Masterclass in Complex Elbow Trauma: Radial Head and Olecranon Fracture-Dislocations

Key Takeaway
The management of radial head and olecranon fractures associated with elbow dislocations requires a profound understanding of elbow biomechanics. This guide details evidence-based surgical protocols, including radial head arthroplasty, coronoid reconstruction, and advanced plate-and-screw fixation for complex ulnohumeral instability. Emphasizing anatomical restoration and early mobilization, these techniques are critical for mitigating post-traumatic stiffness and achieving optimal functional outcomes in complex elbow trauma.
Comprehensive Introduction and Patho-Epidemiology
The management of radial head and neck fractures in the setting of an acute elbow dislocation remains one of the most challenging paradigms in orthopedic traumatology. These complex injury patterns, which frequently encompass the dreaded "terrible triad" of the elbow, transolecranon fracture-dislocations, and Monteggia variants, demand a profound understanding of elbow kinematics and osseous anatomy. Historically, the treatment of these injuries was fraught with high rates of chronic instability, post-traumatic osteoarthritis, and catastrophic stiffness. However, the modern era of orthopedic surgery has heralded a paradigm shift from simple excision and prolonged immobilization to aggressive, anatomically precise reconstruction and early, active mobilization.
The epidemiology of complex elbow trauma demonstrates a bimodal distribution. High-energy mechanisms, such as motor vehicle collisions or falls from significant heights, predominantly affect young, active males, resulting in severe comminution and profound soft tissue compromise. Conversely, low-energy falls from a standing height are increasingly responsible for these injuries in the osteopenic elderly population, particularly post-menopausal females. The pathophysiological mechanism typically involves a combination of axial loading, supination, and valgus stress applied to a partially flexed elbow. This cascade of forces sequentially disrupts the lateral collateral ligamentous complex, the anterior and posterior capsule, and finally the medial collateral ligament, as classically described by O'Driscoll's circle of soft tissue disruption.
When the primary ligamentous restraints are disrupted during a dislocation event, the osseous architecture of the radial head and the coronoid process becomes the primary buttress against joint subluxation. The radial head functions as a critical secondary stabilizer, working synergistically with the anterior band of the medial collateral ligament (MCL) to resist valgus stress, and with the lateral ulnar collateral ligament (LUCL) to resist posterolateral rotatory instability (PLRI). Therefore, the presence of a radial head or olecranon fracture in the context of a dislocation fundamentally alters the biomechanical environment, converting a purely soft-tissue injury into a highly unstable osseous-ligamentous disruption that mandates meticulous surgical intervention.
Failure to recognize the subtle nuances of these fracture-dislocations often leads to devastating clinical outcomes. A misdiagnosis of a transolecranon fracture-dislocation as a simple olecranon fracture, for instance, may result in inadequate fixation of the coronoid process, leading to immediate postoperative ulnohumeral subluxation. Consequently, the contemporary orthopedic surgeon must approach these injuries with a high index of suspicion, utilizing advanced cross-sectional imaging to delineate the exact fracture morphology and meticulously planning a surgical strategy that sequentially restores the osseous and ligamentous stabilizers of the elbow joint.
Detailed Surgical Anatomy and Biomechanics
A masterful comprehension of elbow anatomy and biomechanics is the absolute prerequisite for successfully navigating complex fracture-dislocations. The elbow is a highly constrained, ginglymoarthrodial joint composed of three distinct articulations: the ulnohumeral, radiocapitellar, and proximal radioulnar joints. The stability of this complex is traditionally divided into primary and secondary constraints. The primary constraints include the highly congruent ulnohumeral articulation, the anterior bundle of the medial collateral ligament (AMCL), and the lateral collateral ligament (LCL) complex, specifically the lateral ulnar collateral ligament (LUCL). The secondary constraints encompass the radial head, the common flexor and extensor origins, and the dynamic compressive forces generated by the musculature crossing the joint.
The radial head plays an indispensable role in load transfer and kinematic stability. In a fully extended elbow, approximately 60% of the axial load is transmitted across the radiocapitellar joint. The radial head acts as the primary secondary stabilizer to valgus stress; in the setting of an AMCL deficiency, the radial head provides up to 30% of the resistance to valgus displacement. Furthermore, the radial head is vital in preventing posterior translation of the radius and ulna relative to the humerus. The articular surface of the radial head is not perfectly circular but rather elliptical, and it possesses a "bare area" devoid of hyaline cartilage on its non-articulating anterolateral margin, which serves as the safe zone for hardware placement during internal fixation.
The proximal ulna, comprising the olecranon and coronoid processes, forms the greater sigmoid notch, which intimately articulates with the humeral trochlea. The olecranon serves as the insertion site for the triceps brachii, functioning as the primary extensor mechanism of the elbow. Biomechanically, the olecranon prevents anterior translation of the ulna relative to the distal humerus. The coronoid process, conversely, is the critical anterior buttress. It is divided into the tip, body, anteromedial facet, and sublime tubercle. The sublime tubercle serves as the insertion footprint for the AMCL, while the anteromedial facet provides essential varus and posteromedial rotatory stability. Fractures involving the base of the coronoid profoundly destabilize the ulnohumeral joint and must be rigidly addressed.
Understanding the kinematic chain of the elbow is crucial during surgical reconstruction. The axis of rotation of the elbow passes through the center of the capitellum and the anteroinferior aspect of the medial epicondyle. Any surgical intervention, whether it be radial head arthroplasty or olecranon plating, must meticulously restore this axis. Overstuffing the radiocapitellar joint with an oversized radial head prosthesis, for example, will gap the lateral joint line, increase tension on the LCL repair, and lead to premature capitellar wear, stiffness, and chronic pain. Similarly, failure to anatomically reduce the contour of the greater sigmoid notch during olecranon fixation will result in altered contact mechanics, rapidly accelerating post-traumatic arthropathy.
Exhaustive Indications and Contraindications
The decision-making algorithm for complex elbow trauma hinges on a precise evaluation of joint stability, fracture comminution, and patient-specific physiological factors. The overarching goal is to achieve a concentrically reduced, stable joint that permits immediate active range of motion. Prolonged immobilization in the setting of complex elbow trauma is universally condemned, as it leads to irreversible capsular contracture and profound functional deficit.
| Clinical Scenario | Primary Indications for Operative Intervention | Relative/Absolute Contraindications |
|---|---|---|
| Radial Head Fracture in Dislocation | Any displaced fracture (>2mm) causing a mechanical block; Mason Type II/III with concomitant ligamentous disruption; Inability to achieve concentric reduction. | Truly undisplaced fractures (rare in dislocation); Medically unfit patients (absolute); Active joint infection (absolute). |
| Olecranon Fracture-Dislocation | Disruption of the extensor mechanism; Articular step-off >2mm; Transolecranon fracture-dislocations; Monteggia variants; Coronoid involvement. | Non-ambulatory, low-demand patients with minimal displacement (relative); Severe, untreatable medical comorbidities. |
| Tension Band Wiring (Olecranon) | Simple, transverse fractures (Schatzker Transverse); Intact coronoid and radial head; Exceptional soft tissue compromise requiring low-profile implants. | Comminuted fractures; Oblique fractures; Distal extension; Concomitant elbow instability (absolute contraindications). |
| Plate Osteosynthesis (Olecranon) | Comminuted fractures; Oblique/distal fracture patterns; Fracture-dislocations; Coronoid basal fractures requiring lag screw fixation through the plate. | Active overlying skin infection; Inadequate soft tissue envelope precluding coverage (requires flap first). |
| Radial Head Arthroplasty | Unsalvageable radial head (>3 articular fragments) in the setting of MCL/LCL disruption or coronoid fracture; Essex-Lopresti injuries. | Salvageable radial head amenable to ORIF; Isolated radial head fractures without instability (relative); Children/adolescents with open physes. |
Operative intervention is strongly indicated for nearly all radial head and olecranon fractures associated with elbow dislocations. Open Reduction and Internal Fixation (ORIF) of radial head fractures is always preferable to excision if the radial head is anatomically salvageable (typically defined as fewer than three articular fragments without severe metaphyseal comminution). If the radial head is deemed unsalvageable and must be excised, the surgeon must acutely address the resulting valgus and posterolateral rotatory instability. In this scenario, the medial collateral ligament (MCL) and the flexor-pronator mass must be meticulously repaired, and a metallic radial head implant (arthroplasty) is strongly considered—and often mandated—to act as a temporary or permanent spacer to maintain lateral column length.
Contraindications to immediate internal fixation primarily revolve around severe physiological instability (damage control orthopedics) or catastrophic soft tissue envelopes. In cases of severe open fractures with massive soft tissue loss, spanning external fixation across the elbow joint may be utilized as a temporizing measure until the soft tissue bed is optimized for definitive internal fixation. Furthermore, patient compliance is a critical, albeit subjective, indication; patients who are unable or unwilling to participate in the rigorous postoperative rehabilitation protocol may experience suboptimal outcomes regardless of the surgical perfection achieved in the operating theater.
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the cornerstone of successful outcomes in complex elbow trauma. Standard orthogonal anteroposterior (AP) and lateral radiographs of the elbow are mandatory, but they are frequently insufficient for fully characterizing the extent of articular comminution and occult coronoid involvement. Therefore, a fine-cut Computed Tomography (CT) scan with 3D reconstructions is considered the gold standard and is universally recommended for all fracture-dislocations of the elbow. The CT scan allows the surgeon to conceptualize the fracture fragments in three dimensions, specifically assessing the size of the coronoid fragment, the degree of radial head comminution, and the presence of marginal impaction within the greater sigmoid notch.
Digital templating is an essential component of the preoperative workflow. The surgeon must anticipate the need for various implant systems, including mini-fragment screws (1.5mm, 2.0mm, 2.4mm) for radial head and coronoid fixation, anatomically precontoured proximal ulna plates, and a modular radial head arthroplasty system. Anticipating the trajectory of lag screws for the coronoid—whether they will be placed from posterior to anterior through the proximal ulna or anterior to posterior—dictates the surgical approach and plate selection. Furthermore, the contralateral uninjured elbow should be radiographed to serve as a template for restoring the anatomical ulnar bow and assessing the native radiocapitellar joint space.
Patient positioning is critical for optimizing surgical exposure and facilitating intraoperative fluoroscopy. The two most common positions are the lateral decubitus position and the supine position with the arm draped across the chest. In the lateral decubitus position, the patient is secured with a beanbag, and the injured arm is draped over a padded L-bar or a dedicated elbow positioner. This allows for excellent access to the posterior and lateral compartments of the elbow and facilitates gravity-assisted reduction of the triceps. Alternatively, the supine position with the arm draped across the chest is highly effective, particularly in polytrauma patients who cannot be turned laterally. A sterile tourniquet is routinely applied to the proximal arm to ensure a bloodless surgical field, inflated only after exsanguination and careful padding to protect the radial nerve.
Intraoperative fluoroscopy must be positioned to allow unhindered orthogonal views of the elbow without compromising the sterile field. The C-arm is typically brought in parallel to the operating table, coming from the head or the opposite side of the patient. The surgeon must confirm that true lateral views (demonstrating concentric overlapping of the capitellum and trochlea) and true AP views can be easily obtained before the incision is made. Failure to optimize the fluoroscopic setup preoperatively invariably leads to intraoperative frustration, prolonged surgical time, and an increased risk of malreduction.
Step-by-Step Surgical Approach and Fixation Technique
The surgical management of combined radial head and olecranon fracture-dislocations requires a highly structured, algorithmic approach. A universal posterior skin incision is the workhorse approach, accommodating access to both the medial and lateral columns while minimizing the risk of devitalizing skin flaps. The incision is centered just lateral to the tip of the olecranon, curving gently to avoid crossing the apex of the olecranon directly, which can lead to painful postoperative scarring. Full-thickness fasciocutaneous flaps are meticulously elevated to preserve the delicate vascular supply to the posterior skin.
Radial Head Management in Dislocation Settings
Access to the radial head is typically achieved through either the Kocher interval (between the extensor carpi ulnaris and the anconeus) or the Kaplan interval (between the extensor digitorum communis and the extensor carpi radialis brevis). In the setting of a dislocation, the lateral soft tissues are often already avulsed, and the surgeon can simply utilize the traumatic rent in the extensor origin to access the joint.
If the radial head is salvageable, ORIF is performed using headless compression screws or low-profile plates applied to the safe zone. If excision is necessary, the surgeon must acutely address the resulting instability.
Surgical Pearl: The "Back-Table" Reconstruction
If radial head excision is necessary, the excised fragments must be reconstructed on the sterile back table. This is a critical step to ensure that no osteochondral fragments are retained within the joint space, which could lead to mechanical blocking, third-body wear, or post-traumatic osteoarthritis.
Today, the use of a metallic radial head implant (arthroplasty) is strongly considered—and often mandated—if instability persists. The prosthesis acts as a crucial temporary or permanent spacer to maintain the lateral column length and provide a valgus buttress. Sizing the prosthesis is paramount; the implant must articulate concentrically with the capitellum without overstuffing the joint. The proximal articular surface of the implant should sit flush with or 1-2 mm distal to the lateral edge of the coronoid process.
Olecranon Fractures and Schatzker Classification
Olecranon fractures disrupt the extensor mechanism of the elbow and compromise the primary ulnohumeral articulation. Schatzker classified olecranon fractures based on the fracture pattern and the mechanical considerations required for internal fixation. Understanding this classification is paramount for selecting the appropriate osteosynthesis construct.
Transverse Fracture Pattern:

Transverse-Impacted Fracture Pattern:

Oblique Fracture Pattern:

Comminuted Fracture Pattern:
Oblique-Distal Fracture Pattern:
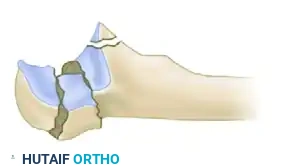
Fracture-Dislocation Pattern:
Historically, the tension band wiring technique was the workhorse for simple, transverse olecranon fractures. The biomechanical principle relies on converting the tensile forces of the triceps on the posterior cortex into compressive forces across the articular surface at the sigmoid notch. However, this procedure is fraught with complications, primarily symptomatic hardware requiring removal.
Surgical Warning: Neurovascular Injury
When utilizing Kirschner wires to anchor the tension band, there is a distinct risk of injury to the neurovascular structures in the anterior forearm if the wires overpenetrate the anterior ulnar cortex. Transcortical placement rather than purely intramedullary placement increases stability but requires precise depth control.
Plate fixation is the contemporary treatment of choice, offering superior biomechanical stability. It is specifically indicated for fractures with comminution, distal extensions, and complex fracture-dislocations. Typically applied in a neutralization mode, the plating technique allows for independent lag screw fixation of the olecranon and/or coronoid fragments.
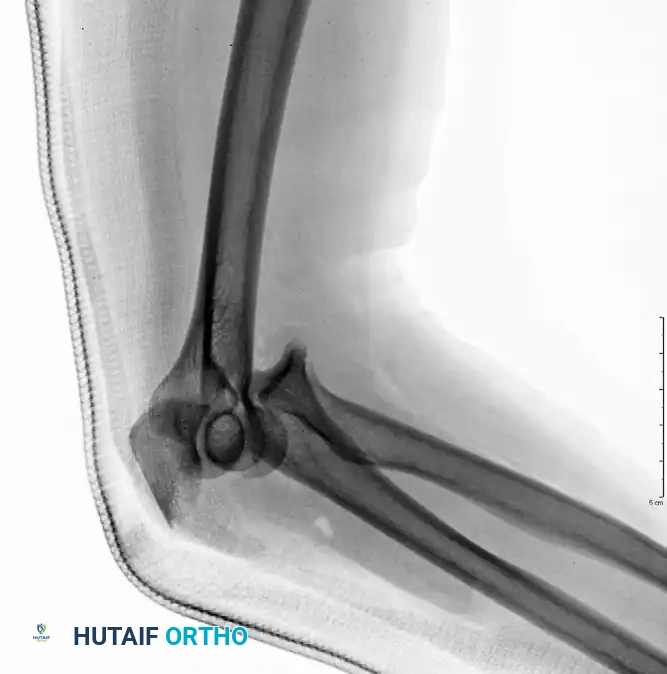
Preoperative Injury - Olecranon Fracture-Dislocation:

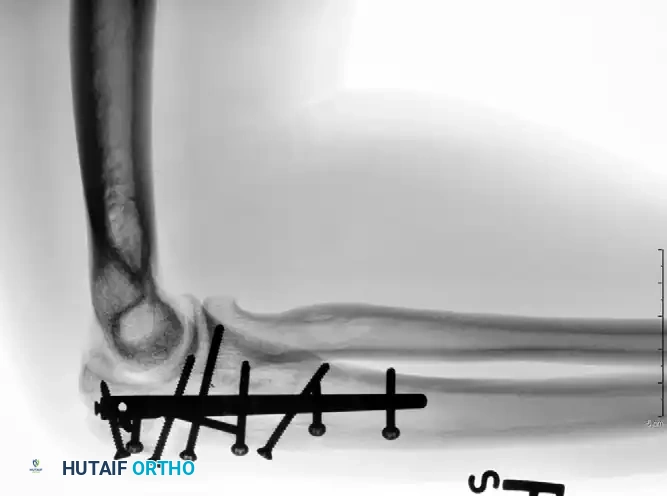
Fixation with Lag Screw and Plate (AP View):

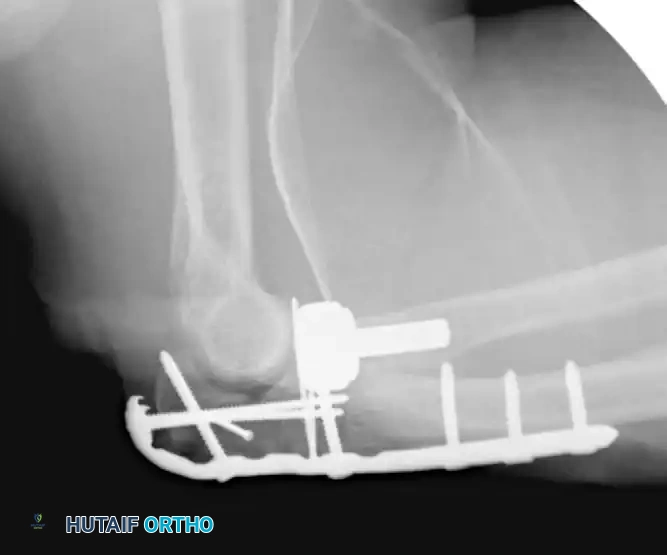
Fixation with Lag Screw and Plate (Lateral View):
Modern precontoured plates are anatomically designed, lower in profile, and feature locking screw capabilities. Biomechanical testing confirms that these plates provide significantly greater compression than tension bands.
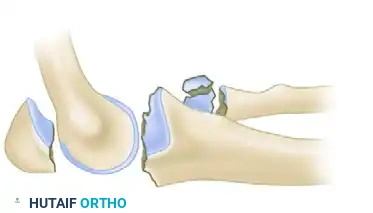
Complex Olecranon Fracture-Dislocation (Injury):
Fixation with Low-Profile Plate (AP View):

Fixation with Low-Profile Plate (Lateral View):

Transolecranon and Posterior Fracture-Dislocations
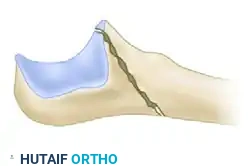
In an anterior transolecranon fracture-dislocation, the mechanism involves the distal humerus imploding through the olecranon. Crucially, the proximal radioulnar joint (PRUJ) remains anatomically preserved, and the collateral ligaments are typically intact. The routine treatment protocol demands anatomical reconstruction of the greater sigmoid notch articular surface followed by rigid plate fixation. The coronoid must be reduced and stabilized with lag screws first, followed by a robust plate spanning the entire zone of injury.
Preoperative Transolecranon Fracture-Dislocation:
Fixation with Lag Screws and Plate Spanning Entire Injury (AP View):
Fixation with Lag Screws and Plate Spanning Entire Injury (Lateral View):

Fixation with Lag Screws and Plate Spanning Entire Injury (Oblique View):

Posterior dislocations involve both ulnohumeral and radioulnar disruption (Monteggia variants). Beingessner et al. outlined a definitive 6-step approach:
1. Radial Head Management (repair or replacement).
2. Ulnar Shaft Reduction.
3. Coronoid Stabilization (using anterior-to-posterior screws or transosseous sutures).
4. Olecranon Fixation (definitive plate fixation).
5. Ligamentous Repair (Distal insertions).
6. Ligamentous Repair (Proximal humeral origins).
Intramedullary Nailing Techniques
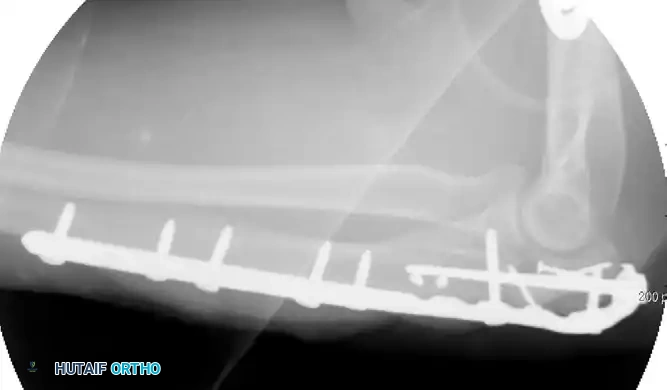
Recently, there has been a resurgence of interest in the use of intramedullary (IM) nails for the treatment of proximal ulna and olecranon fractures. The biomechanical advantage of IM nailing lies in its load-sharing capacity and minimal soft tissue disruption, which is highly advantageous in patients with compromised posterior skin envelopes.
More advanced, dedicated implants have since been developed, such as multiplanar locking intramedullary nails, which demonstrate high efficacy for the treatment of proximal olecranon fractures, including those presenting with complex, multi-directional instability patterns.
Complex Fracture-Dislocation of the Elbow (Pre-op AP):

Complex Fracture-Dislocation of the Elbow (Pre-op Lateral):

Fixation with Multiplanar Locking Intramedullary Nail (Post-op AP):

Fixation with Multiplanar Locking Intramedullary Nail (Post-op Lateral):
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, the management of complex elbow fracture-dislocations is associated with a formidable complication profile. The elbow joint is notoriously unforgiving, with a robust propensity for capsular fibrosis and heterotopic ossification (HO). The surgeon must maintain a proactive stance in identifying and mitigating these complications early in the postoperative course.
| Complication | Estimated Incidence | Pathophysiology & Clinical Management |
|---|---|---|
| Post-Traumatic Stiffness | 30% - 60% | The most common complication. Driven by capsular contracture and prolonged immobilization. Treated initially with static progressive splinting. Refractory cases require open or arthroscopic capsular release after 6-12 months. |
| Symptomatic Hardware | 10% - 80% | Highest with tension band wiring (up to 80%). Modern low-profile plating has reduced this to <15%. Managed with elective hardware removal once radiographic union is confirmed (typically >6 months). |
| Heterotopic Ossification | 10% - 35% | Formation of lamellar bone in periarticular soft tissues. High risk in head trauma or delayed fixation. Prophylaxis includes Indomethacin or single-dose localized radiation. Excision delayed until bone matures (normal alkaline phosphatase). |
| Ulnar Neuropathy | 5% - |
