Solving Arthroscopic Valgus Instability: Regain Elbow Stability
Key Takeaway
Learn more about Solving Arthroscopic Valgus Instability: Regain Elbow Stability and how to manage it. Arthroscopic valgus instability refers to elbow instability caused by ulnar collateral ligament (UCL) attenuation from repetitive valgus stress, commonly in overhead athletes. This leads to abnormal valgus rotation, resulting in valgus extension overload, bony impingement, and pain. It is a condition managed through arthroscopic intervention to stabilize the joint.
Introduction and Epidemiology
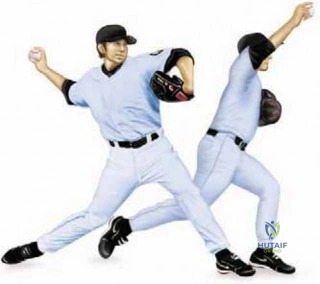
Valgus extension overload of the elbow represents a complex constellation of pathologic changes primarily observed in the overhead throwing athlete. The repetitive, high-velocity kinematics inherent to overhead throwing, particularly pitching, generate extraordinary biomechanical forces across the ulnohumeral and radiocapitellar articulations. The resulting clinical syndrome is characterized by a specific triad of biomechanical derangements: medial compartment distraction, lateral compartment compression, and posterior compartment impingement.

Epidemiologically, valgus extension overload is most frequently diagnosed in baseball pitchers, though it is also prevalent in javelin throwers, tennis players, and volleyball attackers. The incidence of this pathology has risen concurrently with the increasing demands placed on overhead athletes at both the collegiate and professional levels. The repetitive pitching motion imparts a massive valgus torque on the elbow, often approaching 64 Newton-meters (Nm) during the late cocking and early acceleration phases of the throwing cycle. Because the ulnar collateral ligament (UCL) is biomechanically capable of withstanding only approximately 32 Nm of force before failure, the dynamic stabilizers of the flexor-pronator mass must absorb the remaining kinetic energy.

When the dynamic stabilizers fatigue, the repetitive microtrauma is transferred directly to the static restraints, leading to incomplete recovery, subsequent attenuation of the UCL, and the initiation of the valgus extension overload cascade. Failure to recognize and appropriately manage this condition can result in career-ending structural damage to the elbow joint.
Surgical Anatomy and Biomechanics
Osseous Constraints
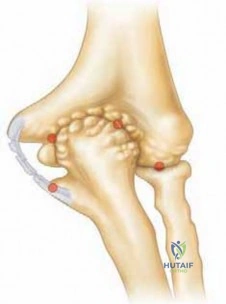
The bony articulation of the elbow joint provides primary stability to varus and valgus forces at the extremes of motion, specifically at angles of less than 20 degrees and greater than 120 degrees of flexion. The highly constrained nature of the ulnohumeral joint relies on the precise congruency between the trochlea of the distal humerus and the greater sigmoid notch of the proximal ulna. During terminal extension, the olecranon process locks into the olecranon fossa, providing substantial osseous stability against valgus stress.

Ligamentous Stabilizers
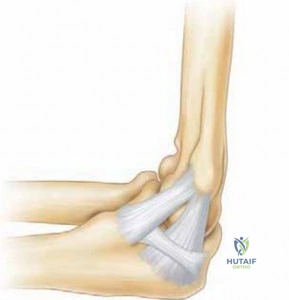
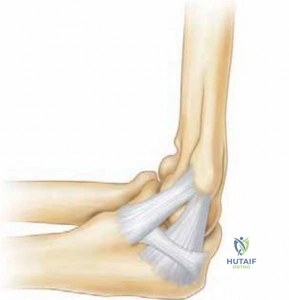
Soft tissues act as the chief stabilizers of the elbow between 20 and 120 degrees of flexion, which encompasses the functional arc where the majority of athletic activity occurs. The ulnar collateral ligament complex is the primary restraint to valgus stress. Anatomically, the UCL is composed of three distinct components: the anterior band, the posterior band, and the transverse ligament (Cooper ligament).
The anterior band is the most critical structure for valgus stability and is further subdivided into the anterior and posterior bundles, which perform reciprocal functions during the arc of motion. The anterior bundle is taut in extension and relaxes in flexion, whereas the posterior bundle is lax in extension and becomes taut in flexion. This reciprocal tensioning ensures continuous constraint against valgus loads throughout the functional range of motion.
Pathomechanics of Valgus Extension Overload
UCL insufficiency can be remarkably subtle. Ligament-sectioning studies have demonstrated only a 3-degree difference in valgus laxity when the anterior band of the UCL is completely transected. However, even microscopic attenuation of the UCL leads to abnormal valgus rotation of the elbow. This pathologic rotation dramatically alters the mechanics of the highly constrained posterior elbow joint.

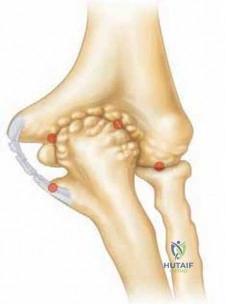
As the medial compartment distracts under valgus load, the olecranon process is driven forcefully into the posteromedial wall of the olecranon fossa. Chronic, repetitive bony impingement leads to reactive osteophyte formation on the posteromedial aspect of the olecranon and the corresponding fossa. Concurrently, the lateral compartment experiences excessive compressive forces, frequently resulting in radiocapitellar chondromalacia or osteochondral defects.
Indications and Contraindications
The management of valgus extension overload requires careful patient selection. Arthroscopic intervention is primarily indicated for patients who have failed an exhaustive course of non-operative management, including structured physical therapy, kinetic chain optimization, and non-steroidal anti-inflammatory medications.

A critical distinction must be made between isolated valgus extension overload and VEO occurring in the presence of gross UCL incompetence. Arthroscopic resection of posteromedial osteophytes in the setting of a high-grade UCL tear is strictly contraindicated unless performed concurrently with UCL reconstruction. The posteromedial osteophyte often acts as a secondary bony restraint to valgus stress in the UCL-deficient elbow; resecting it without addressing the ligamentous laxity will precipitate catastrophic iatrogenic valgus instability.

Operative vs Non Operative Management
| Clinical Scenario | Recommended Management Strategy | Rationale |
|---|---|---|
| Asymptomatic posteromedial osteophytes | Non-Operative | Incidental findings do not warrant surgical morbidity. |
| Symptomatic VEO failing 3-6 months of conservative care | Operative (Arthroscopic Resection) | Mechanical impingement requires structural decompression. |
| VEO with concurrent loose bodies | Operative (Arthroscopic Removal) | Loose bodies cause mechanical locking and progressive chondral damage. |
| VEO with high-grade UCL rupture | Operative (UCL Reconstruction + Scope) | Arthroscopy alone is contraindicated; ligamentous stability must be restored. |
| VEO with severe ulnar neuritis | Operative (Open Decompression/Transposition) | Isolated arthroscopy cannot adequately address compressive neuropathy. |
Pre Operative Planning and Patient Positioning
Clinical Evaluation
The classic presentation of valgus extension overload involves a patient complaining of a progressive loss of terminal extension accompanied by posterior or posteromedial elbow pain. Pitchers will characteristically report sharp, localized pain during the acceleration and follow-through phases of the throwing motion.
Physical examination must include a meticulous assessment of the UCL. The moving valgus stress test and the milking maneuver are highly sensitive for detecting subtle ligamentous insufficiency. Palpation of the posteromedial olecranon will often elicit point tenderness, and forced terminal extension will reproduce the patient's posterior impingement pain. A thorough neurologic examination is mandatory to rule out concurrent ulnar neuropathy, which frequently coexists due to the proximity of the ulnar nerve to the posteromedial osteophytes.

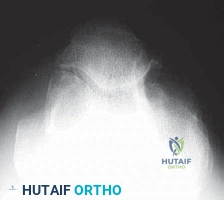
Imaging Modalities
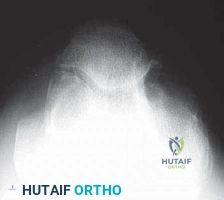
Standard radiographic evaluation includes anteroposterior, lateral, and axial views of the elbow. The axial view is particularly useful for visualizing posteromedial olecranon osteophytes. Computed tomography (CT) with 3D reconstruction provides superior osseous detail and is invaluable for preoperative surgical planning, allowing precise quantification of the osteophyte dimensions. Magnetic resonance arthrography (MRA) remains the gold standard for evaluating the integrity of the UCL and identifying associated chondral lesions within the radiocapitellar joint.

Patient Positioning Setup
Elbow arthroscopy for valgus extension overload can be performed in the lateral decubitus, prone, or supine suspended positions. The lateral decubitus position is heavily favored by many academic surgeons as it provides excellent access to both the anterior and posterior compartments while allowing the elbow to rest comfortably over a bolster at 90 degrees of flexion.
A non-sterile tourniquet is applied high on the brachium. The arm is prepped and draped in standard sterile fashion. Bony landmarks, including the medial and lateral epicondyles, the radial head, and the olecranon, are meticulously outlined with a surgical marker. The course of the ulnar nerve is also marked to maintain continuous spatial awareness during posterior portal placement.

Detailed Surgical Approach and Technique
Diagnostic Anterior Arthroscopy
The procedure typically begins with the establishment of the proximal anteromedial portal. The joint is insufflated with 20 to 30 mL of normal saline through the soft spot (center of the anconeus triangle) to distend the capsule and displace the neurovascular structures anteriorly. The proximal anteromedial portal is created 2 cm proximal and 1 cm anterior to the medial epicondyle, utilizing a "nick and spread" technique with a small hemostat to avoid injury to the medial antebrachial cutaneous nerve.

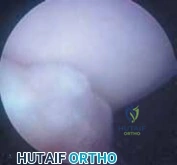
A 4.0-mm, 30-degree arthroscope is introduced, and a thorough diagnostic sweep of the anterior compartment is performed. The coronoid process, anterior capsule, and radiocapitellar joint are inspected. In the throwing athlete with VEO, it is common to observe chondromalacia on the capitellum or radial head secondary to lateral compressive forces. An anterolateral portal is established under direct intra-articular visualization to facilitate instrumentation and debridement of any anterior pathology.

Posterior Compartment Access
Following completion of the anterior work, the arthroscope is transitioned to the posterior compartment. A direct posterior portal is established 3 cm proximal to the olecranon tip, traversing the triceps tendon. A posterolateral portal is subsequently created just superior to the lateral epicondyle, adjacent to the lateral border of the triceps.
The posterior compartment is systematically evaluated. The olecranon fossa is cleared of fibrotic tissue and synovitis using a motorized shaver to expose the posteromedial osteophyte. The surgeon must maintain acute awareness of the ulnar nerve, which lies immediately medial to the posteromedial capsule. Aggressive suction or indiscriminate use of the shaver in the posteromedial gutter must be strictly avoided.

Arthroscopic Resection of Valgus Extension Overload
The core of the surgical intervention is the precise resection of the posteromedial olecranon osteophyte. A high-speed 4.0-mm motorized burr is introduced through the posterolateral portal while viewing from the direct posterior portal. The osteophyte is progressively resected until the normal anatomic contour of the olecranon is restored.

It is of paramount importance to avoid over-resection of the olecranon. Biomechanical studies have definitively demonstrated that resecting more than 3 to 4 mm of the native olecranon tip significantly increases the strain on the anterior bundle of the UCL. Over-resection effectively removes the osseous constraint that protects the ligament during terminal extension, precipitating iatrogenic valgus instability. The goal is strictly to remove the reactive osteophyte, not to perform a generalized olecranonectomy.
Dynamic evaluation is performed intraoperatively. The elbow is taken through a full range of motion, specifically bringing it into terminal extension with a valgus load applied. The surgeon observes the articulation to ensure that the impingement has been successfully eliminated and that the olecranon tracks smoothly into the fossa without engaging the medial wall. Any residual loose bodies within the olecranon fossa or posteromedial gutter are extracted.
Complications and Management
Arthroscopic management of valgus extension overload is generally safe, but complications can be profound if technical errors occur. The most devastating complication is iatrogenic valgus instability resulting from overzealous resection of the olecranon. If the surgeon inadvertently resects the native osseous constraint, the patient will experience increased valgus laxity, which typically necessitates a subsequent UCL reconstruction to salvage the athlete's career.

Neurologic injury is another significant concern. The ulnar nerve is highly vulnerable during instrumentation of the posteromedial gutter. The capsule in this region can be exceedingly thin or even deficient, placing the nerve at direct risk from shavers, burrs, or thermal ablation devices. Additionally, the medial antebrachial cutaneous nerve is at risk during the establishment of the proximal anteromedial portal, and the posterior interosseous nerve is at risk if the anterolateral portal is placed too distally.

Summary of Complications
| Complication | Estimated Incidence | Etiology | Salvage Strategy |
|---|---|---|---|
| Iatrogenic Valgus Instability | 2-5% | Resection of >3-4mm of native olecranon | UCL Reconstruction (Tommy John Surgery) |
| Ulnar Neuropathy | 1-3% | Direct trauma, thermal injury, or fluid extravasation | Observation vs. Ulnar Nerve Transposition |
| Portal Neuroma (MABC/LABC) | <1% | Poor portal placement or aggressive soft tissue spreading | Surgical excision and nerve burying |
| Postoperative Stiffness | 5-10% | Inadequate rehabilitation, capsular scarring | Aggressive physical therapy, static progressive splinting |
| Heterotopic Ossification | <1% | Aggressive bony resection, inadequate lavage | Excision once mature (typically 6-12 months post-op) |

Post Operative Rehabilitation Protocols
The postoperative rehabilitation protocol must be meticulously structured to restore full range of motion while protecting the dynamic and static stabilizers of the elbow.
Phase 1 Immediate Postoperative Period
During the first 7 to 10 days, the primary goals are to minimize edema, control pain, and prevent capsular contracture. The elbow is placed in a soft compressive dressing. Immediate active and active-assisted range of motion exercises are initiated. Cryotherapy is utilized aggressively. Immobilization is strictly avoided to prevent postoperative stiffness, which is a common sequela of elbow arthroscopy.
Phase 2 Intermediate Rehabilitation
From weeks 2 through 6, the focus shifts to restoring full terminal extension and initiating isotonic strengthening of the flexor-pronator mass and the triceps. Scapular stabilization and core strengthening—essential components of the overhead athlete's kinetic chain—are heavily emphasized. By the end of week 6, the patient should possess full, painless range of motion.
Phase 3 Return to Play
At approximately 6 to 8 weeks postoperatively, assuming the patient has full strength and no pain with provocative testing, an interval throwing program is initiated. This program gradually increases throwing distance and volume over a 4 to 6 week period. Pitchers typically begin throwing off the mound at 10 to 12 weeks, with a full return to competitive play expected between 3 and 4 months following isolated arthroscopic osteophyte resection.