Olecranon Fractures: Tension Band Wiring Principle, Surgical Anatomy & Biomechanics
Key Takeaway
Tension band wiring for olecranon fractures converts distracting tensile forces, primarily from the triceps muscle, into stable compressive forces across the fracture site. This dynamic compression, achieved with K-wires and a figure-of-eight wire, promotes healing and allows for early, protected mobilization. It's a cornerstone technique for transverse and short oblique olecranon fractures, minimizing stiffness.
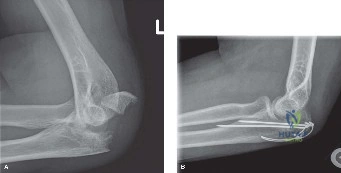
A 45-year-old patient presents following a fall onto the elbow. Radiographs confirm a displaced, simple transverse fracture of the olecranon. You are discussing the surgical plan for tension band wiring (TBW). The patient asks, "Why are we using a wire loop if the bone is broken? Won't the muscle just pull it apart?" How do you explain the biomechanical principle of the tension band to the patient, and what is your requirement for the construct to work?
Candidate: "The triceps pulls on the olecranon, creating a distraction force that opens the fracture. The tension band wire acts like a rope on the back of the bone; when you tighten it, it pulls the fracture together, turning that pulling force into a compression force. For it to work, I need to make sure the front of the joint (the anterior cortex) is intact, because that acts as a hinge, and I need two solid K-wires to hold the bone in place."
Failing to emphasize the importance of the intact anterior cortex. If the candidate describes the "tension band" but fails to mention the biomechanical requirement of a "compression side" (the anterior cortex acting as a fulcrum), they demonstrate a lack of fundamental understanding. Also, failing to mention the dynamic nature—that the construct actually gets tighter as the elbow flexes—is a missed opportunity for higher marks.
The candidate should state: "The tension band principle converts the distractive tensile forces of the triceps into compressive forces across the articular surface. The posterior cortex acts as the tension side, while the anterior cortex (the trochlear notch) acts as the compression side/fulcrum. For the construct to succeed, we require: 1) An intact anterior cortex to act as the pivot point; 2) Anatomical reduction of the articular surface; 3) Parallel K-wires to provide axial and rotational stability; and 4) Proper tensioning of the figure-of-eight wire. This construct is 'dynamic' because it provides more compression as the elbow flexes."
We are in the operating theatre. You have performed your exposure. Describe your specific surgical steps to achieve definitive fixation for this fracture using the tension band wiring technique.
Candidate: "After identifying and protecting the ulnar nerve, I would reduce the articular surface anatomically using pointed reduction forceps. Once reduced, I would pass two 1.6mm or 2.0mm K-wires longitudinally from the olecranon tip into the ulnar shaft, engaging the anterior cortex. I'd then make a transverse drill hole distal to the fracture, pass the 18-gauge wire through it in a figure-of-eight, loop it over the K-wires, tighten it, and finally bend and bury the K-wire tips into the bone."
Forgetting the ulnar nerve. In an FRCS viva, failing to mention the neurovascular structures during the surgical steps is a major safety omission. Also, forgetting to "bury" the K-wire ends is a common oversight that leads to the most common post-operative complaint: hardware prominence.
The candidate must be systematic: 1. Exposure: Midline incision, protecting the ulnar nerve (identify and protect early). 2. Reduction: Direct visualization of the joint surface, maintaining reduction with pointed forceps. 3. K-wires: Insert two parallel K-wires to engage the anterior cortex (not the articular surface) for axial stability. 4. Tensioning: Create a transverse drill hole 2-3cm distal to the fracture. Pass 18G wire in a figure-of-eight. 5. Finalizing: Bend K-wires 180 degrees, cut, and impact into the proximal olecranon to avoid hardware irritation. Confirm stability and reduction with fluoroscopy.
The patient returns at 6 months complaining of significant pain over the tip of their elbow, making it difficult to lean on their elbow or wear certain clothes. The fracture is fully healed on X-ray. What is the most likely cause, and how do you manage it?
Candidate: "This is hardware prominence, which is the most common complication of tension band wiring, occurring in up to 80% of patients. Since the fracture is healed, I would offer elective hardware removal. I would warn the patient that it's a day-case procedure but carries the usual risks of infection, scarring, and injury to the cutaneous nerves."
Suggesting immediate hardware removal without confirming union. Always emphasize that hardware removal should only be done after radiographic confirmation of bone healing. Failing to mention the high incidence rate (managing patient expectations) makes the candidate appear less experienced.
Acknowledge the high prevalence of hardware prominence (30-80%). Manage the patient by: 1. Confirming fracture union on imaging. 2. Discussing the elective nature of the procedure. 3. Listing the benefits (pain relief) vs. the risks (surgical site infection, scar, neuroma). Mention that this is a routine elective procedure that typically results in high patient satisfaction.
