
The Volar Approach and Deep Dissection
An 8-cm longitudinal or slightly curvilinear incision is made over the volar aspect of the wrist, centered over the Flexor Carpi Radialis (FCR) tendon, extending from the distal wrist crease proximally.