Sauvé-Kapandji Procedure: A Masterclass in Distal Radioulnar Joint Reconstruction

Key Takeaway
This masterclass guides fellows through the Sauvé-Kapandji procedure for painful distal radioulnar joint (DRUJ) arthritis and instability. We cover comprehensive anatomy, meticulous preoperative planning, and a granular, real-time intraoperative execution. Learn precise osteotomy, DRUJ arthrodesis, and hardware application, emphasizing neurovascular protection, proper alignment, and critical pearls to optimize outcomes and manage potential complications.
Comprehensive Introduction and Patho-Epidemiology
Welcome, fellows and colleagues, to the operating theater and this comprehensive academic review. Today, we are addressing a profoundly challenging yet immensely rewarding clinical entity: symptomatic distal radioulnar joint (DRUJ) arthritis, incongruity, and chronic instability. Our patient presents with a classic constellation of symptoms—chronic ulnar-sided wrist pain, severely limited forearm rotation, diminished grip strength, and mechanical clunking—consistent with end-stage DRUJ derangement following a remote, malunited distal radius fracture. To address this complex pathology, we will be performing a Sauvé-Kapandji procedure. Originally described in 1936 by French surgeons L. Sauvé and M. Kapandji, this technique offers a robust, biomechanically sound solution by arthrodesing the DRUJ to eliminate pain, while simultaneously creating a controlled pseudoarthrosis in the proximal ulnar metaphysis to restore forearm pronation and supination.

The evolution of DRUJ reconstruction has been driven by the high complication rates associated with earlier, simpler procedures. For decades, the Darrach procedure (resection of the distal ulna) was the workhorse for DRUJ arthritis. However, excision of the ulnar head catastrophically removes the critical ulnar buttress of the carpus, frequently leading to ulnar translation of the carpus, radioulnar impingement, and a debilitating loss of grip strength. The Sauvé-Kapandji procedure elegantly circumvents these pitfalls. By retaining the ulnar head and fusing it to the sigmoid notch of the radius, the ulnocarpal ligamentous complex (the triangular fibrocartilage complex, or TFCC) remains anchored. This preserves the anatomical platform that supports the ulnar carpus, maintains the integrity of the extensor carpi ulnaris (ECU) subsheath, and provides a stable strut for load transmission across the wrist.
Understanding the patho-epidemiology of DRUJ disorders is critical for appropriate patient selection. The most common etiology necessitating a Sauvé-Kapandji procedure is post-traumatic osteoarthritis. Displaced fractures or malunions of the distal radius (such as Colles or Smith fractures with intra-articular extension into the sigmoid notch) inevitably alter the kinematics of the DRUJ. Even minor degrees of radial shortening, dorsal tilt, or translational deformity can exponentially increase the contact stresses at the DRUJ, leading to rapid cartilage wear, secondary rupture or elongation of the radioulnar ligaments, and profound pain. Another major demographic includes patients with advanced rheumatoid arthritis (RA). In RA, synovial hypertrophy relentlessly destroys the DRUJ and the TFCC, progressing to the classic "caput ulnae syndrome"—characterized by dorsal prominence of the distal ulna, volar subluxation of the carpus, profound weakness, and the impending threat of extensor tendon ruptures (Vaughan-Jackson syndrome).

Beyond trauma and inflammatory arthropathies, congenital anomalies such as Madelung deformity present unique reconstructive challenges that are well-served by this operation. In Madelung deformity, premature closure of the volar-ulnar distal radial physis results in an exaggerated volar tilt, severe positive ulnar variance, and dorsal dislocation of the ulnar head. The Sauvé-Kapandji procedure not only addresses the painful incongruity but also allows the surgeon to acutely correct the ulnar variance by resecting an appropriate length of the ulnar diaphysis. Iatrogenic causes, such as a previously failed Darrach procedure or Bowers hemiresection interposition arthroplasty, can also be salvaged with a modified Sauvé-Kapandji, provided enough ulnar head remains to achieve a solid arthrodesis with the radius.
Detailed Surgical Anatomy and Biomechanics
Before we make any incisions, a rigorous review of the critical anatomy and biomechanics of the distal forearm is mandatory. The DRUJ is a pivotal diarthrodial articulation that, in concert with the proximal radioulnar joint (PRUJ), allows the radius to sweep around the stationary ulna, facilitating pronation and supination. This complex system relies on a delicate balance between bony congruence and an intricate web of robust soft tissue stabilizers.
Bony Anatomy and Articular Congruence
The bony architecture of the DRUJ is inherently unstable. The sigmoid notch of the distal radius is a shallow, concave articular surface with a radius of curvature of approximately 15 mm. Conversely, the ulnar head is semicylindrical, possessing a tighter radius of curvature of about 10 mm and an articular convexity that spans roughly 220 degrees. Crucially, because these radii of curvature do not perfectly match, the joint lacks intrinsic osseous stability. In the extremes of pronation and supination, less than 10% of the ulnar head may actually be in contact with the sigmoid notch. This profound inherent incongruity dictates that the stability of the DRUJ is almost entirely dependent on its soft tissue envelope. Furthermore, the ulnar styloid acts as a vital bony strut, serving as the foundational anchor for the ulnocarpal soft tissue complex.
Ligamentous Stabilizers
The triangular fibrocartilage complex (TFCC) is the primary, indispensable stabilizer of the DRUJ. The core of this complex is the triangular fibrocartilage (TFC) articular disc, which originates at the junction of the lunate fossa and sigmoid notch and inserts firmly at the fovea at the base of the ulnar styloid. The central portion of the TFC is avascular and cartilaginous, explicitly designed to absorb compressive weight-bearing forces transmitted from the ulnar carpus. However, the peripheral margins—specifically the dorsal and palmar radioulnar ligaments—are composed of thick, well-vascularized lamellar collagen designed to resist immense tensile loading. During supination, the palmar radioulnar ligament tightens, while in pronation, the dorsal radioulnar ligament becomes taut. These ligaments receive their blood supply from the palmar and dorsal branches of the anterior interosseous artery and the ulnar artery. Extending distally from this complex are the ulnocarpal ligaments (ulnolunate and ulnotriquetral), which provide crucial volar stability to the ulnar carpus.
Musculotendinous Stabilizers
Dynamic stabilization of the DRUJ is provided by the surrounding musculotendinous units. The Extensor Carpi Ulnaris (ECU) tendon is paramount; it runs through a dedicated, robust fibro-osseous tunnel (the sixth dorsal compartment) deep to the extensor retinaculum. The ECU subsheath acts as a dynamic tension band across the dorsal aspect of the joint. Preserving the relationship between the ECU and the ulnar head is a major biomechanical advantage of the Sauvé-Kapandji procedure over excisional arthroplasties. Volarly, the Pronator Quadratus (PQ) muscle plays a dual role. During active pronation, the deep head of the PQ actively coapts the ulnar head into the sigmoid notch. During supination, it passively stabilizes the joint through viscoelastic tension. We will meticulously preserve the PQ during our extraperiosteal dissection to utilize it as an interpositional flap later in the procedure.
Neurovascular Topography
Navigating the neurovascular topography is the most treacherous aspect of the surgical approach. The Dorsal Cutaneous Branch of the Ulnar Nerve (DCBUN) is the structure at highest risk. It typically branches from the main ulnar nerve 5 to 8 cm proximal to the pisiform, emerging from beneath the flexor carpi ulnaris (FCU) tendon to course dorsally and superficially over the distal ulna. It crosses directly through our surgical field. It is highly susceptible to iatrogenic transection or traction injury during the initial incision and superficial dissection; injury here leads to agonizing, recalcitrant dysesthesias and neuromas. Deeper in the volar compartment, the ulnar artery and main ulnar nerve lie protected beneath the FCU, but extreme care must be taken when placing retractors or passing instruments volarly around the ulnar neck.
Exhaustive Indications and Contraindications
The decision to proceed with a Sauvé-Kapandji procedure must be made after a careful analysis of the patient's pathology, functional demands, and the integrity of the surrounding anatomical structures. It is primarily considered a salvage procedure, utilized when joint-preserving operations (such as ligamentous reconstructions or corrective osteotomies) are no longer viable due to advanced articular destruction.
The primary indication is painful osteoarthritis or rheumatoid arthritis of the DRUJ accompanied by a structurally intact proximal radioulnar joint (PRUJ). In the rheumatoid patient, the Sauvé-Kapandji is often the procedure of choice. Unlike the Darrach procedure, which can exacerbate the natural tendency of the rheumatoid carpus to translocate ulnarly and volarly, the Sauvé-Kapandji maintains the ulnar head as a physical buttress and preserves the vital ulnocarpal ligaments. It is also highly indicated for post-traumatic DRUJ incongruity following distal radius fractures, especially when there is concurrent positive ulnar variance that requires simultaneous shortening. Furthermore, it is an excellent option for managing the painful, stiff DRUJ in patients with Madelung deformity, where the complex three-dimensional deformity makes anatomical reconstruction nearly impossible.
However, the procedure is not without strict contraindications. The most absolute contraindication is a compromised proximal radioulnar joint (PRUJ). Because the Sauvé-Kapandji relies on the creation of a proximal pseudoarthrosis for forearm rotation, the radius must be able to rotate freely around the proximal ulna at the PRUJ. If the PRUJ is arthritic, fused, or unstable (e.g., following a radial head excision without a stable prosthesis), the Sauvé-Kapandji will fail to restore rotation and will likely result in severe proximal stump instability and pain. This scenario—often seen in the Essex-Lopresti lesion—requires alternative management strategies, such as creation of a one-bone forearm.
Relative contraindications include patients with extremely high physical demands or those engaged in heavy manual labor. While the Sauvé-Kapandji provides excellent pain relief, the proximal ulnar stump is inherently unstable and can impinge against the radius during heavy lifting or forceful gripping, leading to secondary pain. In young, high-demand laborers with isolated DRUJ arthritis, an ulnar head arthroplasty or a partial ulnar head resection (Bowers procedure) might be considered first, reserving the Sauvé-Kapandji as a secondary salvage option. Additionally, active local or systemic infection is an absolute contraindication to any elective arthrodesis.
| Category | Specific Clinical Scenarios | Rationale / Considerations |
|---|---|---|
| Primary Indications | End-stage DRUJ Osteoarthritis | Salvage for destroyed articular cartilage; relieves pain while preserving ulnocarpal support. |
| Rheumatoid Arthritis (Caput Ulnae) | Prevents ulnar/volar carpal translocation; maintains ECU subsheath and TFCC integrity. | |
| Post-traumatic Incongruity | Ideal for malunited distal radius fractures, especially with associated positive ulnar variance. | |
| Madelung Deformity | Addresses complex multi-planar deformity and pain; allows for acute ulnar shortening. | |
| Absolute Contraindications | PRUJ Arthritis or Instability | The procedure relies entirely on a functioning PRUJ for forearm rotation. |
| Active Infection | Arthrodesis and hardware placement are strictly contraindicated in the presence of infection. | |
| Essex-Lopresti Lesion (Unreconstructed) | Longitudinal radioulnar dissociation will lead to catastrophic proximal stump convergence. | |
| Relative Contraindications | Heavy Manual Laborers | High risk of symptomatic radioulnar impingement at the proximal ulnar stump during heavy lifting. |
| Non-compliant Patients | Post-operative immobilization and phased rehabilitation are critical to achieving bony union. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of a successful Sauvé-Kapandji reconstruction. The surgical strategy must be meticulously mapped out before the patient ever enters the operating room, relying on a combination of high-quality imaging and precise geometric templating.
Imaging and Diagnostic Studies
Standard, high-quality radiographs are the first step. We require strict neutral rotation posteroanterior (PA) and lateral views of the wrist, as well as specific views to assess ulnar variance. We always compare these to the contralateral, unaffected wrist to establish the patient's baseline anatomy. On the PA view, we scrutinize the relative position of the distal ulna to the radius (ulnar variance), looking for signs of ulnocarpal abutment, cystic changes in the lunate or ulnar head, and the overall alignment of the carpus. If dynamic ulnocarpal abutment is suspected but not obvious on static films, a PA radiograph taken with the forearm in pronation and the fist forcefully clenched can dynamically increase positive ulnar variance and reveal the impaction.

Advanced imaging is frequently necessary to fully characterize the pathology. Computed Tomography (CT) scans are invaluable for assessing the three-dimensional architecture of the sigmoid notch, the degree of dorsal or volar subluxation of the ulnar head, and the exact extent of articular cartilage loss. We routinely obtain simultaneous CT views of both upper extremities in neutral rotation, full supination, and full pronation to truly understand the dynamic instability of the joint. Magnetic Resonance Imaging (MRI), particularly MRA (MR Arthrography) with intra-articular gadolinium, is excellent for evaluating the soft tissue envelope. It allows us to assess the integrity of the TFCC, the ECU subsheath, and the scapholunate and lunotriquetral interosseous ligaments, which are frequently injured concurrently in post-traumatic scenarios.

Surgical Planning and Templating
The crux of the preoperative plan involves determining the exact level of the ulnar osteotomy and the precise length of the bony resection. We carefully review the templated radiographs to determine the appropriate level for the distal ulnar cut. The goal is to transect the ulna just proximal to the metaphyseal flare of the ulnar head. This leaves a sufficient block of distal ulna to safely accommodate two lag screws (typically 3.5 mm or 4.0 mm cannulated screws) for the arthrodesis, ensuring a rigid construct.

The length of the resected segment is critical to the success of the pseudoarthrosis. If there is pre-existing positive ulnar variance, we must plan to resect a larger segment of the ulna to allow the ulnar head to be recessed proximally, achieving neutral or slightly negative ulnar variance at the time of arthrodesis. The final gap created (the pseudoarthrosis site) must be substantial enough to prevent bony cross-union (synostosis) but not so large that it exacerbates proximal stump instability. Typically, a gap of 10 to 15 mm is targeted after the ulnar variance has been corrected. We will use cannulated self-tapping screws for the arthrodesis; they provide secure, rigid compression, allow for earlier postoperative rehabilitation, and completely avoid the high complication rates (pin tract infections, nerve irritation, loss of fixation) historically associated with Kirschner wire fixation.

Patient Positioning and Setup
Patient positioning must facilitate unhindered access to the entire forearm and allow for dynamic intraoperative fluoroscopy.
1. Supine Position: The patient is positioned supine on the operating table with the arm extended.
2. Hand Table: The operative upper extremity is placed on a radiolucent, dedicated hand table. The table must be completely stable and large enough to support the arm from the elbow to the fingertips.
3. Pneumatic Tourniquet: A well-padded pneumatic tourniquet is applied high on the brachium. We will exsanguinate the arm with an Esmarch bandage and inflate the tourniquet (typically to 250 mmHg) immediately prior to incision. A bloodless field is absolutely mandatory for the meticulous dissection required to identify and protect the delicate cutaneous nerves.
4. Fluoroscopy: The intraoperative C-arm fluoroscope is draped sterilely and positioned perpendicular to the hand table, ready to be brought into the field seamlessly. We will rely on it heavily to confirm our osteotomy levels, verify the correction of ulnar variance, and ensure perfect trajectory of our cannulated hardware.
5. Forearm Position for Arthrodesis: During the critical arthrodesis phase, we will position the patient's elbow flexed to 90 degrees, resting firmly on the operating table, with the forearm directed vertically (perpendicular to the table) in absolute neutral rotation. This specific positioning is paramount for accurately judging and setting the ulnar variance prior to definitive fixation.
Step-by-Step Surgical Approach and Fixation Technique
With the preoperative plan finalized and the patient optimally positioned, we are ready to proceed with the operative execution. This procedure demands meticulous soft tissue handling, precise bony cuts, and rigid internal fixation.
Incision and Superficial Dissection
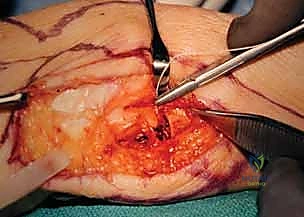
"Scalpel, please, and a skin hook." We begin by making a straight, longitudinal incision, approximately 6 to 8 centimeters in length, centered directly over the ulnar border of the distal forearm. This direct ulnar approach provides excellent, extensile exposure of the ulnar neck and head while minimizing unnecessary soft tissue stripping. In specific cases, such as patients with severe rheumatoid arthritis requiring a concurrent dorsal tenosynovectomy or extensor tendon transfer, we might utilize a more dorsal longitudinal incision, raising thick fasciocutaneous flaps to access both the DRUJ and the dorsal compartments. However, for an isolated Sauvé-Kapandji, the straight ulnar incision is optimal.

Immediately upon incising the skin and superficial subcutaneous fat, we enter the most critical danger zone of the procedure. Surgical Warning: Fellows, the Dorsal Cutaneous Branch of the Ulnar Nerve (DCBUN) must be actively identified and protected before any deep dissection occurs. Using fine tenotomy scissors or a blunt mosquito hemostat, carefully spread the subcutaneous tissues. The DCBUN typically emerges from beneath the volar aspect of the FCU tendon in the proximal aspect of our incision and courses obliquely across the ulnar border toward the dorsal aspect of the hand. Once identified, we gently mobilize it with a vessel loop and retract it safely out of the surgical field, usually volarly. We must be vigilant not to place excessive traction on this nerve throughout the case.
Deep Dissection and Extraperiosteal Exposure
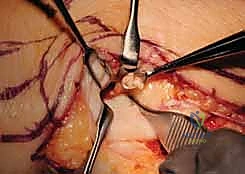
With the nerve protected, we proceed to the deep fascial layer. We incise the deep fascia longitudinally, precisely developing the interval between the Extensor Carpi Ulnaris (ECU) tendon dorsally and the Flexor Carpi Ulnaris (FCU) tendon volarly. Using blunt retractors, we retract the ECU dorsally and the FCU volarly, revealing the distal ulnar diaphysis and the metaphyseal flare.

Our approach to the bone is strictly extraperiosteal. We incise the periosteum longitudinally along the ulnar shaft and carefully elevate it using a sharp periosteal elevator. It is imperative to preserve the periosteal sleeve as much as possible, as we will later close it over the pseudoarthrosis gap to act as a barrier against hematoma and bone regeneration. As we dissect volarly around the ulnar neck, we encounter the Pronator Quadratus (PQ) muscle. We meticulously elevate the ulnar insertion of the PQ, preserving its muscle belly, as this will serve as our primary interpositional soft tissue flap.
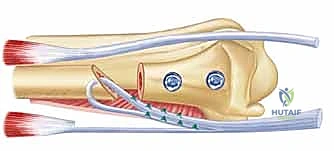
The Ulnar Osteotomies
"Alright, the ulna is well exposed. Let's bring in the C-arm to confirm our osteotomy sites." We must execute two precise cuts to create the pseudoarthrosis gap.

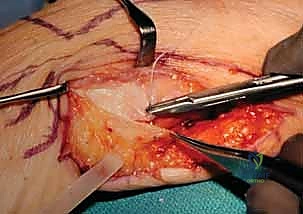
- The Distal Cut: We plan the first cut just proximal to the metaphyseal flare of the ulnar head. We must ensure we are entirely proximal to the articular surface of the DRUJ, yet distal enough to leave a robust block of bone that can accommodate two 3.5 mm or 4.0 mm screws. We verify this level with fluoroscopy. Using a small oscillating microsaw with a fresh blade, we make a clean, perpendicular cut across the ulnar shaft. Copious, continuous saline irrigation is applied directly to the blade to prevent thermal necrosis of the bone, which could compromise our arthrodesis.
- The Proximal Cut: Based on our preoperative measurements, we measure proximally from our first cut to mark the second osteotomy. If the patient has 3 mm of positive ulnar variance and we desire a final pseudoarthrosis gap of 12 mm, we must resect a total of 15 mm of bone. We mark the bone, verify with fluoroscopy, and make the second perpendicular cut. The cylindrical segment of the ulnar diaphysis is then removed and discarded (or saved as local autograft if needed for the arthrodesis site).
Joint Preparation and Arthrodesis
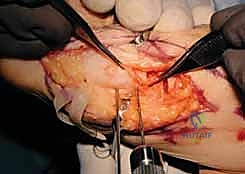
With the ulnar diaphysis resected, the ulnar head is now freely mobile, tethered only by the TFCC and ulnocarpal ligaments distally. We use a sturdy towel clip or a small bone clamp to grasp the ulnar head. By applying gentle traction and rotating the head, we gain excellent access to the articular surfaces of the DRUJ.
Using a high-speed burr or a sharp rongeur, we meticulously decorticate the articular cartilage down to bleeding subchondral bone on both the ulnar head and the corresponding sigmoid notch of the radius. It is absolutely critical during this step to protect the distal and volar attachments of the TFCC to the fovea of the ulnar head. Stripping these attachments will
Clinical & Radiographic Imaging Archive