Masterclass: Extra-articular Reconstruction for DRUJ and Ulnocarpal Instability

Key Takeaway
This masterclass provides an immersive, step-by-step guide to extra-articular distal radioulnar joint (DRUJ) and ulnocarpal reconstruction. We'll meticulously detail the Modified Herbert and Hui-Linscheid techniques, covering comprehensive surgical anatomy, precise intraoperative execution, critical pearls and pitfalls, and essential postoperative management for optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
The distal radioulnar joint (DRUJ) and the ulnocarpal articulation represent a marvel of biomechanical engineering, functioning synergistically to permit fluid pronosupination while simultaneously transferring substantial axial loads across the wrist. The intrinsic stability of this complex region relies heavily on the structural integrity of the triangular fibrocartilage complex (TFCC), a multifaceted soft-tissue network that acts as the primary stabilizer of the ulnar carpus and the DRUJ. When this delicate equilibrium is disrupted—whether through acute traumatic insult, such as a fall on an outstretched hand (FOOSH), or via insidious degenerative attrition—the resulting instability frequently precipitates chronic, debilitating ulnar-sided wrist pain, profound grip weakness, and severe functional limitation.
Historically, the management of chronic DRUJ and ulnocarpal instability has posed a formidable challenge to orthopedic and hand surgeons. While acute peripheral TFCC tears are often amenable to direct arthroscopic or open repair, chronic instability with attenuated, retracted, or biologically compromised native tissues demands a more robust reconstructive strategy. Extra-articular reconstructions, specifically the Modified Herbert reconstruction and the Hui-Linscheid procedure, have emerged as indispensable techniques in the surgeon's armamentarium. These procedures bypass the compromised intra-articular structures, utilizing autologous local tissues to recreate the essential stabilizing vectors and restore the ligamentotaxic constraint necessary for physiologic kinematics.
The epidemiology of ulnocarpal instability demonstrates a bimodal distribution, frequently affecting young, high-demand athletes following acute rotational trauma, as well as older individuals suffering from degenerative conditions such as rheumatoid arthritis or ulnar impaction syndrome. The pathogenesis is fundamentally rooted in the failure of the radioulnar ligaments and the ulnocarpal suspension mechanism. As the primary stabilizers yield, secondary stabilizers—such as the extensor carpi ulnaris (ECU) subsheath and the interosseous membrane—are subjected to unphysiologic loads, eventually leading to a cascading failure of the entire ulnar-sided stabilizing envelope. Recognizing this cascade is paramount for selecting the appropriate reconstructive intervention.
In authoring this definitive masterclass, our objective is to provide an exhaustive, technically rigorous exposition of extra-articular reconstructive techniques for the DRUJ and ulnocarpal joint. We will dissect the intricate surgical anatomy, outline precise preoperative templating protocols, and detail the step-by-step execution of these complex procedures. By mastering these extra-articular techniques, the reconstructive surgeon can reliably restore stability, alleviate chronic pain, and salvage function in wrists that might otherwise be relegated to salvage procedures such as the Darrach or Sauvé-Kapandji operations.
Detailed Surgical Anatomy and Biomechanics
Before initiating any surgical incision, an absolute, three-dimensional mastery of the ulnar wrist anatomy is mandatory. The ulnar aspect of the wrist is a densely packed, unforgiving anatomical zone where critical neurovascular structures are intimately associated with intricate tendinous and ligamentous networks. Any deviation from precise anatomical planes can result in catastrophic iatrogenic injury or catastrophic failure of the reconstruction.
The Triangular Fibrocartilage Complex Architecture
The TFCC is the indisputable cornerstone of stability for both the DRUJ and the ulnocarpal joint. It is imperative to conceptualize the TFCC not as a singular, monolithic structure, but rather as a highly specialized, heterogeneous collection of soft tissues working in concert. The triangular fibrocartilage proper (articular disc) originates from the hyaline cartilage of the sigmoid notch of the radius and projects ulnarly to insert into the base of the ulnar styloid and the fovea. This central disc provides a continuous, frictionless gliding surface for the carpus but contributes minimally to tensile stability.

The true mechanical stabilizers are the dorsal and palmar radioulnar ligaments (DRUL and PRUL), which border the articular disc. These marginal ligaments possess both superficial (inserting on the ulnar styloid) and deep (inserting on the fovea) fibers. Biomechanical studies have definitively shown that the deep foveal fibers represent the true isometric axis of forearm rotation. Furthermore, the ulnocarpal ligaments—specifically the ulnolunate and ulnotriquetral ligaments—originate from the palmar aspect of the TFCC and suspend the ulnar carpus from the ulnar head, preventing volar subluxation of the carpus during dynamic loading.
Crucially, the surgeon must understand that the ulnar carpus does not directly articulate with the osseous distal ulna; it is entirely suspended by the TFCC. This sling-like suspension mechanism is vital for its load-transferring capabilities, cushioning the carpus and transmitting approximately 20% of the axial load through the ulnar shaft under normal variance. The ECU subsheath, a robust fibrous tunnel, intimately blends with the dorsal aspect of the TFCC, providing dynamic stability to the DRUJ during active forearm rotation and ECU contraction.
The Extensor Retinaculum and Compartmental Anatomy
The extensor retinaculum is a thick, unyielding fibrous band that plays a central role in extra-articular reconstructive procedures, particularly the Modified Herbert technique. Its anatomical orientation is not strictly transverse; rather, it courses in a radial-proximal to ulnar-distal direction. Medially, it anchors firmly to the pisiform and triquetrum, while laterally, it attaches to the lateral margin of the radius. This oblique orientation is critical to understand when harvesting retinacular flaps, as it dictates the functional vector of the resulting reconstruction.
Deep to the extensor retinaculum lie the six extensor compartments of the wrist, each separated by vertical septa that insert onto the dorsal radius and ulna. For the procedures discussed herein, the surgeon's focus is primarily directed toward the fourth, fifth, and sixth compartments. The fifth compartment, housing the extensor digiti minimi (EDM), frequently serves as the primary landmark for our initial surgical approach. The sixth compartment, containing the ECU, is intimately involved in ulnar-sided pathology and is often utilized as a graft source in the Hui-Linscheid procedure.
The retinaculum is continuous distally with the palmar carpal ligament and shares connecting fibers with the flexor retinaculum proximal to the pisiform. This continuity implies that tensioning a dorsal retinacular flap will inevitably influence the palmar carpal dynamics. Furthermore, the dorsal cutaneous branch of the ulnar nerve (DCBUN) reliably crosses the surgical field dorsally, typically emerging from beneath the flexor carpi ulnaris (FCU) approximately 5 cm proximal to the ulnar styloid, and arborizing over the ulnar carpus. Meticulous identification and protection of this nerve are non-negotiable.
Relevant Osteology and Kinematics
The osseous architecture of the DRUJ is inherently unstable. The sigmoid notch of the distal radius possesses a radius of curvature significantly larger (approximately 15 mm) than that of the articulating ulnar head (approximately 10 mm). This geometric mismatch results in a joint that is highly dependent on soft-tissue constraints for stability, functioning more as a sliding and pivoting articulation rather than a highly congruent ball-and-socket or hinge joint.
During pronosupination, the radius rotates around a relatively fixed ulna. The ulnar head translates volarly during supination and dorsally during pronation within the sigmoid notch. Consequently, the stabilizing ligaments experience differential tensioning throughout the arc of motion. The palmar radioulnar ligament tightens in supination, preventing dorsal subluxation of the ulna, while the dorsal radioulnar ligament tightens in pronation, preventing volar subluxation.
The distal ulna features critical landmarks for reconstructive surgery: the ulnar styloid, the fovea (the depression at the base of the styloid), and the articular circumference of the ulnar head. When executing a Hui-Linscheid reconstruction, drill holes must be precisely placed through the distal ulna to recreate the isometric origins of the radioulnar ligaments. Similarly, understanding the spatial relationship between the pisiform, triquetrum, and the ulnar styloid is essential for establishing the correct tensioning vectors during the Modified Herbert retinacular flap advancement.
Exhaustive Indications and Contraindications
The decision to proceed with an extra-articular reconstruction of the DRUJ and ulnocarpal joint must be predicated on a rigorous clinical and radiographic evaluation. These procedures are not prophylactic; they are definitive salvage operations for symptomatic, chronic instability that has proven refractory to exhaustive conservative management. The ideal candidate is a patient with debilitating ulnar-sided wrist pain, demonstrable mechanical instability (e.g., clicking, clunking, or subjective giving-way), and a significant reduction in grip strength and pronosupination torque.
Primary indications include chronic, irreparable peripheral tears of the TFCC resulting in gross DRUJ instability. This is often clinically manifested by a positive "piano key" sign or gross translation during the supination test. Additionally, patients with isolated ulnocarpal instability—where the carpus supinates and sags volarly away from the distal ulna due to attenuation of the ulnolunate and ulnotriquetral ligaments—are excellent candidates. These procedures are also highly effective in cases of dynamic ECU snapping caused by a deficient ECU subsheath, provided there is concomitant underlying DRUJ or ulnocarpal laxity that requires stabilization.
Conversely, absolute contraindications must be respected to prevent catastrophic surgical failures. The most critical contraindication is the presence of advanced, fixed osteoarthritis of the DRUJ or the ulnocarpal joint. Extra-articular reconstructions rely on a functional, cartilage-preserved joint space; tightening a severely arthritic joint will only exacerbate pain and severely restrict motion. In such instances, salvage arthroplasty (e.g., ulnar head replacement) or ablative procedures (e.g., Darrach or Sauvé-Kapandji) are the standard of care.
Furthermore, severe, uncorrected carpal instability (such as a fixed Dorsal Intercalated Segment Instability [DISI] or Volar Intercalated Segment Instability [VISI]) represents a relative contraindication. The altered carpal kinematics will place unphysiologic stress on the extra-articular reconstruction, leading to rapid attenuation and failure of the graft or retinacular flap. Active local or systemic infection, severe osteopenia precluding secure osseous fixation, and profound patient non-compliance regarding postoperative rehabilitation are also absolute contraindications.
| Category | Specific Conditions | Rationale for Inclusion/Exclusion |
|---|---|---|
| Primary Indications | Chronic, irreparable peripheral TFCC tears | Native tissue is insufficient for direct repair; requires extra-articular constraint. |
| Symptomatic ulnocarpal instability | Restores the suspension sling of the ulnar carpus, alleviating pain and weakness. | |
| Recurrent ECU tendon subluxation with DRUJ laxity | Addresses both the dynamic tendon snapping and the underlying joint instability. | |
| Absolute Contraindications | Advanced DRUJ or ulnocarpal osteoarthritis | Reconstructing ligaments across an arthritic joint exacerbates pain and stiffness. |
| Active local or systemic infection | High risk of deep space infection and catastrophic failure of the reconstruction. | |
| Relative Contraindications | Uncorrected global carpal instability (DISI/VISI) | Altered mechanics will subject the reconstruction to premature failure and attenuation. |
| Severe osteopenia / osteoporosis | Prevents secure fixation of grafts within osseous tunnels (relevant for Hui-Linscheid). |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the bedrock of successful extra-articular reconstruction. The surgeon must synthesize data from the clinical examination, advanced imaging, and intraoperative dynamic assessments to tailor the specific reconstructive technique (Modified Herbert vs. Hui-Linscheid) to the patient's unique pathoanatomy.
Clinical Examination and Advanced Imaging Modalities
The physical examination must be exhaustive. Visual inspection often reveals a subtle ulnar-sided supination deformity or prominent ulnar head. Palpation should precisely localize tenderness—whether over the DRUJ, the fovea, or the ulnocarpal interval. Provocative maneuvers are critical: the Piano Key Test assesses DRUJ stability, while the Supination Test is the diagnostic hallmark for ulnocarpal instability. During the Supination Test, the examiner firmly stabilizes the DRUJ and stresses the wrist in supination and volar translation; reproduction of pain or a palpable "clunk" confirms the diagnosis.
Standard posteroanterior (PA) and lateral radiographs are mandatory to evaluate ulnar variance, rule out fractures, and assess for degenerative changes. However, standard static radiographs are often insufficient for diagnosing dynamic ligamentous instability. Computed Tomography (CT), particularly in bilateral pronation and supination views, is excellent for quantifying DRUJ subluxation and assessing the congruity of the sigmoid notch.
Magnetic Resonance Arthrography (MRA) is the imaging modality of choice for evaluating the soft tissues of the ulnar wrist. MRA provides superior sensitivity and specificity for detecting peripheral TFCC tears and ulnocarpal ligament attenuation compared to standard MRI. Furthermore, live fluoroscopy combined with the Supination Test provides invaluable dynamic visualization. As the wrist is supinated, the surgeon can observe the triquetrum's changing spatial relationship and the widening of the ulnocarpal interval, definitively confirming the instability pattern.


Patient Positioning and Operating Room Setup
Proper patient positioning and operating room setup are essential for facilitating seamless surgical execution and optimal intraoperative imaging. The patient is placed in the supine position on a standard operating table equipped with a specialized radiolucent hand table extension. General anesthesia is typically employed, supplemented by a regional block (e.g., supraclavicular or axillary brachial plexus block) to ensure profound intraoperative muscle relaxation and excellent postoperative analgesia.
The affected upper extremity is placed on the arm board with the elbow flexed to approximately 45 degrees. The forearm is initially positioned in full pronation. This pronated posture is mechanically advantageous; it naturally reduces the DRUJ in most patterns of instability and provides optimal, unimpeded exposure to the dorsal aspect of the wrist. A well-padded pneumatic tourniquet is applied high on the brachium and inflated to standard upper extremity pressures after exsanguination with an Esmarch bandage.
The entire arm, from the tourniquet margin down to the fingertips, is meticulously prepped and draped in a standard sterile fashion. A sterile C-arm fluoroscopy unit must be readily available and positioned perpendicular to the hand table. The C-arm should be capable of effortlessly swinging between anteroposterior (AP) and true lateral projections without compromising the sterile field. Intraoperative fluoroscopy is not merely for documentation; it is a critical tool used repeatedly throughout the procedure to confirm joint reduction, verify drill hole trajectories, and dynamically assess the tensioning of the reconstruction.
Step-by-Step Surgical Approach and Fixation Technique
The execution of extra-articular reconstructions demands meticulous soft-tissue handling, precise spatial awareness, and a deep understanding of wrist kinematics. We will detail the operative steps for both the Modified Herbert Reconstruction, which utilizes a retinacular flap, and the Hui-Linscheid procedure, which relies on tendon grafting.
The Modified Herbert Reconstruction
The Modified Herbert reconstruction is an elegant procedure designed to stabilize the DRUJ and ulnocarpal joint by creating an ulnar-based flap of the extensor retinaculum. This flap is subsequently routed and advanced in a distal-ulnar to radial-proximal direction, creating a dynamic sling that provides robust ligamentotaxic constraint against volar and ulnar sagging of the carpus.
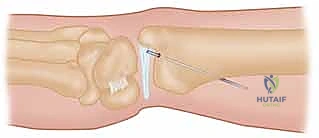
Incision and Superficial Dissection:
The procedure commences with a precise longitudinal incision, approximately 4 to 5 cm in length, centered directly over the palpable fifth extensor compartment at the level of the radiocarpal joint.
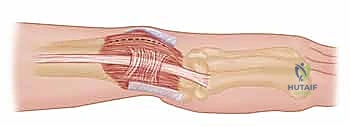
As the incision is deepened through the subcutaneous tissues, the surgeon must exercise extreme vigilance to identify and protect the dorsal cutaneous branch of the ulnar nerve (DCBUN). The DCBUN frequently arborizes across this exact surgical field. Using fine blunt dissection with Metzenbaum scissors, the nerve branches are carefully mobilized and retracted using vessel loops. Iatrogenic injury to the DCBUN will result in debilitating postoperative neuropathic pain, often overshadowing the functional success of the joint reconstruction.
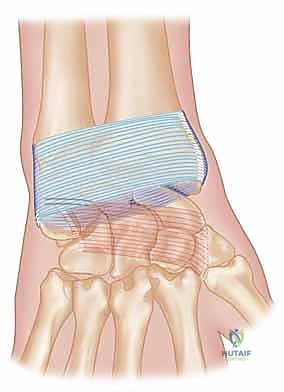
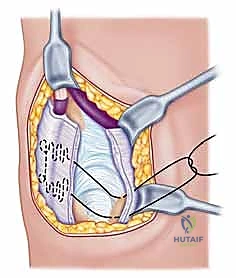
Retinacular Flap Creation:
Once the extensor retinaculum is exposed, the borders of the fifth compartment (housing the EDM) and the sixth compartment (housing the ECU) are clearly delineated. A distally based, rectangular flap of the extensor retinaculum is meticulously elevated. The radial incision for the flap is made along the septum separating the fourth and fifth compartments, while the ulnar incision is made along the ulnar border of the sixth compartment.

The flap is elevated from proximal to distal, leaving its robust distal attachment securely anchored to the triquetrum and pisiform. This preserves the essential ulnocarpal continuity required for the reconstruction. The EDM and ECU tendons are now visible and can be inspected for any concomitant pathology, such as tenosynovitis or subluxation.
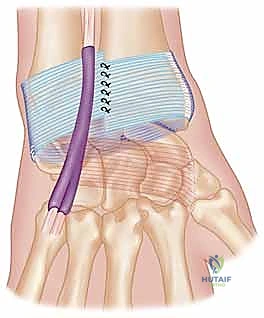
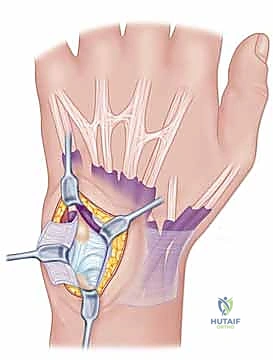
Routing and Ligamentotaxic Tensioning:
The critical step involves routing the distally based retinacular flap to recreate the stabilizing vector. The flap is passed deep to the ECU tendon—acting as a sling to stabilize the tendon and reinforce the deficient subsheath—and is then pulled proximally and radially.
While an assistant holds the forearm in neutral rotation and applies a dorsally directed force to the pisiform (reducing the ulnocarpal sag), the surgeon tensions the retinacular flap. The proximal end of the flap is firmly sutured to the dorsal radioulnar ligament remnant or directly to the dorsal rim of the sigmoid notch using heavy, non-absorbable braided sutures (e.g., #2-0 FiberWire or equivalent).

This precise vector of tension effectively translates the ulnar carpus dorsally and radially, reducing the DRUJ and restoring the ulnocarpal suspension. Intraoperative fluoroscopy is utilized to confirm the reduction of the DRUJ in both pronation and supination before final knot tying.
The Hui-Linscheid Procedure
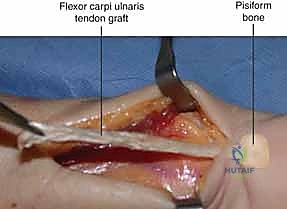
For instances where the extensor retinaculum is insufficient, or greater structural rigidity is demanded, the Hui-Linscheid procedure is employed. This technique utilizes a tendon graft—typically a split strip of the FCU or ECU—routed through osseous tunnels in the distal ulna to anatomically reconstruct the radioulnar and ulnocarpal ligaments.
Tendon Harvest and Preparation:
An extended ulnar incision is utilized to expose both the distal ulna and the harvest site. If the ECU is selected, a distally based, half-thickness strip of the tendon is harvested, leaving its insertion on the base of the fifth metacarpal intact.


The graft is tubularized using a running locking stitch with a #4-0 absorbable suture to facilitate smooth passage through the osseous tunnels.
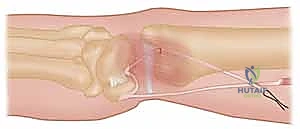
Osseous Tunnels and Graft Routing:
Precise creation of the osseous tunnels is the most technically demanding aspect of the Hui-Linscheid procedure. Using fluoroscopic guidance, a guide pin is driven from the dorsal aspect of the ulnar neck, exiting precisely at the anatomical fovea (the isometric center of rotation). A 3.0 mm or 3.5 mm cannulated drill bit is then passed over the guide pin to create the tunnel.
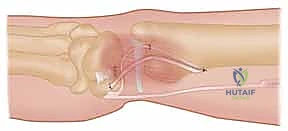

The prepared tendon graft is subsequently routed through this ulnar tunnel from distal (fovea) to proximal (dorsal ulnar neck).

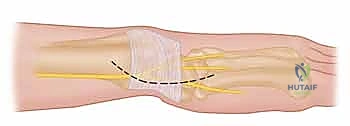
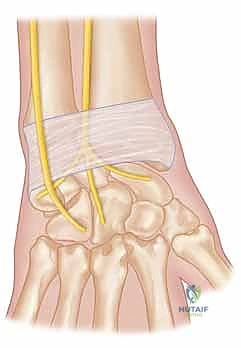
Fixation and Final Assessment:
The graft is then tensioned. The forearm is positioned in neutral rotation, and the DRUJ is manually reduced. The graft is pulled taut through the dorsal ulnar exit hole. Fixation can be achieved using a variety of methods, including a bio-tenodesis screw, a bony anchor, or by suturing the graft back onto itself or the adjacent periosteum.


Following fixation, the stability of the DRUJ is rigorously tested through a full arc of pronosupination. The joint should remain congruous and stable without excessive restriction of motion. Finally, the extensor retinaculum is repaired over the remaining ECU tendon, and the skin is closed in layers.

Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, extra-articular reconstructions of the DRUJ and ulnocarpal joint carry a distinct profile of potential complications. The surgeon must be acutely aware of these risks, counsel the patient appropriately during the preoperative phase, and possess the requisite skills to manage these adverse events should they arise.
The most feared
