Comprehensive Management of Elbow Instability and Ulnar Collateral Ligament Reconstruction
Key Takeaway
The management of elbow instability requires a nuanced understanding of joint biomechanics and ligamentous anatomy. While stable acute dislocations often respond to early functional rehabilitation, chronic attritional injuries—particularly ulnar collateral ligament insufficiency in overhead athletes—frequently necessitate surgical reconstruction. This guide details evidence-based nonoperative protocols, arthroscopic evaluation techniques, and advanced surgical interventions, including the classic Jobe technique and the modern docking procedure for UCL reconstruction.
Comprehensive Introduction and Patho-Epidemiology
The elbow is a highly constrained, remarkably complex hinge joint that relies on a delicate, synergistic interplay of osseous congruity and capsuloligamentous integrity to maintain stability across a wide arc of motion. The primary static stabilizers are the geometrically congruent ulnohumeral articulation, the anterior bundle of the medial ulnar collateral ligament (UCL), and the lateral collateral ligament (LCL) complex, specifically the lateral ulnar collateral ligament (LUCL). Disruption of these critical structures, whether through high-energy acute traumatic dislocation or chronic, attritional microtraumatic attenuation in overhead athletes, leads to profound functional impairment, debilitating pain, and progressive articular degeneration. The patho-epidemiology of elbow instability is broadly bifurcated into these two distinct clinical entities: acute traumatic instability and chronic valgus overload.
Acute elbow dislocations represent the second most common major joint dislocation in adults, trailing only the glenohumeral joint. The mechanism of injury typically involves a fall on an outstretched hand (FOOSH), generating a combination of axial loading, external rotation, and valgus stress. This predictably results in a sequence of soft tissue failure that begins laterally and progresses medially, a cascade famously described by O’Driscoll as the "circle of Horii." Stage 1 involves disruption of the LUCL, leading to posterolateral rotatory instability (PLRI). Stage 2 involves anterior and posterior capsular tearing. Stage 3 involves complete disruption of the medial UCL, resulting in frank posterior or posterolateral dislocation. Understanding this predictable pattern of failure is paramount when formulating both nonoperative and operative management algorithms, as the lateral side is almost universally compromised in acute dislocations and must be the primary focus of reconstructive efforts if surgical stabilization is warranted.
Conversely, chronic elbow instability is overwhelmingly a pathology of the medial compartment, specifically targeting the UCL in the overhead throwing athlete. The epidemiology of UCL insufficiency has undergone a dramatic evolution over the past three decades. Originally considered a career-ending injury exclusive to elite professional baseball pitchers, the incidence of UCL reconstruction (colloquially known as "Tommy John" surgery) has surged exponentially across all levels of play, particularly among high school and collegiate athletes. This alarming demographic shift is driven by the year-round specialization in overhead sports, increased pitch velocities, and inadequate rest periods. The pathophysiology is characterized by repetitive, supraphysiologic valgus stress applied to the medial elbow during the late cocking and early acceleration phases of throwing.
These repetitive microtraumas exceed the ultimate tensile strength of the UCL, leading to microscopic tissue failure, interstitial tearing, and eventual macroscopic elongation or rupture. This attritional cascade is frequently accompanied by secondary adaptive changes, including valgus extension overload (VEO) syndrome. In VEO, the attenuation of the medial restraints allows for excessive valgus laxity, which in turn causes abnormal compressive forces laterally at the radiocapitellar joint and pathologic shear forces posteriorly as the olecranon forcefully abuts against the medial wall of the olecranon fossa. This repetitive impingement generates posteromedial osteophytes, loose bodies, and fixed flexion contractures, creating a complex constellation of intra-articular pathology that must be meticulously addressed during surgical intervention to ensure a successful return to sport.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the osseous and ligamentous anatomy of the elbow is the absolute prerequisite for diagnosing instability patterns and executing anatomically precise reconstructive procedures. The elbow joint is composed of three distinct articulations: the ulnohumeral joint, the radiocapitellar joint, and the proximal radioulnar joint. The ulnohumeral joint is a highly congruent ginglymus (hinge) joint that provides the primary osseous stability to the elbow, particularly at the extremes of flexion and extension. The radiocapitellar joint, while primarily facilitating forearm rotation, acts as a crucial secondary stabilizer against valgus stress, particularly when the medial ligamentous structures are compromised. The radial head absorbs approximately 30% of the valgus load in a competent elbow, but this demand increases dramatically in the setting of UCL insufficiency.
The medial ulnar collateral ligament (UCL) complex is the primary static restraint to valgus stress. It is composed of three distinct components: the anterior bundle, the posterior bundle, and the transverse ligament (Cooper’s ligament). The anterior bundle is the most biomechanically critical structure. It originates from the anteroinferior aspect of the medial epicondyle, posterior to the axis of rotation, and inserts onto the sublime tubercle of the proximal ulna. The anterior bundle is further subdivided into anterior and posterior bands. The anterior band is taut in extension and serves as the primary restraint to valgus stress up to 90 degrees of flexion, while the posterior band becomes taut in deeper flexion (beyond 90 degrees). This reciprocal tensioning ensures consistent medial stability throughout the functional arc of motion. The posterior bundle of the UCL originates from the posterior aspect of the medial epicondyle and inserts onto the medial margin of the semilunar notch, forming the floor of the cubital tunnel; it acts as a secondary restraint to valgus stress at maximum flexion. The transverse ligament spans the medial olecranon to the coronoid process and contributes negligible stability, as it originates and inserts on the same bone.
On the lateral side, the lateral collateral ligament (LCL) complex is the primary restraint to varus and external rotatory stress. It comprises the radial collateral ligament (RCL), the lateral ulnar collateral ligament (LUCL), the annular ligament, and the accessory collateral ligament. The LUCL is the most critical component for preventing posterolateral rotatory instability (PLRI). It originates from the lateral epicondyle, blends with the fibers of the annular ligament, and traverses posteroinferiorly to insert on the supinator crest of the proximal ulna. The LUCL acts as a hammock, supporting the radial head and preventing it from subluxating posteriorly relative to the capitellum during supination and axial loading. The RCL originates from the lateral epicondyle and inserts into the annular ligament, stabilizing the radial head while permitting rotation.
The dynamic stabilizers of the elbow play an equally vital role in maintaining joint congruity, particularly during the extreme force generation of the throwing motion. The flexor-pronator mass, originating from the medial epicondyle, provides dynamic valgus stability. Specifically, the flexor carpi ulnaris (FCU) and flexor digitorum superficialis (FDS) overlie the UCL and contract eccentrically to absorb valgus torque during the acceleration phase of throwing. Biomechanical studies have demonstrated that the valgus torque generated during a professional fastball pitch (approximately 64 Nm) exceeds the ultimate failure strength of the native UCL (approximately 34 Nm). Therefore, the integrity and synchronized firing of the dynamic flexor-pronator musculature are absolutely essential to prevent catastrophic ligamentous failure. Similarly, the common extensor origin and the anconeus provide dynamic lateral stability, while the triceps and biceps compress the ulnohumeral joint, enhancing osseous congruity across the arc of motion.
Exhaustive Indications and Contraindications
The decision-making process for the management of elbow instability requires a nuanced understanding of the patient's functional demands, chronicity of the injury, and the specific anatomic structures involved. A rigorous conservative trial is almost universally indicated as the first line of management, particularly for acute simple dislocations and first-time episodes of medial elbow pain in athletes. Operative intervention is reserved for specific, well-defined clinical scenarios where nonoperative modalities have failed or where the anatomic disruption precludes functional recovery.
For acute simple elbow dislocations, the primary indication for surgical intervention is a joint that remains subluxated or grossly unstable in a functional arc of motion (typically requiring more than 45 degrees of flexion to maintain reduction) despite appropriate closed reduction and splinting. Additionally, if the patient experiences recurrent instability in a well-fitted hinged brace, surgical stabilization of the lateral collateral ligament complex, and potentially the medial side, is warranted. In the chronic setting, the indications for UCL reconstruction are highly specific. The classic candidate is an elite overhead throwing athlete who has sustained an acute, complete rupture of the UCL or who suffers from chronic, attritional medial elbow pain that prevents competitive throwing and has proven refractory to a minimum of 3 to 6 months of strictly supervised, progressive rehabilitation.
Contraindications to surgical reconstruction must be carefully evaluated to prevent devastating postoperative complications and functional deterioration. Absolute contraindications include active intra-articular or periarticular infection, medically unstable patients who cannot tolerate general or regional anesthesia, and profound noncompliance. Relative contraindications require careful surgical judgment. For instance, a patient with a chronic UCL tear who does not participate in overhead sports or heavy manual labor can typically be managed nonoperatively with excellent functional outcomes, making reconstruction an unnecessary risk.
| Category | Indications for Surgical Intervention | Contraindications to Surgical Intervention |
|---|---|---|
| Acute Instability | Irreducible simple dislocation | Stable reduction through functional arc of motion |
| Recurrent instability despite rigid bracing | Polytrauma precluding immediate upper extremity surgery | |
| Persistent subluxation on post-reduction radiographs | Severe soft tissue compromise/blistering (delay surgery) | |
| Associated displaced fractures (coronoid, radial head) | Patient noncompliance with postoperative immobilization | |
| Chronic Instability | Elite throwing athlete with acute complete UCL rupture | Non-throwing athlete with asymptomatic laxity |
| Failure of 3-6 months of conservative rehab (UCL) | Advanced osteoarthritis with global joint stiffness | |
| Symptomatic PLRI affecting activities of daily living | Active regional or systemic infection | |
| Valgus extension overload with mechanical locking | Inadequate bone stock for tunnel creation (relative) |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the cornerstone of successful elbow ligamentous reconstruction. The clinical examination must be exhaustive, focusing on differentiating true capsuloligamentous instability from secondary intra-articular pathology such as radiocapitellar chondromalacia, posteromedial impingement, or ulnar neuritis. For medial instability, the moving valgus stress test and the milking maneuver are highly sensitive and specific. For lateral instability, the lateral pivot-shift test of O'Driscoll, typically performed with the patient supine and the arm overhead, is the pathognomonic clinical sign of LUCL incompetence, though it is often difficult to elicit in the awake patient due to muscular guarding.
Imaging protocols must be standardized to accurately delineate the bony and soft tissue architecture. Standard anteroposterior (AP), lateral, and oblique radiographs are mandatory to assess for subtle fractures, loose bodies, and osteophyte formation. Gravity valgus stress radiographs can quantify the degree of medial opening compared to the contralateral elbow. Magnetic Resonance Imaging (MRI), particularly MR arthrography (MRA) with intra-articular gadolinium, is the gold standard for evaluating the integrity of the UCL and LCL complexes. The "T-sign," characterized by contrast leakage deep to the distal insertion of the UCL on the sublime tubercle, is highly indicative of a high-grade partial or complete undersurface tear.

Graft selection is a critical component of preoperative planning. The palmaris longus (PL) autograft remains the undisputed gold standard for UCL reconstruction due to its ideal biomechanical properties, appropriate diameter, and minimal donor site morbidity. However, the surgeon must be acutely aware that the PL is congenitally absent in approximately 15% to 20% of the general population. Preoperative clinical assessment of the PL (asking the patient to oppose the thumb and small finger while flexing the wrist) is mandatory. In cases of PL absence, the gracilis tendon autograft is the preferred primary alternative, offering excellent tensile strength, though its larger diameter may require careful sizing of the bony tunnels. Plantaris tendon or allograft options (such as semitendinosus) are reserved for revision scenarios or multi-ligamentous reconstructions.
Patient positioning and operating room setup must be optimized for both arthroscopic and open phases of the procedure. The patient is typically positioned supine on the operating table. For the arthroscopic evaluation, the arm is often suspended using a sterile traction setup or positioned over a padded arm board. A non-sterile tourniquet is applied high on the brachium. Prior to prepping and draping, a rigorous Examination Under Anesthesia (EUA) is performed. The elimination of muscular guarding allows the surgeon to definitively quantify the degree of valgus, varus, and rotatory instability, comparing the operative limb to the contralateral side. If diagnostic arthroscopy is planned to address concomitant intra-articular pathology (e.g., loose body removal, posteromedial osteophyte resection), it is performed prior to the open reconstruction.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of a Ulnar Collateral Ligament (UCL) reconstruction demands unparalleled precision, profound anatomic knowledge, and meticulous tissue handling. While numerous techniques have been described since Frank Jobe's revolutionary initial report in 1986, the modern evolution of the procedure centers on minimizing morbidity to the flexor-pronator mass and optimizing graft fixation biomechanics. The "Docking Procedure" and the muscle-splitting approach have largely supplanted the classic Jobe technique, offering superior clinical outcomes and accelerated rehabilitation timelines.
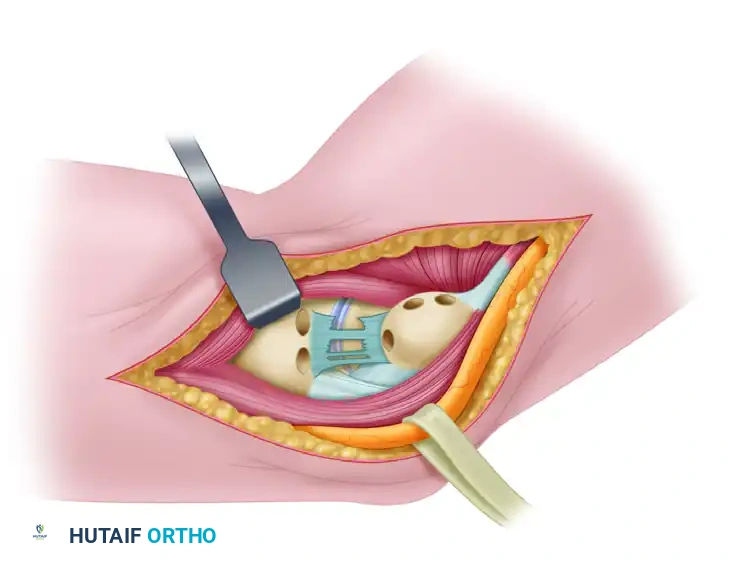
The surgical approach begins with a 5 to 7 cm longitudinal incision centered over the medial epicondyle, extending distally towards the sublime tubercle of the ulna. Subcutaneous dissection is performed meticulously to identify and protect the branches of the medial antebrachial cutaneous nerve (MABC). Iatrogenic injury to the MABC is a frequent source of debilitating postoperative neuroma and must be avoided at all costs. The deep fascia overlying the flexor-pronator mass is incised. In the modern muscle-splitting approach, rather than detaching the flexor-pronator origin from the epicondyle, a longitudinal split is created in the interval between the two heads of the flexor carpi ulnaris (FCU) or directly through the substance of the FCU, utilizing the natural fascial planes. Blunt retraction exposes the underlying native, attenuated UCL.
Management of the ulnar nerve is a critical decision point. In the original Jobe technique, obligatory submuscular transposition of the ulnar nerve was performed. However, contemporary practice advocates for in situ decompression or subcutaneous transposition only if the patient presents with preoperative ulnar neuritis or if the nerve subluxates dynamically during the procedure. Leaving the nerve in situ significantly reduces the risk of iatrogenic devascularization and postoperative neuropathy. If the nerve is left in situ, it is carefully protected with a retractor during tunnel preparation. The native UCL is longitudinally incised, exposing the medial joint space. An inspection of the articular surface is performed, and the sublime tubercle is cleared of soft tissue to prepare for ulnar tunnel creation.
Ulnar tunnel preparation requires precise trajectory to avoid cortical blowout and ensure anatomic graft placement. Two convergent drill holes (typically 3.2 mm) are created in the sublime tubercle, separated by a 1 cm bone bridge. The tunnels must be positioned exactly at the anatomic insertion of the anterior bundle of the UCL to ensure isometricity. A curved curette or specialized chamfering tool is used to connect the tunnels, creating a smooth, U-shaped intraosseous pathway. A passing suture is shuttled through the ulnar tunnel to facilitate subsequent graft passage.
Humeral tunnel preparation in the Docking Procedure represents a significant biomechanical advancement over the classic figure-of-eight technique. A single, closed-ended longitudinal socket (typically 4.0 to 4.5 mm in diameter, depending on graft size) is drilled into the anterior half of the medial epicondyle, at the exact anatomic origin of the native UCL. Two smaller exit punctures (1.5 mm) are drilled diverging from the apex of the main socket, exiting the posterior cortex of the medial epicondyle. The harvested palmaris longus graft is prepared on the back table with Krackow locking sutures at both ends. The graft is passed through the ulnar tunnel, and the two free limbs are brought proximally. The limbs are passed into the humeral socket, and the suture tails are shuttled through the small posterior exit holes. The elbow is positioned in supination and varus, and flexed to approximately 30 to 45 degrees to establish the appropriate tension. The graft is "docked" into the humeral tunnel, and the sutures are tied securely over the posterior bony bridge of the epicondyle. The native UCL is then imbricated and repaired over the graft to provide secondary vascularity and mechanical reinforcement.
Complications, Incidence Rates, and Salvage Management
Despite the high success rates associated with modern UCL reconstruction, the procedure is not without significant risks. Complications can profoundly impact the athlete's ability to return to sport and may necessitate complex salvage procedures. A thorough understanding of these potential pitfalls is essential for the operating surgeon to implement preventative strategies and manage adverse outcomes effectively.
Ulnar neuropathy remains the most frequent complication following UCL reconstruction, with reported incidence rates ranging from 5% to 15%, depending on the technique utilized. The etiology is multifactorial, including intraoperative traction neuropraxia, iatrogenic compression from fascial slings during transposition, perineural hematoma, or devascularization of the nerve. Symptoms typically manifest as paresthesias in the ring and small fingers, intrinsic muscle weakness, or a positive Tinel's sign at the cubital tunnel. While many cases are transient and resolve with conservative management (gabapentinoids, NSAIDs, observation), refractory cases lasting beyond 3 to 6 months may require surgical exploration, neurolysis, and formal transposition. The shift towards in situ nerve management in the Docking procedure has significantly reduced the incidence of this complication.
Graft failure or persistent instability is a catastrophic complication, occurring in approximately 2% to 5% of cases. Failure can result from technical errors (non-anatomic tunnel placement, inadequate graft tensioning, cortical blowout), biological failures (poor graft incorporation, infection), or premature return to high-velocity throwing before adequate ligamentization has occurred. If a patient presents with recurrent medial pain and a positive moving valgus stress test postoperatively, MRI is indicated to assess graft integrity. Salvage management for a failed UCL reconstruction is technically demanding. Revision surgery typically requires the use of a larger, more robust graft, such as a gracilis or semitendinosus autograft, or an allograft. The surgeon must carefully assess the existing bone tunnels; if they are excessively widened or malpositioned, bone grafting and staged reconstruction may be necessary to ensure rigid fixation.
| Complication | Estimated Incidence | Preventative Strategy | Salvage Management |
|---|---|---|---|
| Ulnar Neuropathy | 5% - 15% | Avoid obligatory transposition; meticulous hemostasis; limit traction | Gabapentinoids; surgical neurolysis; formal anterior transposition |
| Graft Failure/Laxity | 2% - 5% | Anatomic tunnel placement; strict adherence to rehab protocol | Revision reconstruction (Gracilis/Allograft); staged bone grafting |
| Medial Epicondyle Fx | < 1% | Avoid multiple large humeral tunnels (use Docking technique) | Open Reduction Internal Fixation (ORIF); cast immobilization |
| Heterotopic Ossification | 2% - 4% | Meticulous soft tissue handling; copious irrigation | Indomethacin; radiation therapy; delayed surgical excision |
| MABC Neuroma | 1% - 3% | Careful subcutaneous dissection; identify and retract nerve | Corticosteroid injection; surgical excision and burying of nerve stump |
| Infection | < 1% | Strict sterile technique; preoperative prophylactic antibiotics | Irrigation and debridement; targeted IV antibiotic therapy |
Phased Post-Operative Rehabilitation Protocols
The surgical reconstruction of the ulnar collateral ligament provides only the static mechanical foundation for stability; the ultimate functional success of the procedure is inextricably linked to the patient's strict adherence to a highly structured, phased rehabilitation protocol. The rehabilitation paradigm must balance the competing demands of protecting the healing graft from premature valgus stress while simultaneously preventing the rapid onset of debilitating arthrofibrosis, to which the elbow joint is uniquely susceptible. The protocol is typically divided into four distinct phases, progressing from immediate postoperative protection to a highly sport-specific return-to-throwing program.
Phase I: Immediate Postoperative Protection (Weeks 0-3)
The primary objectives of Phase I are to protect the healing graft, minimize inflammation, and initiate early, safe range of motion. Immediately postoperatively, the elbow is immobilized in a posterior splint at 90 degrees of flexion with the forearm in neutral rotation for 7 to 10 days. This allows the acute inflammatory phase to subside and the surgical incisions to heal. At the first postoperative visit, the splint is transitioned to a hinged elbow brace, initially locked from 30 to 90 degrees. Submaximal, pain-free isometric exercises for the biceps, triceps, and shoulder girdle are initiated. Crucially, gripping exercises and active wrist flexion/extension are encouraged to promote venous return and prevent distal edema, but resisted wrist flexion and pronation are strictly avoided to prevent dynamic stress on the flexor-pronator origin and the underlying graft.
Phase II: Intermediate Range of Motion and Strengthening (Weeks 4-8)
As the graft begins the early stages of ligamentization, the focus shifts to restoring full, symmetric range of motion and initiating isotonic strengthening. The hinged brace is gradually unlocked, typically advancing 10 to 15 degrees of extension and flexion per week, with the goal of achieving full ROM by week 6. Once full motion is achieved, the brace is discontinued. Isotonic strengthening of the entire upper extremity is initiated, emphasizing the flexor-pronator mass, which serves as the critical dynamic stabilizer of the medial elbow. Equally important is the initiation of a comprehensive kinetic chain program. Rehabilitation must aggressively target core stability, lower extremity power, and scapular kinematics. Scapular dyskinesia is a frequent concomitant finding in overhead athletes and, if left unaddressed, will result in altered throwing mechanics and recurrent excessive valgus stress on the newly reconstructed elbow.
Phase III: Advanced Strengthening and Plyometrics (Weeks 9-13)
Phase III bridges the gap between basic strength and explosive, sport-specific power generation. The athlete progresses to advanced, eccentric strengthening of the rotator cuff and periscapular musculature. Plyometric exercises are introduced to train the neuromuscular system to absorb and generate force rapidly. This typically begins with two-handed plyometric chest passes using a lightweight medicine ball, progressing to two-handed overhead throws, and eventually to one-handed plyometric throws against a trampoline. The athlete must demonstrate pain-free, symmetric strength and flawless kinetic chain mechanics before being cleared to progress to the final phase.
Phase IV: Interval Throwing and Return to Sport (Weeks 14+)
The initiation of an interval throwing program (ITP) marks the final and most critical phase of rehabilitation. The ITP is a highly structured, progressive program that gradually increases throwing distance, volume, and intensity. It typically begins with 45-foot flat-ground throws, emphasizing proper mechanics and a smooth, effortless delivery. The athlete progresses through 60-foot, 90-foot, and 120-foot stages, strictly monitoring for any return of medial elbow pain. Once the flat-ground program is completed successfully, the pitcher transitions to throwing off the mound, initially throwing exclusively fastballs at 50% effort. Breaking pitches (curveballs, sliders) are introduced last, as they generate the highest supraphysiologic valgus torques. Return to competitive, unrestricted pitching typically occurs between 12 and 18 months postoperatively, contingent upon the athlete demonstrating pain-free maximal velocity, flawless mechanics, and psychological readiness.
Summary of Landmark Literature and Clinical Guidelines
The evolution of elbow instability management and UCL reconstruction is deeply rooted in several landmark clinical and biomechanical studies that have shaped modern orthopedic practice. A comprehensive understanding of this literature is essential for the academic surgeon to practice evidence-based medicine and critically evaluate emerging surgical techniques.
The genesis of modern UCL reconstruction is universally attributed to Dr. Frank Jobe and his colleagues, who published their seminal paper in the Journal of Bone and Joint Surgery in 1986. Jobe detailed the surgical technique utilized on professional pitcher Tommy John in 1974, describing the detachment of the flexor-pronator mass, the creation of figure-of-eight bone tunnels, the use of a palmaris longus autograft, and the obligatory submuscular transposition of the ulnar nerve. While revolutionary, this initial technique was associated with a significant incidence of postoperative ulnar neuropathy (up to 20%) and prolonged rehabilitation timelines due to the extensive soft tissue dissection.
Recognizing the morbidity associated with the classic Jobe technique, Andrews and Timmerman (1995) and later Smith et al. (1996) published critical modifications. They advocated for a muscle-splitting approach through the FCU, preserving the dynamic stability of the flexor-pronator origin, and recommended leaving the ulnar nerve in situ unless clinically indicated. These modifications drastically reduced the incidence of neurologic complications and accelerated the return of functional strength.
The biomechanical superiority of modern fixation techniques was definitively established by Rohrbough et al. (2002) and subsequent researchers who popularized the "Docking Procedure." Biomechanical pull-out studies comparing the traditional figure-of-eight technique, the docking technique, and the use of bioabsorbable interference screws demonstrated that the docking technique provided superior ultimate failure strength and resistance to cyclic elongation. Furthermore, clinical outcome studies by Cain et al. (2010), who evaluated a massive cohort of 743 athletes undergoing UCL reconstruction using the docking technique, reported exceptional results: 83% of athletes returned to the same or a higher level of competition at less than one year postoperatively, cementing the muscle-splitting docking procedure as the contemporary gold standard.
Recent literature has focused on the role of internal brace augmentation. Studies by Dugas et al. (2016) introduced the concept of repairing the native UCL and augmenting it with a synthetic collagen-coated suture tape (internal brace) in select cases of acute, proximal, or distal avulsions with excellent tissue quality. While this technique offers the tantalizing prospect of a 6-month return to sport, long-term clinical outcome data and strict patient selection criteria are still being actively investigated, and formal autograft reconstruction remains the definitive standard of care for chronic, attritional ligamentous failure.
This academic synthesis is based on established protocols from Hutaifortho's Operative Orthopaedics and has been medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is designed to assist orthopedic residents, fellows, and practicing surgeons in surgical preparation and board reviews (AAOS, FRCS, Arab Board).

Chapter Index
- Comprehensive Introduction and Patho-Epidemiology
- Detailed Surgical Anatomy and Biomechanics
- Exhaustive Indications and Contraindications
- Pre-Operative Planning, Templating, and Patient Positioning
- Step-by-Step Surgical Approach and Fixation Technique
- Complications, Incidence Rates, and Salvage Management
- Phased Post-Operative Rehabilitation Protocols
- Summary of Landmark Literature and Clinical Guidelines
Back to Master Guide