Masterclass in Elbow Arthroplasty: Biomechanics, Surgical Techniques, and Clinical Outcomes

Key Takeaway
Elbow arthroplasty aims to restore a painless, functional arc of motion in patients with inflammatory or degenerative arthritis. Success relies on meticulous patient selection, understanding of the complex ginglymoarthrodial biomechanics, and precise surgical execution. This guide covers the historical evolution, anatomical considerations, and step-by-step surgical techniques for modern semiconstrained and unconstrained elbow prostheses, providing orthopedic surgeons with evidence-based protocols for optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Although extremity arthroplasty has been performed for over 150 to 200 years, the elbow remains one of the most unforgiving, anatomically complex, and biomechanically demanding joints to reconstruct. To date, no single arthroplasty design has been developed that universally meets the needs of every patient with a disabled elbow joint. The primary goal—restoration of a painless, functional arc of elbow motion in active individuals with inflammatory or degenerative arthritis—is often incomplete due to the inherent constraints of the soft-tissue envelope and the extraordinary forces transmitted across the articulation.
In lower-demand individuals, such as elderly patients with advanced rheumatoid arthritis or those suffering from catastrophic, un-reconstructible distal humerus fractures, total elbow arthroplasty (TEA) provides excellent, reproducible pain relief and functional restoration. However, careful patient selection is paramount. The epidemiological landscape of elbow arthroplasty has shifted significantly over the past three decades. Historically, the vast majority of TEAs were performed for severe rheumatoid arthritis. With the advent of disease-modifying antirheumatic drugs (DMARDs) and biologic therapies, the incidence of severe rheumatoid elbow destruction has plummeted. Consequently, the contemporary indications have expanded to include post-traumatic osteoarthritis (PTOA), distal humeral nonunions, and acute comminuted intra-articular fractures in the osteoporotic elderly population.
This demographic shift brings profound clinical implications. Patients with post-traumatic conditions often present with compromised soft-tissue envelopes, distorted bony anatomy, retained hardware, and latent subclinical infections. As a result, the complication rates for elbow implant arthroplasty remain substantially higher than those for hip or knee arthroplasty. Managing these complex complications—such as aseptic loosening, periprosthetic joint infection (PJI), periprosthetic fractures, and triceps insufficiency—requires advanced reconstructive expertise, meticulous preoperative planning, and a profound understanding of elbow kinematics.
Historical Evolution of Elbow Reconstruction
The historical development of elbow arthroplasty can be viewed through four distinct eras, as originally categorized by Coonrad. Understanding these eras provides critical insight into the biomechanical rationale behind modern implant designs and the etiology of historical failures.
Era 1: Resection and Anatomical Arthroplasty (1885–1947)
Resection arthroplasty, pioneered by Verneuil and Ollier in the 1800s, involved the radical removal of the entire elbow joint via distal humeral and proximal radioulnar resection.
While its use in post-tuberculous ankylosis effectively eradicated infection, it rendered the elbow grossly unstable and functionally devastating. Nevertheless, in the 1930s, Buzby recommended it strictly for pain control in desperate cases. A variation known as "functional arthroplasty" involved a wedge-shaped distal humeral resection left as a fulcrum for the proximal ulna. Advocated by Hass, this technique is now primarily reserved as a salvage procedure following catastrophic infection or failed arthroplasty.
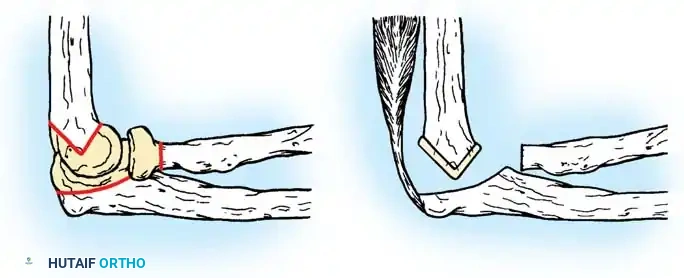
In anatomical arthroplasty, only the articular surfaces were removed, exposing the underlying cancellous bone. To minimize ankylosis, biological interposition materials were popularized in Europe by Payr and Putti. In the United States, Murphy introduced arthroplasty in the 1900s, and Lexer advocated for fascia and fat interposition. In 1918, Baer experimented with materials ranging from zinc and silicone to chromicized pig bladder (Baer membrane). Ultimately, fascia lata became the most popular interpositional substance due to its ease of harvest and minimal donor-site morbidity, yielding acceptable early results in select series.
Era 2: Constrained Hinge Arthroplasty (1947–1970)
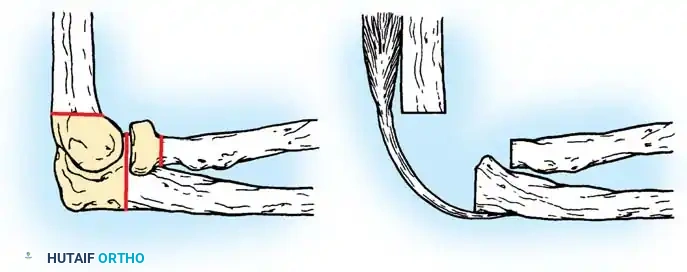
Despite successes with interpositional arthroplasty, efforts shifted toward replacing the joint entirely. Early designs included metal for the olecranon, acrylic for the lower humerus, and Vitallium for the radial head. Metal-to-metal hinged prostheses emerged but frequently failed. Because these rigid hinges lacked an anatomical center of rotation and failed to account for the complex varus-valgus toggle during flexion, they severely limited motion and transmitted massive, unmitigated stresses directly to the bone-implant interface. This inevitably led to rapid aseptic loosening, massive osteolysis, skin breakdown, and triceps tendon ruptures.

Era 3: Polymethyl Methacrylate Fixation (1970–1975)
Dee initiated the third major era by utilizing polymethyl methacrylate (PMMA) bone cement to fix metal-to-metal hinged prostheses. While short-term results were highly encouraging, the fundamental biomechanical flaw remained: rigid constraint combined with rigid PMMA fixation simply accelerated catastrophic implant loosening within 2 to 3 years. The cement mantle could not withstand the cyclical torsional loads, and these designs were largely abandoned.
Era 4: Modern Prosthetic Design (1975–Present)
Since 1975, two dominant prosthetic philosophies have evolved to address the biomechanical failures of rigid hinges, leading to the durable implants utilized today:
- Semiconstrained Metal-to-Polyethylene Hinges: Implants such as the Mayo, Coonrad-Morrey, GSB III, and Discovery designs incorporate a "sloppy hinge." This ingenious design allows 7 to 10 degrees of varus-valgus and rotational laxity, effectively dissipating stresses away from the cement-bone interface and transferring them into the surrounding soft tissues and the polyethylene bushing.
- Unconstrained Resurfacing Arthroplasties: Implants like the Ewald capitellocondylar, Kudo, and Souter-Strathclyde rely entirely on intact capsuloligamentous structures and balanced musculature for stability, mimicking unicompartmental or total knee resurfacing principles.
Modern semiconstrained implant design.

Modern unconstrained implant design.
Detailed Surgical Anatomy and Biomechanics
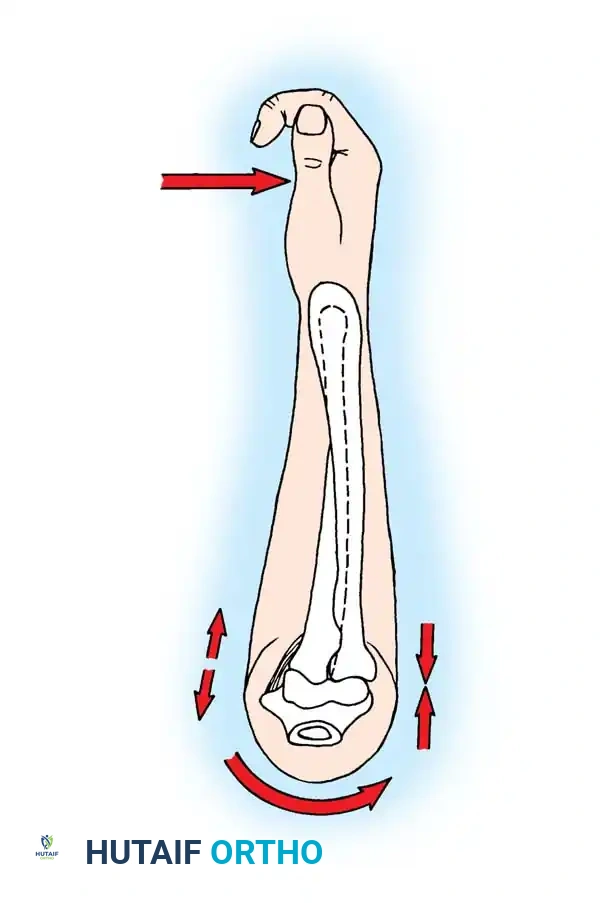
The elbow is a highly congruent ginglymoarthrodial (hinge-pivot) joint composed of two independent uniaxial articulations: the humeroulnar joint (ginglymoid) and the radiocapitellar/proximal radioulnar joint (trochoid). This complex architecture allows two degrees of freedom: flexion-extension and pronation-supination. Understanding the intricate balance between osseous anatomy and soft-tissue restraints is non-negotiable for the reconstructive surgeon.
Capsuloligamentous Stabilizers
Stability of the elbow is maintained by a delicate, dynamic interplay of joint geometry (the primary static stabilizer in extension), capsuloligamentous integrity, and dynamic muscle forces (biceps, brachialis, anconeus, triceps).
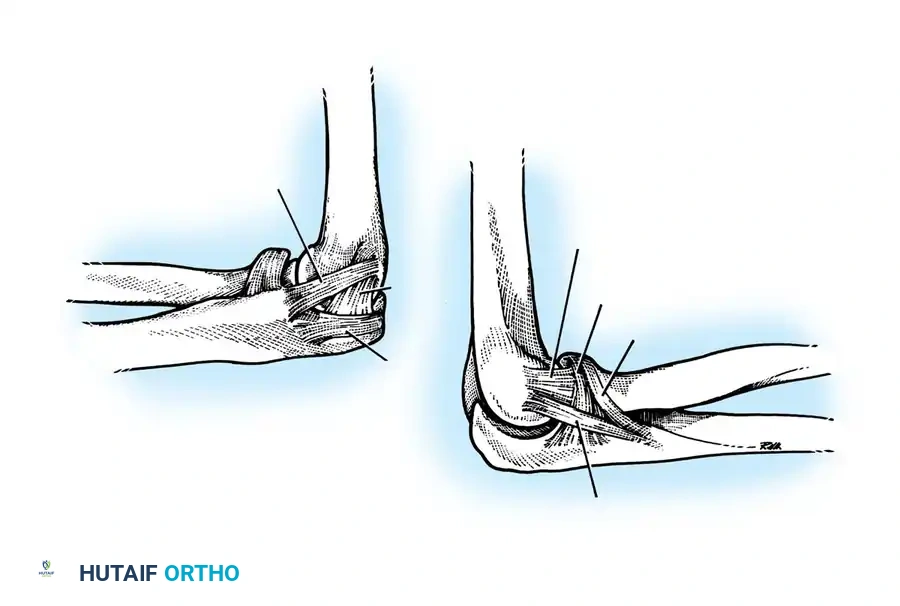
The Medial Collateral Ligament (MCL) complex consists of anterior, posterior, and transverse bundles. The anterior bundle is the primary restraint to valgus stress and remains taut throughout the entire flexion-extension arc. It originates from the anteroinferior surface of the medial epicondyle and inserts onto the sublime tubercle of the coronoid process.
The Lateral Collateral Ligament (LCL) complex, as definitively described by Morrey, includes the radial collateral ligament, the lateral ulnar collateral ligament (LUCL), the accessory lateral collateral ligament, and the annular ligament. The LUCL is the critical structure preventing posterolateral rotatory instability (PLRI). It originates from the lateral epicondyle, extends superficial to the annular ligament, and inserts on the crista supinatorius of the proximal ulna. Disruption of this ligament during surgical exposure without meticulous repair is a primary cause of postoperative instability in unconstrained arthroplasty.
Kinematics and Joint Reaction Forces
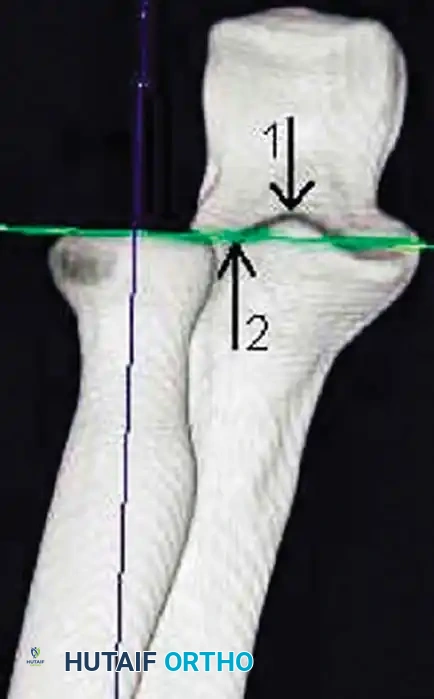
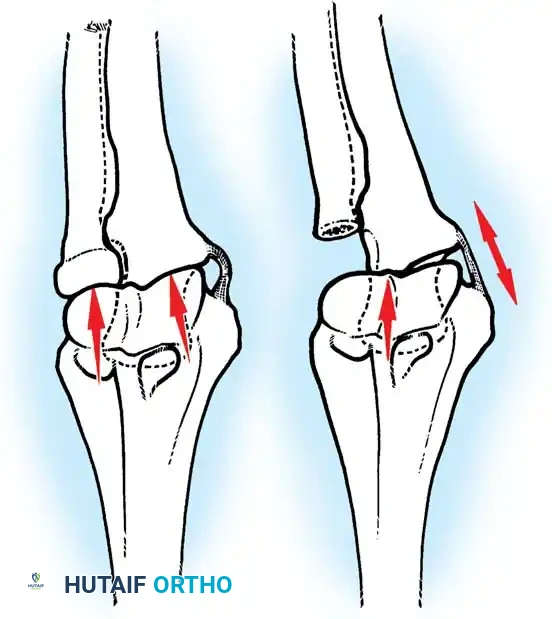
The instantaneous center of rotation for elbow flexion and extension is remarkably constant. It lies at the center of concentric circles formed by the lateral projection of the capitellum and the medial projection of the trochlea, passing colinearly with the anterior cortex of the distal humerus.
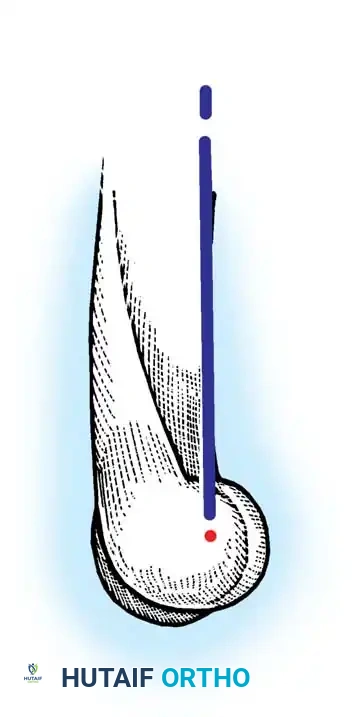
The carrying angle varies dynamically, moving from approximately 11 degrees of valgus in full extension to 6 degrees of varus in full flexion. This dynamic shift is exactly what rigid historical hinges failed to accommodate, leading to their demise. When placing an unconstrained prosthesis, recreating this exact anatomical axis of rotation is mandatory. Failure to do so results in eccentric loading, rapid accelerated polyethylene wear, and early clinical failure.
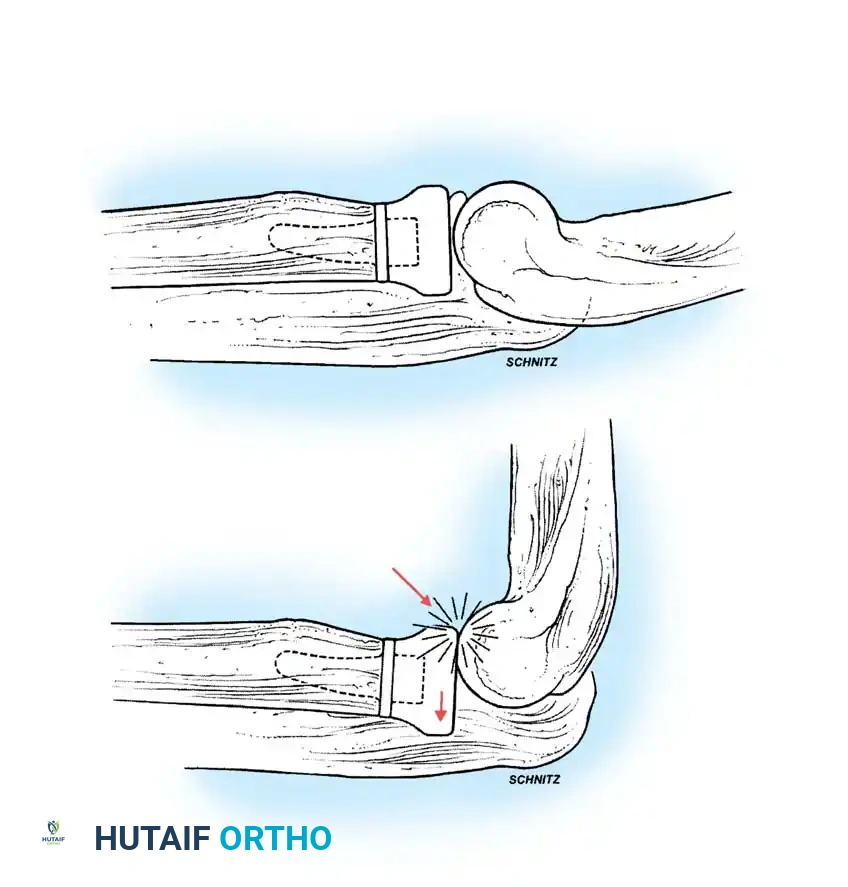
Joint reaction forces at the elbow are surprisingly high, often underappreciated by surgeons accustomed to weight-bearing joints. Static analyses reveal that forces are greatest in extension and pronation. During strenuous lifting or pushing up from a chair, compressive forces across the joint can reach up to three times body weight.
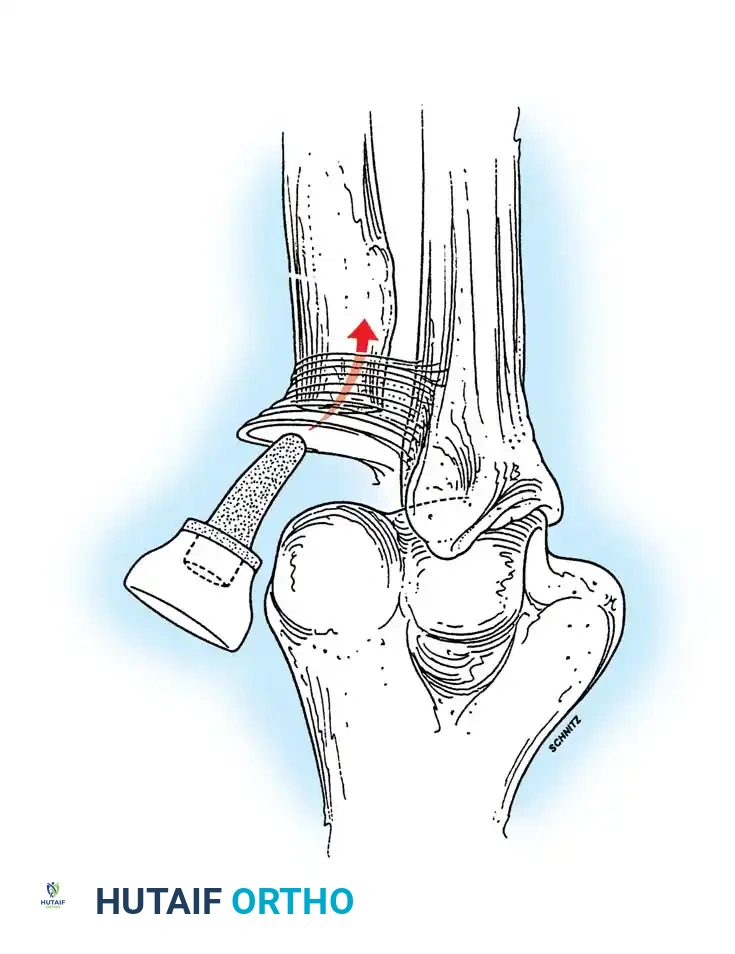
With the elbow extended and axially loaded, 40% of the stress is transmitted through the ulnohumeral joint, and 60% through the radiocapitellar joint. If the radial head is excised—a common maneuver in complex trauma or rheumatoid reconstruction—the humeroradial force is entirely shifted to the ulna. This drastically increases tension on the MCL and concentrates massive loads on the lateral edge of the coronoid process, potentially applying forces up to nine times body weight to the medial structures.
Principles of Soft-Tissue Balancing
Soft-tissue balancing is as critical in the elbow as it is in any major joint reconstruction. While historical texts (such as Wiater and Levine's work on shoulder arthroplasty) note that a 1 cm gain in anterior capsular length increases external rotation by 20 degrees, the analogous principle applies to the elbow: meticulous release of the anterior capsule is required to restore extension, while posterior capsular release is necessary to restore flexion.
Intracapsular and extracapsular releases must be balanced perfectly to prevent iatrogenic instability, particularly when utilizing unconstrained implants. The brachialis muscle often becomes fibrotic and contracted in chronic arthritis; careful fractional lengthening or radical anterior capsulectomy may be required to achieve a functional extension arc (typically defined as lacking no more than 30 degrees of full extension).
Exhaustive Indications and Contraindications
Patient selection is the single most critical determinant of survivorship in elbow arthroplasty. The ideal candidate is a low-demand, older individual (>65 years) with severe, debilitating pain and functional limitation that has failed exhaustive conservative management. High-demand, young laborers are exceptionally poor candidates due to the universal lifetime lifting restrictions (typically 5-10 lbs) imposed after TEA.
Primary Indications
- Rheumatoid Arthritis (RA): Advanced Larsen grade IV or V RA with severe joint destruction, instability, and intractable pain. These patients typically achieve excellent pain relief and functional restoration, as their polyarticular disease naturally limits upper extremity loading.
- Post-Traumatic Osteoarthritis (PTOA): Chronic pain and stiffness following trauma. These cases are technically demanding due to altered anatomy, retained hardware, and compromised soft tissues.
- Acute Distal Humerus Fractures: Comminuted, intra-articular fractures (AO Type 13-C3) in osteoporotic patients over the age of 65. TEA allows immediate weight-bearing through the arm for transfers and avoids the high failure rates of osteosynthesis in poor-quality bone.
- Distal Humeral Nonunions: Chronic nonunions in the elderly where bone stock is insufficient for revision internal fixation.
Absolute and Relative Contraindications
Absolute contraindications must be strictly respected to avoid catastrophic failure. Active or latent periprosthetic joint infection (PJI) is an absolute contraindication to primary arthroplasty. Neuropathic joints (Charcot arthropathy) will rapidly destroy any implant.
| Category | Specific Conditions | Clinical Rationale |
|---|---|---|
| Absolute Contraindications | Active systemic or local infection | High risk of PJI; requires two-stage management if pre-existing. |
| Neuropathic (Charcot) joint | Absence of proprioception leads to rapid catastrophic implant loosening and fracture. | |
| Paralysis of the extremity | Lack of dynamic muscular stabilization renders the limb non-functional regardless of joint mechanics. | |
| High-demand physical labor | Exceeding 5-10 lb lifting restrictions guarantees early aseptic loosening and bushing wear. | |
| Relative Contraindications | Young patient age (<60 years) | High cumulative lifetime load risk; arthrodesis or interposition may be considered. |
| Severe soft-tissue compromise | Prior flaps or radiation increase risk of wound breakdown; requires plastic surgery consultation. | |
| History of prior elbow infection | Requires extensive workup (ESR, CRP, aspiration) to rule out indolent organisms. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative templating is essential to assess bone stock, canal diameter, and the presence of deformity. The elbow's narrow medullary canals and complex diaphyseal bows leave little room for error during reaming and broaching.
Clinical Evaluation and Imaging Modalities
Standard anteroposterior (AP) and lateral radiographs are mandatory. The AP view must be evaluated for medial/lateral epicondylar bone stock, while the lateral view assesses the true anterior bow of the distal humerus and the proximal ulna.
CT scans with 3D reconstructions are highly recommended for post-traumatic cases, nonunions, or revision scenarios to evaluate volumetric bone loss and plan for potential structural allografts or custom implants. MRI is rarely indicated unless there is a specific concern for soft-tissue masses or occult triceps pathology.
Implant Selection Criteria
The choice between a linked (semiconstrained) and unlinked (unconstrained) prosthesis depends entirely on the integrity of the collateral ligaments and the surgeon's experience.
* Unlinked Implants: Require competent collateral ligaments, adequate bone stock (especially the condyles), and a functional radial head (or replacement). They are technically demanding but theoretically reduce stresses at the bone-cement interface.
* Linked (Semiconstrained) Implants: The workhorse of modern TEA. They are indicated when ligaments are incompetent, bone loss is severe (e.g., acute trauma, nonunions), or severe deformity exists. The "sloppy hinge" mechanism is forgiving and provides immediate stability.
Anesthesia and Patient Positioning
Regional anesthesia (supraclavicular or infraclavicular block) combined with general anesthesia is preferred to optimize postoperative pain control and facilitate early rehabilitation.
The patient is typically placed in the lateral decubitus position with the operative arm draped over a padded L-bar or Mayo stand post, allowing 120 degrees of unobstructed flexion. Alternatively, a supine position with the arm brought across the chest can be utilized, though this requires an assistant to hold the limb and can complicate fluoroscopic imaging. A sterile tourniquet is applied high on the brachium to ensure a bloodless field, inflated to 250 mm Hg after exsanguination.

Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of elbow arthroplasty requires meticulous soft-tissue handling and precise osseous preparation. Deviations from established techniques significantly increase the risk of ulnar neuropathy, triceps avulsion, and implant malalignment.
1. Incision and Ulnar Nerve Management
A straight posterior longitudinal incision is utilized, measuring approximately 15 cm. The incision is deliberately curved slightly lateral to the tip of the olecranon to avoid placing the surgical scar directly over the bony prominence, which can lead to painful bursitis or wound breakdown upon resting the elbow.

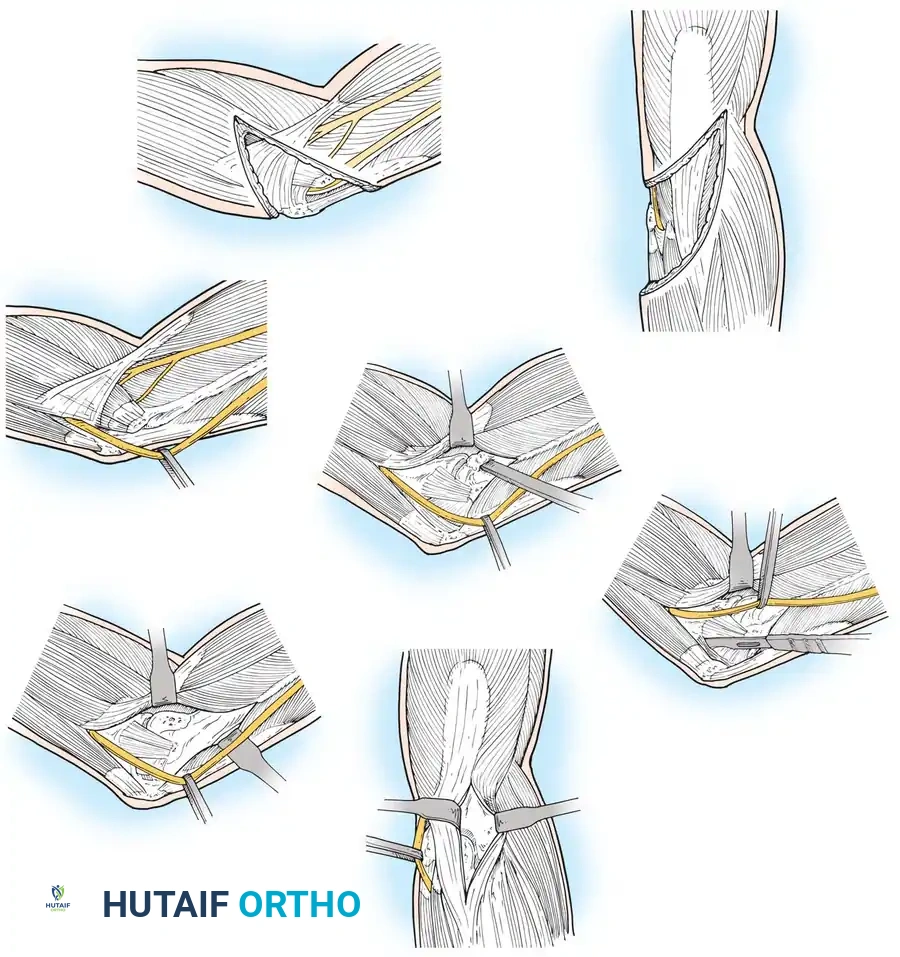
The ulnar nerve must be definitively identified proximally at the medial intermuscular septum. It is carefully mobilized distally through the cubital tunnel, releasing the arcade of Struthers, the Osborne fascia, and the flexor carpi ulnaris (FCU) aponeurosis. Routine anterior transposition (subcutaneous or submuscular) of the ulnar nerve is performed by most surgeons to prevent postoperative tension neuropathy and to keep the nerve away from the cement mantle and retractors during the procedure.
2. Management of the Extensor Mechanism
Accessing the joint requires addressing the triceps tendon. Several options exist, each with specific indications and morbidity profiles:
- Triceps-Reflecting (Bryan-Morrey Approach): The triceps is reflected from medial to lateral in continuity with the anconeus and the periosteum of the proximal ulna. This provides unparalleled exposure and allows for robust repair, making it the gold standard for linked TEA.
- Triceps-Splitting: The triceps is split longitudinally in the midline. While it preserves the medial and lateral insertions, exposure to the radiocapitellar joint is limited.
- Triceps-Sparing (Triceps-On): Used primarily for unconstrained resurfacing or trauma where the epicondyles are fractured. Windows are created medially and laterally to the triceps, preserving the extensor attachment entirely. This allows immediate active postoperative extension but is technically demanding.
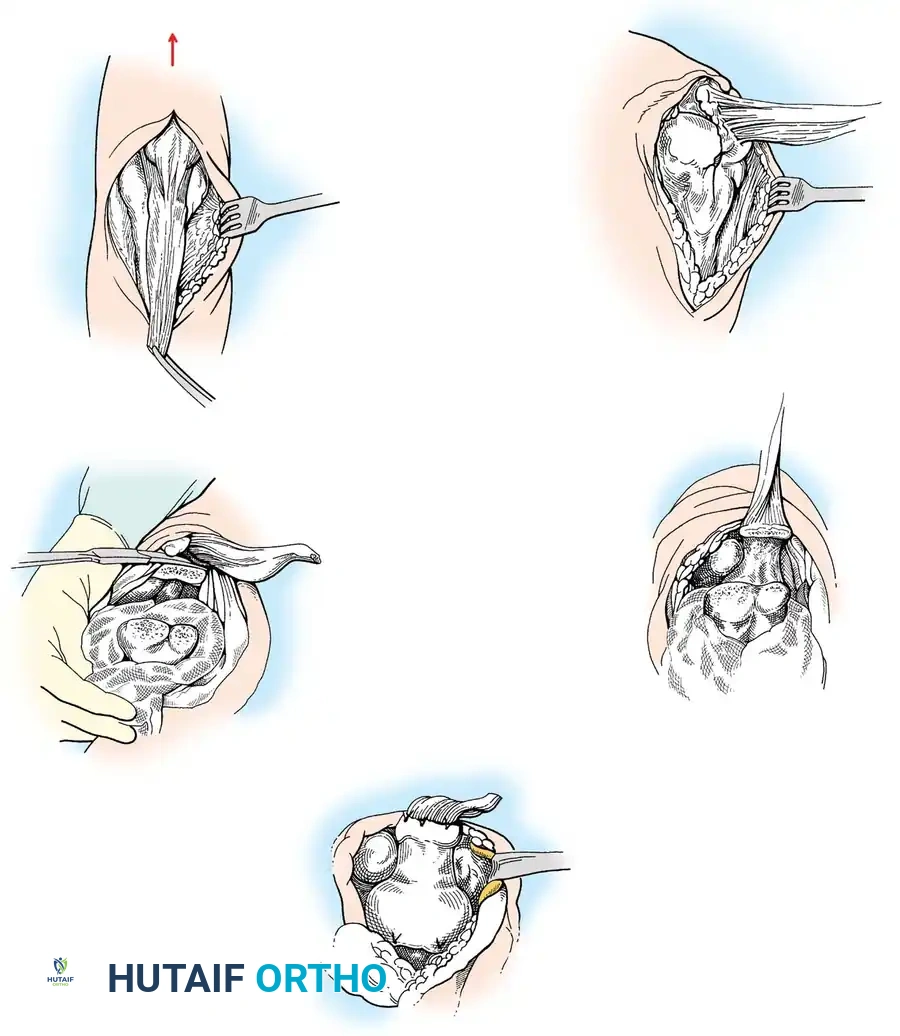
3. Joint Exposure and Osseous Preparation
Once the extensor mechanism is mobilized, the collateral ligaments are released (or preserved, depending on implant constraint), and the joint is dislocated by hyperflexing the elbow. The tip of the olecranon is often excised to improve exposure to the medullary canal of the ulna.
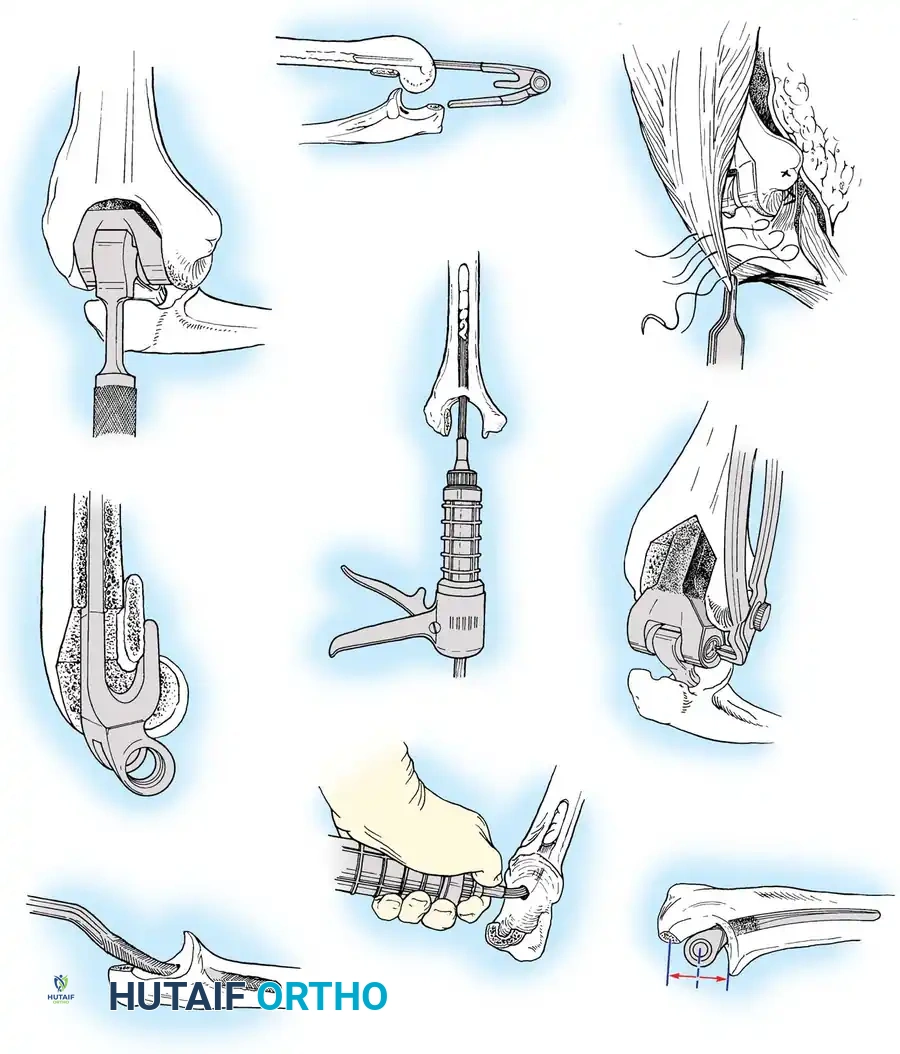
Humeral Preparation:
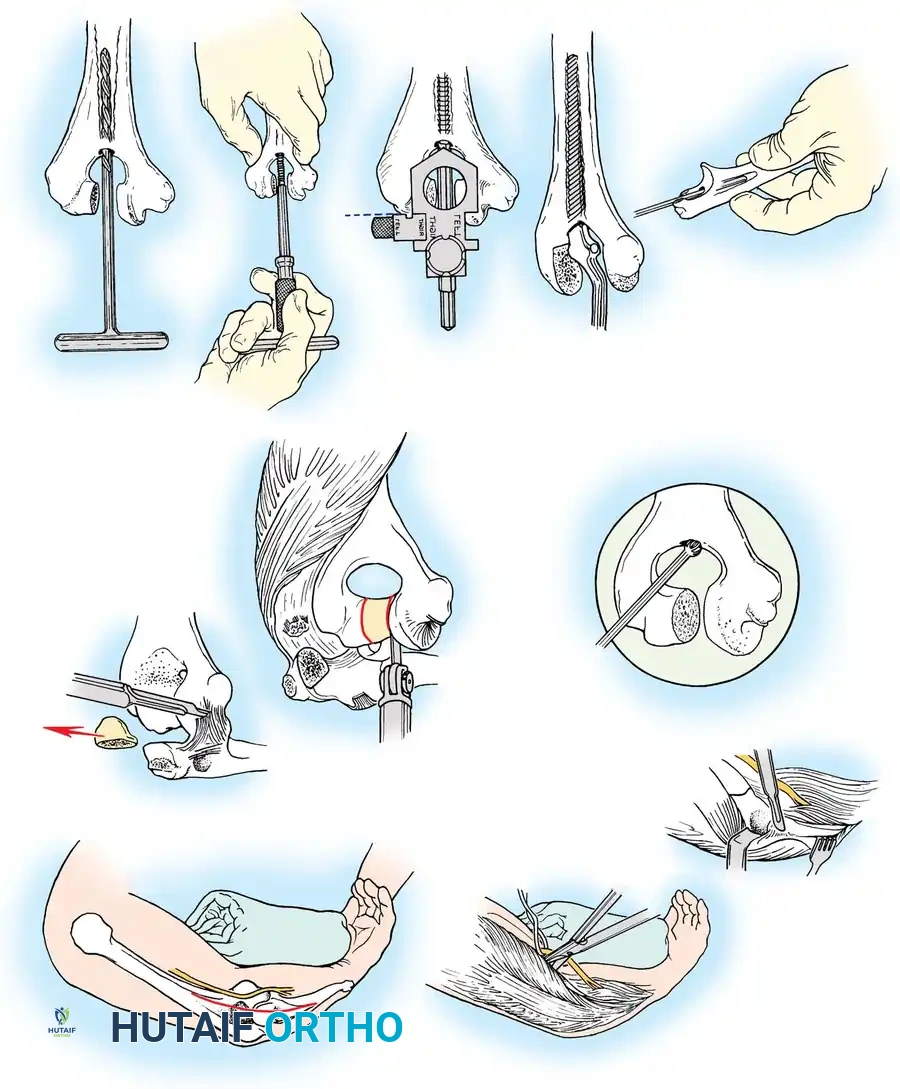
The humeral canal is accessed via the olecranon fossa. A high-speed burr is used to open the roof of the fossa. A pilot hole is created, and the canal is sequentially reamed and broached. It is critical to reference the posterior cortex of the distal humerus to recreate the normal anterior bow; failing to do so will result in anterior cortical perforation. A yoke or cutting block is utilized to resect the trochlea and capitellum, preserving the epicondyles if possible to retain soft-tissue attachments.
Ulnar Preparation:
The ulnar canal is accessed at the footprint of the excised olecranon tip. The ulnar canal has a complex, variable lateral and posterior bow. Sequential broaching must be performed with extreme care, often utilizing fluoroscopy, to avoid cortical perforation or blowout of the proximal ulna.
4. Trialing, Cementing Technique, and Implant Insertion
Trial components are inserted to assess the axis of rotation, tracking, and soft-tissue tension. In a linked prosthesis, the components are coupled, and the elbow is taken through a full range of motion. The joint should easily reach full extension and at least 130 degrees of flexion without excessive tension.
Modern TEA relies heavily on third-generation cementing techniques. The canals are pulsed-lavaged and dried with epinephrine-soaked sponges. Cement restrictors are placed distally in both the humerus and ulna. PMMA is injected in a retrograde fashion using a long-nozzle cement gun.
The ulnar component is typically inserted first, followed rapidly by the humeral component. The components are linked using the specific locking pin and bushing mechanism of the chosen system (e.g., the Coonrad-Morrey locking pin). Excess cement is meticulously removed before it cures, paying special attention to the anterior capsule and the ulnar nerve bed.

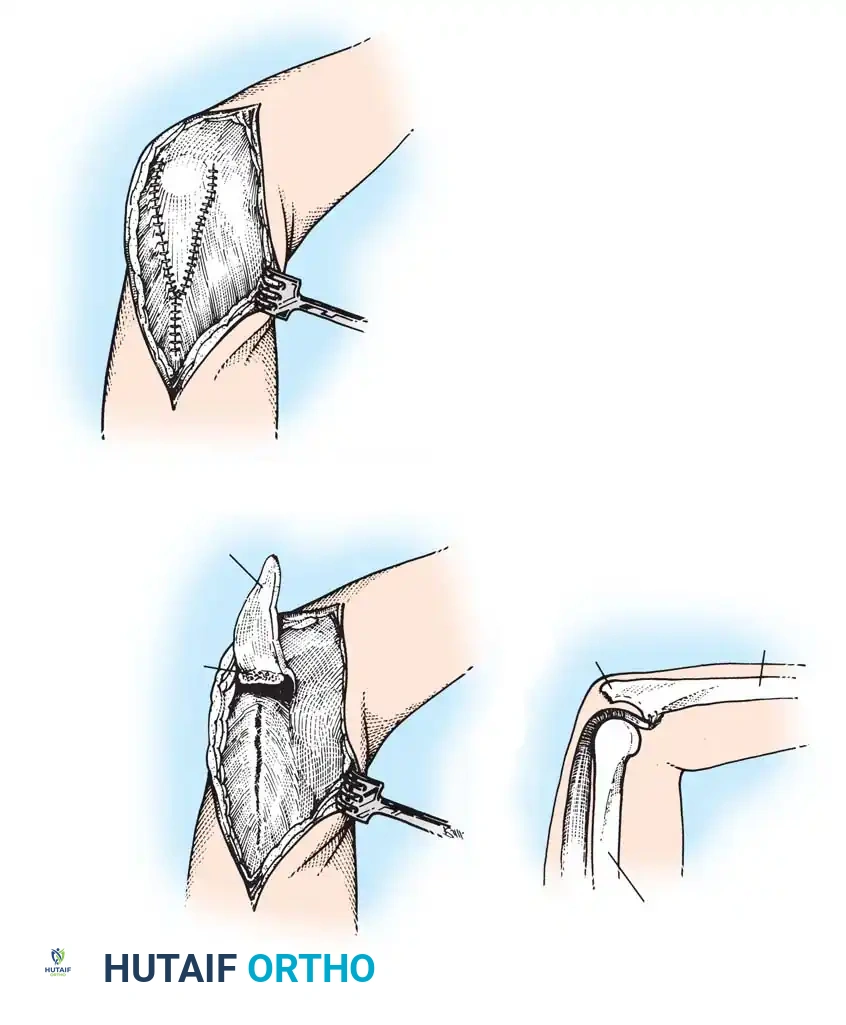
The triceps is then repaired through drill holes in the proximal ulna using heavy non-absorbable sutures (e.g., #2 or #5 FiberWire) in a Krackow fashion. The wound is closed in layers over a suction drain.

Complications, Incidence Rates, and Salvage Management
Total elbow arthroplasty carries a significantly higher complication rate than hip or knee arthroplasty, with overall complication rates historically ranging from 15% to 25%. The superficial nature of the joint, the complex biomechanics, and the poor bone stock of the typical patient cohort all contribute to this elevated risk.
Aseptic Loosening and Osteolysis
Aseptic loosening is the most common long-term complication, particularly of the humeral component. The "sloppy hinge" design has drastically reduced early loosening, but long-term cyclical loading inevitably leads to polyethylene wear at the bushing. The resulting particulate debris incites a macrophage-mediated osteolytic response, leading to massive bone loss and implant subsidence. Revision requires extensive structural allografting (e.g., strut grafts) or the use of custom, long-stemmed revision components.

Periprosthetic Joint Infection (PJI)
The thin soft-tissue envelope of the elbow makes it highly susceptible to infection, with primary TEA infection rates ranging from 2% to 5%, and up to 10% in revision settings. Staphylococcus aureus and Staphylococcus epidermidis are the most common pathogens. Acute infections (<4 weeks) may be managed with irrigation, debridement, and polyethylene exchange (DAIR). Chronic infections mandate a two-stage revision protocol: implant removal, placement of an antibiotic-impregnated PMMA spacer, 6 weeks of intravenous antibiotics, and eventual reimplantation.
Triceps Insufficiency and Instability
Failure of the triceps repair is a devastating complication, leading to profound weakness in extension and inability to perform activities of daily living against gravity. Incidence ranges from 1% to 4%. Repairing a chronic triceps avulsion is notoriously difficult and often requires augmentation with Achilles tendon allograft or anconeus muscle flaps.
Instability is primarily a complication of
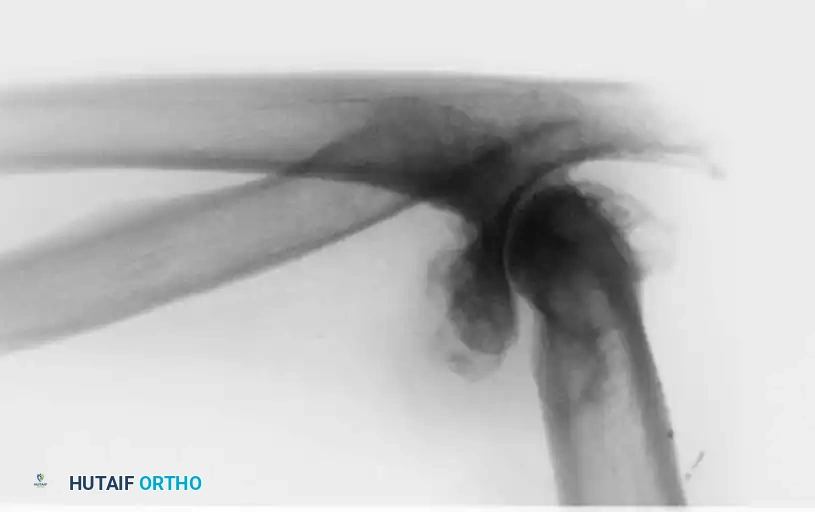
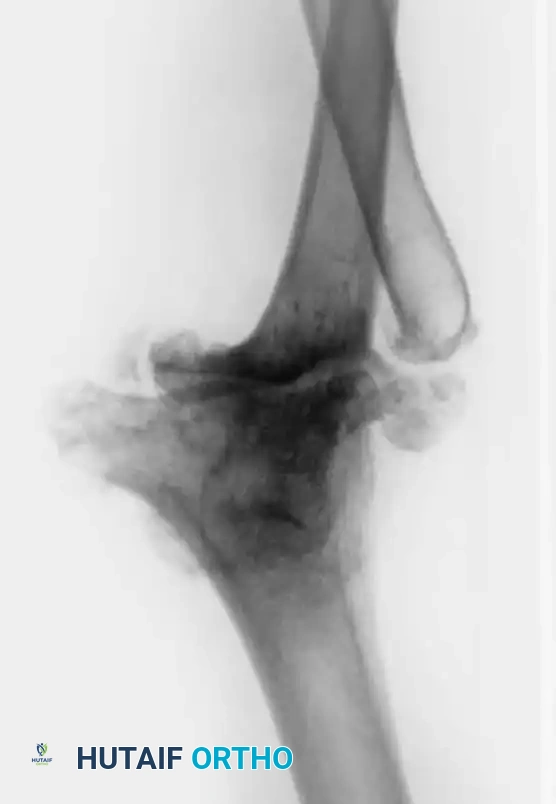
Clinical & Radiographic Imaging Archive