

Comprehensive Introduction and Patho-Epidemiology
The distal radioulnar joint (DRUJ) is a highly specialized, diarthrodial articulation that, in conjunction with the proximal radioulnar joint, dictates the intricate biomechanics of forearm pronation and supination. Unlike a simple hinge, the DRUJ undergoes a complex combination of rotation and translation during motion. The radius arcs around the fixed ulna, a movement stabilized by an intricate network of soft tissues, most notably the triangular fibrocartilage complex (TFCC). When this delicate biomechanical balance is disrupted by trauma, inflammatory arthropathy, or degenerative osteoarthritis, the resulting pain, weakness, and instability can profoundly diminish a patient's functional capacity and quality of life. Ulnar head implant arthroplasty has emerged as a sophisticated, highly effective intervention designed to restore this anatomical relationship and salvage forearm kinematics.

Historically, the surgical management of the irreparably damaged DRUJ relied heavily on ablative procedures. Techniques such as the Darrach procedure (distal ulnar resection) or the Sauvé-Kapandji procedure (distal radioulnar arthrodesis with proximal ulnar pseudoarthrosis) were mainstays. However, while these procedures often successfully eliminated bone-on-bone crepitus, they frequently introduced a secondary, arguably more debilitating pathology: radioulnar convergence. Without the structural buttress of the ulnar head, the distal ulnar stump is subjected to unresisted muscular forces from the pronator quadratus and the brachioradialis, causing it to dynamicially impinge against the radial metaphysis.
This phenomenon, clinically recognized as painful ulnar stump impingement syndrome, is characterized by a narrow radioulnar distance on radiographs, profound loss of grip strength, and intractable pain during load-bearing rotation. The ulnar stump effectively acts as a pestle grinding against the radial mortar, leading to progressive cortical erosion and soft tissue attenuation. For decades, the orthopedic community struggled with the "failed Darrach," attempting soft tissue interpositions and tenodeses with universally disappointing long-term survivorship. The advent of modern ulnar head arthroplasty represented a paradigm shift, moving away from ablation and toward anatomical restoration.
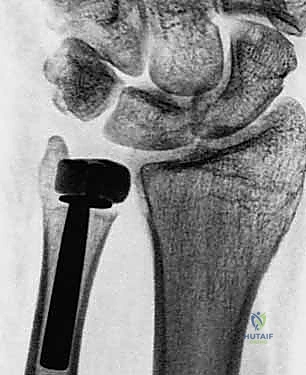
Early attempts at prosthetic replacement utilized silicone capping, which failed predictably due to particulate synovitis and catastrophic mechanical failure under the immense shear forces generated across the DRUJ. Contemporary implant arthroplasty, utilizing highly polished cobalt-chrome, titanium, or pyrocarbon prostheses, aims to anatomically replicate the ulnar head. By restoring the spatial relationship between the radius and ulna, these implants tension the interosseous membrane, restore the functional length of the forearm musculature, and provide a stable fulcrum for rotation. Mastery of this procedure requires not only technical precision in bone preparation but an exhaustive understanding of the surrounding soft tissue envelope, which must be meticulously reconstructed to ensure implant stability and longevity.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of distal forearm anatomy is the absolute prerequisite for successful DRUJ arthroplasty. The osteology of the DRUJ is characterized by a mismatch in the radii of curvature between the ulnar head and the sigmoid notch of the radius. The ulnar head is not a perfect sphere; it is slightly asymmetrical, articulating with the shallow, concave sigmoid notch. This inherent bony incongruity means that the DRUJ is inherently unstable relying almost entirely on extrinsic soft tissue stabilizers. The sigmoid notch itself exhibits variable version (volar, dorsal, or neutral) and inclination, which must be critically evaluated on preoperative axial imaging to determine if a simple hemiarthroplasty will suffice or if the notch requires concurrent resurfacing or a constrained total joint system.

The primary stabilizer of the DRUJ is the Triangular Fibrocartilage Complex (TFCC). This is not a singular ligament but a complex, multi-layered structure comprising the articular disc, the dorsal and volar radioulnar ligaments, the ulnocarpal ligaments (ulnolunate and ulnotriquetral), and the extensor carpi ulnaris (ECU) subsheath. The critical stabilizing components are the deep (ligamentum subcruentum) and superficial fibers of the radioulnar ligaments. The deep fibers insert directly into the fovea—a distinct depression at the base of the ulnar styloid—while the superficial fibers attach to the tip of the styloid. During ulnar head replacement, preserving or anatomically reconstructing this foveal footprint is paramount to preventing postoperative prosthesis subluxation.
Secondary stabilizers include the interosseous membrane (IOM), specifically the distal oblique bundle (DOB), and the dynamic muscular forces of the pronator quadratus and ECU. The ECU tendon, housed within its distinct fibro-osseous tunnel (the sixth dorsal compartment), acts as a dynamic restraint to dorsal translation of the ulnar head during supination. When performing the surgical exposure, the ECU subsheath must be meticulously preserved or robustly repaired. Failure to tension the ECU subsheath appropriately will lead to recurrent dorsal instability of the implant, a common and frustrating complication that often necessitates revision surgery.
Neurovascular anatomy dictates our surgical corridors. The most critical structure at risk during the ulnar border approach is the dorsal sensory branch of the ulnar nerve (DSBUN). This nerve typically branches from the main ulnar nerve approximately 5 to 8 centimeters proximal to the pisiform, traveling dorsally deep to the flexor carpi ulnaris (FCU) before piercing the deep fascia to provide sensation to the dorsoulnar aspect of the hand. Its anatomical course is highly variable, and it frequently crosses the surgical field directly over the distal ulna. Iatrogenic injury to the DSBUN results in a debilitating, recalcitrant neuroma that can render a technically perfect arthroplasty a clinical failure. Meticulous blunt dissection, loop magnification, and absolute respect for the subcutaneous tissues are mandatory.
Exhaustive Indications and Contraindications
The decision to proceed with ulnar head implant arthroplasty requires a nuanced synthesis of the patient's clinical presentation, functional demands, and radiographic findings. The primary goal is pain relief, followed closely by the restoration of stable forearm rotation and grip strength. Patient selection is critical; this is a salvage procedure designed for complex pathology, not a first-line treatment for mild, manageable osteoarthritis. A thorough understanding of the indications and absolute contraindications will prevent catastrophic implant failures and ensure optimal clinical outcomes.

The most robust indication for unconstrained ulnar head hemiarthroplasty is symptomatic radioulnar convergence following a prior distal ulnar resection (e.g., failed Darrach or matched resection). In these patients, the loss of the ulnar fulcrum leads to dynamic impingement of the ulnar stump against the radius, causing severe pain during lifting and rotation. Primary degenerative osteoarthritis of the DRUJ, post-traumatic arthrosis (often secondary to malunited distal radius fractures with severe DRUJ incongruity), and well-controlled rheumatoid arthritis with preserved bone stock represent other primary indications. In cases of primary arthropathy, joint-preserving procedures such as arthroscopic debridement or wafer resections must have been exhausted or deemed anatomically inappropriate prior to considering arthroplasty.
Contraindications must be strictly observed. Absolute contraindications include active or latent deep infection, severe uncorrectable radiocarpal instability, and a complete absence of a viable soft tissue envelope (specifically the lack of a functional ECU or irreparable capsuloligamentous structures). If the soft tissue envelope is incompetent, an unconstrained hemiarthroplasty will inevitably dislocate; in such scenarios, a constrained total DRUJ replacement (e.g., the Aptis implant) is the only viable arthroplasty option. Furthermore, significant destruction, severe dysplasia, or advanced erosive changes of the radial sigmoid notch preclude isolated ulnar head replacement, as the implant will rapidly wear through the compromised radial bone.
| Category | Indications for Unconstrained Arthroplasty | Contraindications (Absolute & Relative) |
|---|---|---|
| Primary Pathology | Primary DRUJ Osteoarthritis (advanced) | Active local or systemic infection |
| Post-Surgical | Failed Darrach procedure (ulnar impingement) | Incompetent soft tissue envelope (requires constrained total joint) |
| Trauma | Post-traumatic arthrosis (DRUJ incongruity) | Severe sigmoid notch destruction/dysplasia |
| Inflammatory | Rheumatoid Arthritis (well-controlled, good bone stock) | Uncorrectable radiocarpal or carpal instability |
| Anatomical | Irreparable ulnar head fractures | Skeletal immaturity |
| Neurological | Intact regional motor control | Charcot arthropathy or severe neurocognitive deficit |
Pre-Operative Planning, Templating, and Patient Positioning
Preoperative planning is the crucible in which the success of the arthroplasty is forged. Clinical evaluation must isolate DRUJ pathology from concomitant wrist disorders. The "piano key" sign (dorsal ballotment of the ulnar head) indicates gross instability, while the radioulnar compression test—where the examiner squeezes the radius and ulna together while rotating the forearm—will elicit severe pain in the presence of arthrosis or impingement. Grip strength testing using a Jamar dynamometer in varying positions of forearm rotation provides a quantifiable baseline for postoperative comparison.
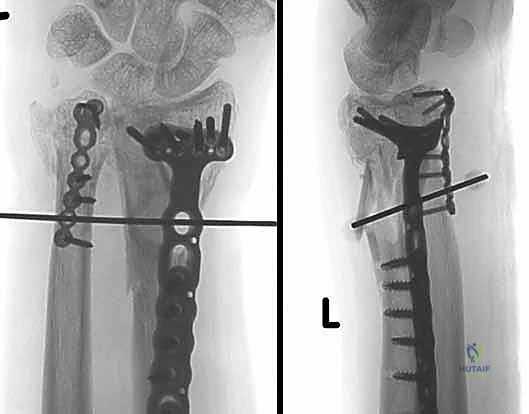
Imaging requires a meticulously standardized protocol. A true "zero-rotation" posteroanterior (PA) radiograph of the wrist, taken with the shoulder abducted 90 degrees and the elbow flexed 90 degrees, is mandatory to accurately assess ulnar variance. A true lateral radiograph is required to evaluate dorsal or volar subluxation. Furthermore, stress-loaded PA views—where the patient grips a 2.2-kg weight—are invaluable for unmasking dynamic radioulnar convergence in cases of suspected impingement. High-resolution computed tomography (CT) is strongly recommended, not just for the affected wrist, but for the contralateral normal wrist. Axial CT slices allow for precise measurement of the sigmoid notch version, depth, and the presence of osteophytes, dictating whether the notch can accept a hemiarthroplasty or requires resurfacing.

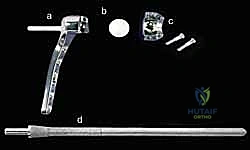
Templating is performed using digital software calibrated to the radiographic markers. The goal is to restore neutral ulnar variance and replicate the native center of rotation. We size the ulnar head implant to match the diameter of the native head (or the contralateral head if the native anatomy is destroyed). The intramedullary stem size is determined by evaluating the isthmus of the distal ulna. If the patient has had a prior Darrach resection, an extended-collar implant may be necessary to compensate for the resected bone and restore appropriate myofascial tension to the interosseous membrane.

Patient positioning must facilitate unhindered access and excellent fluoroscopic visualization. The patient is placed supine with the operative extremity extended onto a radiolucent hand table. A pneumatic tourniquet is applied to the proximal arm. Crucially, the C-arm fluoroscope should be brought in parallel to the hand table, allowing the surgeon to obtain true AP and lateral images simply by rotating the patient's forearm, rather than maneuvering the heavy C-arm during critical steps of the procedure. Standard sterile prep and drape are applied, ensuring the entire forearm up to the tourniquet is exposed to allow for assessment of dynamic rotation during trial reduction.
Step-by-Step Surgical Approach and Fixation Technique
Partial Ulnar Head Replacement Arthroplasty (Dorsal Approach)
This approach is indicated when the disease process, typically localized arthritis, is limited to the distal ulnar articular surface, and we aim to preserve the ulnar styloid and the deep foveal attachment of the TFCC.

- Incision and Exposure: A longitudinal skin incision is made directly in line with the fourth metacarpal, extending proximally about 5-6 cm from the radiocarpal joint line. After careful subcutaneous dissection, the extensor retinaculum overlying the fourth dorsal compartment is identified and divided longitudinally. The extensor digiti minimi (EDM) and the extensor digitorum communis (EDC) tendons are retracted to expose the dorsal capsule of the DRUJ.
- Capsulotomy and Joint Assessment: An ulnar-based, robust capsular flap is elevated, preserving the dorsal radioulnar ligament distally. This exposes the articular portion of the ulnar head. The joint is inspected, and the integrity of the TFCC is probed. If the foveal attachment is intact, the partial head replacement can proceed.
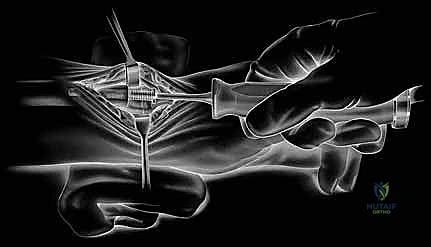
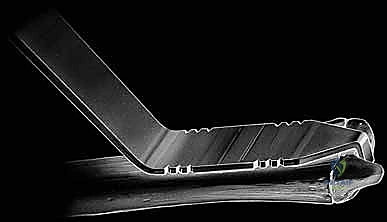
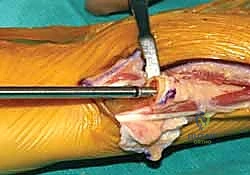
- Ulnar Head Resection: Using a customized jig specific to the implant system, precisely resect the articular dome of the ulnar head. The guide wire is placed centrally into the ulnar head, parallel to the ulnar shaft. A cannulated reamer is then used to remove the articular cartilage and subchondral bone, creating a flat surface that will interface seamlessly with the collar of the prosthesis. Extreme care must be taken during this step to protect the ulnar styloid and the attached TFCC footprint from the reamer.
- Preparation and Trialing: The ulnar canal is sequentially broached to accept the stem of the implant. A trial implant is inserted. The DRUJ is reduced, and the forearm is taken through a full, dynamic range of pronation and supination. The surgeon must meticulously assess for impingement against the sigmoid notch, overstuffing of the joint, and stability throughout the arc of motion. Fluoroscopy confirms correct implant depth and neutral ulnar variance.
- Final Implantation and Closure: Once the correct size is confirmed, the definitive implant (often press-fit, though cement may be used in osteoporotic bone) is impacted into place. The dorsal capsule is meticulously repaired using non-absorbable sutures to prevent dorsal subluxation. The extensor retinaculum is repaired, leaving the EDM superficial to the retinaculum to prevent postoperative bowstringing or tendon rupture.
Unconstrained Hemiarthroplasty (Ulnar Border Approach)
For patients requiring complete ulnar head replacement, particularly those with a failed Darrach procedure, the ulnar border approach provides optimal access for both bony preparation and complex soft-tissue reconstruction.

- Incision and Neuroma Prevention: A 7-8 cm longitudinal incision is made along the subcutaneous border of the distal ulna. The dissection proceeds carefully through the subcutaneous tissues. The dorsal sensory branch of the ulnar nerve (DSBUN) must be immediately identified, mobilized, and protected with a vessel loop. This is arguably the most critical step of the exposure; careless retraction here will result in a disastrous postoperative pain syndrome.

- Interval Development: The interval between the flexor carpi ulnaris (FCU) and the extensor carpi ulnaris (ECU) is developed. The ECU subsheath is incised longitudinally, leaving a robust ulnar cuff for later repair. The distal ulnar shaft (or the residual stump in a revision case) is skeletonized subperiosteally. Any heterotopic ossification or fibrotic scar tissue from previous surgeries is meticulously excised to mobilize the radius and ulna.

- Bone Preparation: The distal ulna is resected at the pre-planned level using an oscillating saw. The medullary canal is identified and sequentially broached. It is imperative to maintain proper rotational alignment of the broach to ensure the asymmetrical head of the final implant correctly articulates with the sigmoid notch. Trial components are inserted.

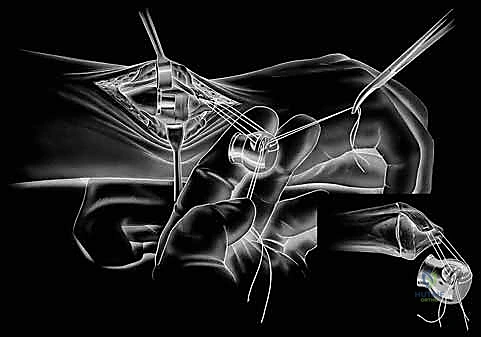
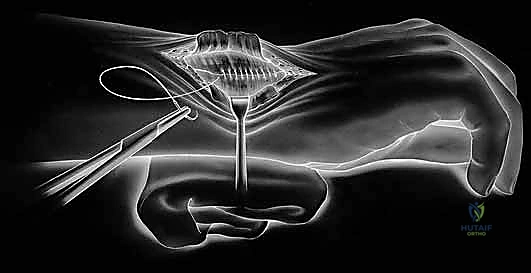
- Soft Tissue Reconstruction (The Crux of the Procedure): If the TFCC is completely absent, stability relies entirely on reconstructing the capsuloligamentous envelope. Drill holes are placed in the dorsal and volar cortex of the distal radius. Heavy non-absorbable sutures or suture anchors are utilized to imbricate the remaining capsule and the ECU subsheath over the implant. The trial is reduced, and stability is assessed. If dorsal instability persists, an ECU tenodesis or a slip of the FCU may be routed around the ulnar neck to act as a dynamic sling.

- Final Implantation: Once absolute stability is achieved with the trials, the true implant is inserted. The soft tissue reconstruction is tied down with the forearm held in neutral rotation. The ECU tendon must be stabilized within its subsheath to prevent volar subluxation during supination. The wound is closed in layers over a closed suction drain to prevent hematoma formation.

Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, DRUJ arthroplasty carries a distinct complication profile. The most frequent and challenging complication is postoperative instability, specifically dorsal subluxation of the implant during forearm supination. This typically stems from an unrecognized incompetence of the ECU subsheath, failure to adequately tension the dorsal capsule, or an inherent mismatch between the implant and a dysplastic sigmoid notch. Early instability may require revision soft tissue reconstruction, while chronic instability often necessitates conversion to a constrained total DRUJ prosthesis.
Neurologic complications, primarily involving the DSBUN, occur in up to 10% of cases depending on the series. Symptoms range from transient neuropraxia due to retractor pressure to severe, intractable neuroma pain from direct laceration. Management of a true neuroma involves surgical exploration, resection of the neuroma, and burying the proximal nerve stump deep into the pronator quadratus muscle belly. Aseptic loosening and implant subsidence are less common with modern press-fit stems but can occur, particularly in osteoporotic bone or if the implant is undersized. Symptomatic loosening requires revision to a larger stemmed implant or cemented fixation.

Periprosthetic fractures can occur intraoperatively during aggressive broaching of a narrow ulnar canal or postoperatively secondary to trauma. Intraoperative fractures must be recognized immediately and managed with cerclage wiring or a longer-stemmed implant that bypasses the fracture site. Infection, while rare (<2%), is devastating and requires standard principles of explantation, aggressive serial debridement, placement of an antibiotic spacer, and delayed reconstruction once the infection is definitively cleared.

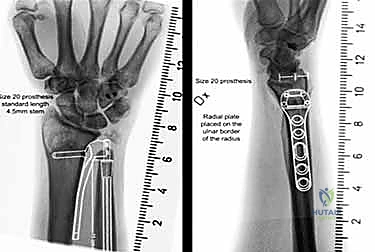
When unconstrained hemiarthroplasty fails irretrievably—due to severe instability, massive bone loss, or sigmoid notch destruction—salvage options are limited but critical. The gold standard salvage is conversion to a constrained total DRUJ replacement (e.g., the Aptis system), which relies on a radial plate and a captured ulnar sphere, bypassing the need for a competent soft tissue envelope. Alternatively, a one-bone forearm procedure (creation of a radioulnar synostosis with proximal ulnar resection) can provide a stable, painless limb, albeit at the absolute sacrifice of all forearm rotation.

| Complication | Estimated Incidence | Primary Etiology | Management / Salvage Strategy |
|---|---|---|---|
| Dorsal Instability | 5 - 15% | ECU subsheath failure, capsular laxity |
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding ulnar-head-implant-arthroplasty