
Introduction and Epidemiology
Fractures of the radius and ulna shafts represent a complex orthopedic challenge due to the intricate biomechanical relationship between these two bones. The forearm functions not merely as a structural appendage but as a highly specialized joint facilitating pronation and supination while transmitting loads from the wrist to the elbow. Disruption of this diaphyseal segment significantly impairs upper extremity kinematics.
Epidemiologically, forearm diaphyseal fractures exhibit a bimodal distribution. They are predominantly observed in young adult males, secondary to high-energy trauma such as motor vehicle collisions, motorcycle accidents, contact athletic participation, and falls from a height. A secondary peak occurs in the elderly population, particularly females, associated with low-energy falls and osteoporotic bone.
Notably, the ratio of open fractures to closed fractures in the forearm is exceptionally high, surpassed anatomically only by the tibial diaphysis. This is primarily due to the subcutaneous nature of the ulnar border and the high-energy mechanisms frequently responsible for these injuries. Pathologic fractures in the forearm diaphysis remain relatively uncommon but should be considered in patients with a known history of malignancy or atypical radiographic presentations.
Surgical Anatomy and Biomechanics
A profound understanding of forearm anatomy and biomechanics is the cornerstone of successful surgical management. The forearm must be conceptualized as a closed anatomic ring, functionally analogous to the pelvic ring or the mandible. The components of this ring include the radius, the ulna, the proximal radioulnar joint, the distal radioulnar joint, and the interosseous membrane.
The Forearm Ring Concept
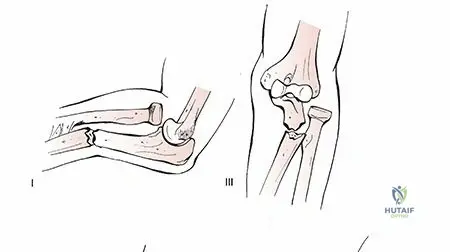
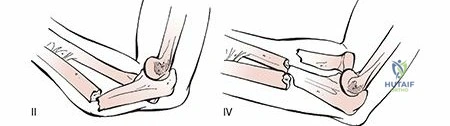
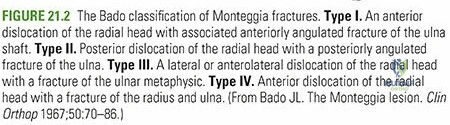
Because the forearm acts as a rigid ring, a fracture resulting in significant shortening or angulation of either the radius or the ulna inevitably leads to either a concurrent fracture of the paired bone or a dislocation at one of the radioulnar joints. Classic examples include the Monteggia fracture-dislocation (proximal ulnar shaft fracture with radial head dislocation) and the Galeazzi fracture-dislocation (distal radial shaft fracture with distal radioulnar joint disruption). Isolated fractures without joint disruption only occur via direct, low-energy trauma, classically described as the "nightstick" fracture of the ulna.
Osteology and Kinematics
The ulna is relatively straight and serves as the stable, fixed axis of the forearm. In contrast, the radius is laterally bowed and rotates around the ulnar axis during pronation and supination. The preservation and anatomic restoration of the lateral curvature of the radius, known as the "radial bow," is paramount. Failure to restore the magnitude and location of the maximum radial bow correlates directly with a permanent loss of forearm rotation and diminished grip strength.
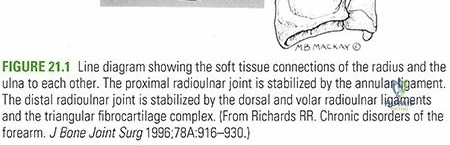
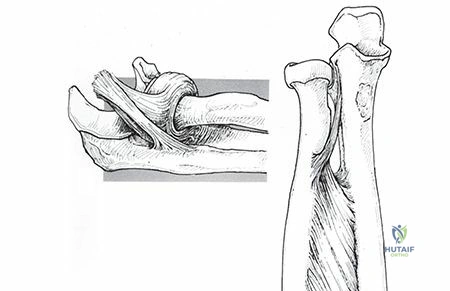
The Interosseous Membrane
The interosseous membrane occupies the radioulnar space, providing longitudinal stability and transmitting forces from the radius to the ulna. The central band is the most critical structural component, measuring approximately 3.5 centimeters in width and running obliquely from its proximal origin on the radius to its distal insertion on the ulna. Biomechanical studies indicate that sectioning the central band alone reduces longitudinal stability by up to 71 percent.
Muscular Deforming Forces
Fracture location dictates the specific deforming forces acting upon the osseous fragments. Recognizing these forces is essential for executing an anatomic reduction.
Proximal third radial shaft fractures occur distal to the supinator insertion but proximal to the pronator teres insertion. In this scenario, the proximal fragment is forcefully supinated and flexed by the unopposed action of the supinator and biceps brachii muscles. The distal fragment is concomitantly pronated by the pronator teres and pronator quadratus.
Middle third radial shaft fractures occur distal to the insertions of both the supinator and the pronator teres. Consequently, the proximal fragment remains in neutral rotational alignment, as the supinating force of the biceps and supinator is counterbalanced by the pronating force of the pronator teres. The distal fragment remains pronated due to the isolated pull of the pronator quadratus.

Indications and Contraindications
The management of diaphyseal forearm fractures in adults is almost exclusively surgical. Unlike pediatric patients, adults possess negligible remodeling potential in the forearm diaphysis. Non-operative management of both-bone forearm fractures in adults yields unacceptably high rates of malunion, nonunion, and catastrophic loss of pronosupination.
Conservative management is strictly reserved for isolated, non-displaced fractures or specific low-energy injuries meeting rigid radiographic criteria.
| Management Strategy | Indications | Contraindications |
|---|---|---|
| Non-Operative Management | Isolated ulnar shaft fractures (Nightstick) with < 50% displacement and < 10 degrees angulation | Both-bone forearm fractures in adults |
| Isolated radial shaft fractures with absolute non-displacement | Monteggia or Galeazzi fracture-dislocations | |
| Patients with absolute medical contraindications to anesthesia | Open fractures | |
| Pediatric patients with acceptable angulation and remodeling potential | Volar compartment syndrome | |
| Operative Management (ORIF) | Displaced both-bone forearm fractures in adults | Active local soft tissue infection (relative contraindication for internal fixation; external fixation preferred) |
| Isolated radial or ulnar shaft fractures exceeding acceptable displacement parameters | Severe osteomyelitis | |
| All Monteggia and Galeazzi fracture-dislocations | ||
| Open forearm fractures | ||
| Fractures associated with acute compartment syndrome requiring fasciotomy | ||
| Pathologic fractures |
Pre Operative Planning and Patient Positioning
Thorough preoperative evaluation and meticulous planning are mandatory to minimize intraoperative complications and optimize functional outcomes.
Clinical Evaluation
Patients typically present with gross clinical deformity, significant edema, ecchymosis, and functional impotence of the affected upper extremity. A rigorous neurovascular examination must be documented prior to any intervention. This includes assessment of the radial and ulnar arterial pulses, capillary refill, and the motor and sensory distributions of the median, radial, and ulnar nerves.
Given the subcutaneous nature of the ulna, the entire forearm must be circumferentially inspected for traumatic arthrotomies or open wounds. Even pinpoint superficial wounds in the presence of an underlying fracture must be treated as open fractures until proven otherwise.
Surgeons must maintain a high index of suspicion for acute compartment syndrome. Excruciating pain out of proportion to the injury, tense forearm compartments on palpation, and severe pain with passive stretch of the digits are hallmark signs. If compartment syndrome is suspected, compartment pressure monitoring should be performed immediately. A delta pressure (diastolic blood pressure minus compartment pressure) of less than 30 mmHg is a definitive indication for emergent volar and dorsal fasciotomies.
Radiographic Evaluation
Standard orthogonal anteroposterior and lateral radiographs of the entire forearm are required. Crucially, these images must encompass both the ipsilateral wrist and elbow joints to definitively rule out complex fracture-dislocations.
The radiocapitellar line must be evaluated on all views; a line drawn through the center of the radial shaft and radial head must perfectly bisect the capitellum regardless of the radiographic projection. Disruption of this line indicates a radial head dislocation (Monteggia variant). Similarly, the distal radioulnar joint must be scrutinized for widening or dorsal/volar subluxation of the distal ulna (Galeazzi variant).
Templating and Implant Selection
Preoperative templating ensures appropriate implant availability. The gold standard for diaphyseal forearm fractures is rigid internal fixation using 3.5 mm dynamic compression plates (LC-DCP) or locking compression plates (LCP). For transverse or short oblique fractures, absolute stability is required, necessitating compression plating techniques. For highly comminuted or segmental fractures, bridge plating techniques are employed to preserve the fracture hematoma and soft tissue envelope, relying on relative stability and secondary bone healing.
Patient Positioning
The patient is positioned supine on a standard radiolucent operating table. The operative extremity is extended onto a radiolucent hand table. A sterile non-sanguineous tourniquet is applied to the proximal brachium. The entire upper extremity is prepped and draped freely to allow unrestricted manipulation, pronation, supination, and intraoperative fluoroscopic evaluation.
Detailed Surgical Approach and Technique
Surgical management of both-bone forearm fractures typically involves two separate incisions to minimize the risk of radioulnar synostosis. The sequence of fixation is dictated by fracture morphology; generally, the less comminuted bone is reduced and provisionally fixed first to restore length and axial alignment, facilitating the reduction of the more complex paired bone.
Surgical Approach to the Radius
The radius can be accessed via two primary surgical corridors depending on the location of the fracture and surgeon preference.
The Volar Henry Approach
The volar Henry approach is the workhorse exposure for the middle and distal thirds of the radial diaphysis. It exploits the internervous plane between the brachioradialis (innervated by the radial nerve) and the flexor carpi radialis (innervated by the median nerve).
The incision is made along a line connecting the biceps tendon proximally to the radial styloid distally. Superficial dissection identifies the cephalic vein, which is retracted laterally. The deep fascia is incised, and the plane between the brachioradialis and flexor carpi radialis is developed.
In the proximal aspect of the wound, the superficial radial nerve and the radial artery are identified. The radial artery must be protected and retracted medially. To mobilize the brachioradialis laterally, the radial recurrent artery and its associated venous venae comitantes (the "leash of Henry") must be meticulously isolated, ligated, and divided.
Deep dissection exposes the supinator muscle proximally, the pronator teres in the middle third, and the pronator quadratus distally. To expose the proximal radius, the supinator must be elevated. To protect the posterior interosseous nerve, which courses through the substance of the supinator, the forearm is fully supinated, and the supinator is sharply detached from its ulnar insertion and reflected laterally.
The Dorsal Thompson Approach
The dorsal Thompson approach is primarily utilized for fractures of the proximal third of the radius. It utilizes the internervous plane between the extensor carpi radialis brevis (radial nerve) and the extensor digitorum communis (posterior interosseous nerve).
The incision connects the lateral epicondyle to the Lister tubercle. The fascial interval between the ECRB and EDC is incised. The posterior interosseous nerve is at significant risk during this approach. It exits the supinator muscle approximately 1 centimeter proximal to the distal edge of the muscle belly. The supinator is incised along its ulnar border and reflected radially to expose the proximal radial shaft, protecting the PIN within the reflected muscle flap.
Surgical Approach to the Ulna
The ulna is approached directly along its subcutaneous border. The internervous plane lies between the extensor carpi ulnaris (posterior interosseous nerve) and the flexor carpi ulnaris (ulnar nerve).
A linear longitudinal incision is made directly over the palpable ulnar crest. The deep fascia is incised, and the extensor and flexor muscle masses are elevated subperiosteally to expose the fracture site. Care must be taken not to strip the periosteum excessively, as this devitalizes the cortical bone and increases the risk of delayed union or nonunion.
Fracture Reduction and Fixation Techniques
Once the fracture sites are exposed, hematoma is evacuated, and the fracture ends are meticulously debrided. Anatomic reduction is achieved using specialized reduction forceps. For transverse fractures, contouring the plate to the anatomy of the bone and utilizing eccentric drilling techniques achieves dynamic axial compression.
Biomechanical principles dictate the use of 3.5 mm heavy-duty plates. A minimum of six cortices of purchase (three bicortical screws) is required both proximal and distal to the fracture zone. For the radius, the plate is typically applied to the volar surface using the Henry approach, as this provides a flat surface for plate seating and excellent soft tissue coverage. For the ulna, the plate is applied to the dorsal or tension band surface when possible, though medial or lateral application is acceptable depending on skin conditions and fracture morphology.
Restoration of the radial bow is critically assessed prior to final tightening. Intraoperative fluoroscopy is utilized to confirm anatomic reduction, plate positioning, screw length, and restoration of the radiocapitellar line and distal radioulnar joint congruity.
Complications and Management
Despite meticulous surgical technique, diaphyseal forearm fractures are associated with a distinct profile of postoperative complications. Early recognition and aggressive management are required to salvage functional outcomes.
| Complication | Incidence and Pathophysiology | Management and Salvage Strategies |
|---|---|---|
| Radioulnar Synostosis | Occurs in 2-6% of cases. Risk factors include severe soft tissue trauma, head injury, combined approaches through a single incision, and fractures occurring at the same level. | Prevention is paramount (separate surgical approaches). Once established, excision of the heterotopic ossification is delayed until the bone scan is cold (typically 6-12 months post-injury). Post-excision radiation or Indomethacin prophylaxis is indicated. |
| Nonunion | Occurs in 2-10% of cases. Associated with inadequate rigid fixation, severe comminution, devascularization from aggressive periosteal stripping, and infection. | Requires revision ORIF. Hypertrophic nonunions require improved mechanical stability (larger plate, compression). Atrophic nonunions require mechanical stability combined with biological augmentation (autologous iliac crest bone grafting). |
| Posterior Interosseous Nerve Palsy | Most commonly iatrogenic, associated with the dorsal Thompson approach or aggressive proximal retraction during the volar Henry approach. | Most represent neuropraxia secondary to traction and resolve spontaneously within 3-6 months. Expectant management with wrist and finger splinting to prevent contracture. If no recovery is noted by 6 months, EMG/NCS and possible tendon transfers are indicated. |
| Compartment Syndrome | High-energy crush injuries or severe soft tissue swelling. Volar compartments are most frequently involved. | Emergent volar and dorsal forearm fasciotomies. Delayed primary closure or split-thickness skin grafting once swelling subsides. |
| Infection | More common in open fractures. Superficial vs. deep osteomyelitis. | Aggressive surgical debridement, hardware retention if fixation remains absolutely stable and infection is acute. Suppressive antibiotics. If fixation is loose, hardware removal, external fixation, and staged reconstruction are required. |
| Malunion | Failure to restore the radial bow or axial alignment, leading to restricted pronosupination and distal radioulnar joint arthrosis. | Corrective osteotomy. Preoperative 3D CT modeling and custom cutting guides are increasingly utilized to accurately restore the complex three-dimensional anatomy of the radial diaphysis. |
Post Operative Rehabilitation Protocols
The primary objective of rigid internal fixation is to permit immediate, safe mobilization of the upper extremity. Prolonged immobilization is detrimental and leads to profound stiffness of the elbow, wrist, and radioulnar joints.
In the immediate postoperative phase (Days 0-14), the patient is placed in a bulky soft compressive dressing or a removable volar splint. Strict elevation is maintained to mitigate edema. Active and active-assisted range of motion exercises for the digits, wrist, and elbow are initiated within 24 to 48 hours postoperatively, guided by patient tolerance. Gentle pronation and supination exercises are encouraged.
At the two-week mark, sutures are removed. The splint is transitioned to a removable orthosis used primarily for protection in public or during sleep. Formal physical therapy is often initiated to maximize active range of motion.
Weight-bearing is strictly limited. Patients are restricted to lifting no more than one to two pounds for the first six weeks. Radiographic progression of healing is evaluated at 6, 12, and 24 weeks. Progressive resistance exercises and weight-bearing are advanced only after radiographic evidence of bridging callus or obliteration of the fracture lines is confirmed, typically between 8 to 12 weeks postoperatively. Full unrestricted athletic and occupational activities are generally delayed until 4 to 6 months post-injury, contingent upon absolute radiographic union.
Summary of Key Literature and Guidelines
The evolution of operative management for forearm diaphyseal fractures is deeply rooted in several landmark orthopedic studies that continue to dictate current treatment guidelines.
The foundational principles of compression plating were validated by Anderson et al. in their classic 1975 Journal of Bone and Joint Surgery publication. They demonstrated that utilizing 3.5 mm dynamic compression plates yielded union rates exceeding 96 percent and established ORIF as the unequivocal gold standard for adult both-bone forearm fractures, effectively rendering non-operative management obsolete for displaced injuries.
The critical importance of the radial bow was definitively quantified by Schemitsch and Richards in 1992. Their biomechanical and clinical analysis proved that the restoration of the maximal radial bow—both in its magnitude and its exact anatomic location along the diaphysis—is the single most important predictor of functional recovery of pronation and supination. Failure to restore this geometry leads to impingement of the radius against the ulna during rotation.
Current guidelines from the Orthopaedic Trauma Association (OTA) and AO Foundation heavily emphasize the necessity of precise soft tissue handling. The preservation of the periosteal blood supply, particularly in comminuted fracture variants, has led to the increased utilization of bridge plating constructs. By bypassing the zone of comminution and avoiding aggressive stripping of the butterfly fragments, surgeons optimize the biological environment for secondary bone healing, significantly reducing the incidence of atrophic nonunion. Furthermore, current literature dictates that prophylactic fasciotomy should have a low threshold in the setting of high-energy crush injuries to the forearm, given the catastrophic functional sequelae of missed volar compartment syndrome.
Clinical & Radiographic Imaging
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding radius-and-ulna-shaft-fractures