Acute Triceps Tendon Ruptures: Epidemiology, Diagnosis, Surgical Anatomy & Biomechanics

Key Takeaway
A triceps tendon rupture is a significant elbow extensor injury, often presenting with a sudden 'pop,' acute pain, and a palpable defect. Common in active middle-aged males, it's diagnosed via history, physical exam (inability to extend elbow), and imaging. MRI is the gold standard, confirming diagnosis, assessing tear severity, and guiding treatment.
A 45-year-old male competitive powerlifter presents to the emergency department following an acute, sharp "pop" in his left elbow while attempting a heavy bench press. He is currently unable to actively extend his elbow against gravity. On examination, there is a palpable gap superior to the olecranon. Describe your immediate management and the critical decision-making process for this patient.
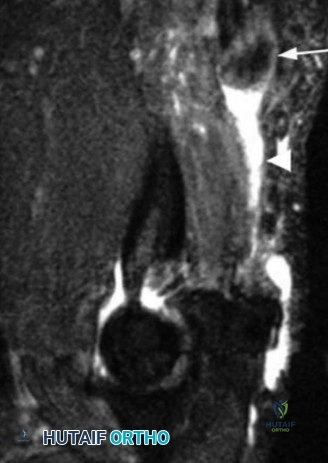
Candidate: I would clinically suspect a complete triceps tendon rupture. I would order AP and lateral radiographs to rule out an avulsion fracture of the olecranon (the "fleck sign"). Following this, I would order an MRI to confirm the rupture, quantify the degree of retraction, and assess the muscle quality. Given his age and high-demand occupation as a powerlifter, I would counsel him for early surgical repair to restore his extensor mechanism.
Failing to mention a thorough neurological examination, particularly regarding the radial nerve and its cutaneous branches. Also, failing to categorize the patient's functional demands, which is essential in justifying the urgency of surgical intervention in an acute setting.
I would approach this by first performing a rigorous physical exam to confirm the complete loss of the extensor mechanism and document baseline neurovascular status—specifically the radial nerve. Radiographically, I’d look for the "fleck sign." Given the patient’s high functional demand, my goal is anatomic repair within 2-3 weeks to avoid muscle contracture and atrophy. I would discuss the surgical options, including transosseous repair versus suture anchors, and explain the possibility of graft augmentation if intraoperative assessment reveals poor tissue quality or significant retraction.
You have decided to proceed with surgery. Describe your preferred patient positioning and the rationale behind your choice. Additionally, comment on the anatomical structures at risk during the approach.
Candidate: I prefer the prone position because it allows the arm to be free-draped, giving me full control over the elbow's range of motion to assess tension during the repair. I must be careful with padding the pressure points. The radial nerve is the main structure to protect; specifically, the posterior cutaneous nerve of the forearm is at high risk during the superficial approach.
Ignoring the "free-draping" aspect. If the arm is fixed on a board, you lose the ability to perform the intraoperative "tension test" at 30 degrees of flexion, which is vital for a successful repair. Also, forgetting to mention the specific sensory branch at risk (Posterior Cutaneous Nerve of the Forearm) makes the answer clinically incomplete.
I would utilize the prone position as it provides superior posterior access and allows for a free-draped arm. This is essential for placing the elbow in 20-30 degrees of flexion to tension the construct correctly. Anatomically, I would be meticulously careful to identify and protect the posterior cutaneous nerve of the forearm during subcutaneous dissection to avoid iatrogenic neuroma. Furthermore, I would remain cognizant of the radial nerve's proximity to the lateral intermuscular septum to avoid stretch or iatrogenic injury during deep exposure.
