Atypical Lateral Elbow Pain: ECRB Pathology, Radial Tunnel Syndrome & Diagnosis
Key Takeaway
Atypical lateral elbow pain extends beyond classic tennis elbow, often stemming from deep ECRB pathology, Radial Tunnel Syndrome (PIN compression), or subtle elbow instability (PLRI). Unlike typical lateral epicondylitis, these cases necessitate meticulous physical examination and advanced imaging for accurate diagnosis, guiding orthopedic surgeons toward effective, targeted interventions for persistent symptoms.
A 42-year-old tennis coach presents with chronic lateral elbow pain. He has failed 8 months of structured physiotherapy, activity modification, and two corticosteroid injections. He describes a deep, aching pain in the forearm distal to the epicondyle, which worsens with resisted supination. How would you approach your clinical examination to differentiate between classic lateral epicondylitis (LEC) and Radial Tunnel Syndrome (RTS)?
Candidate: I would start by palpating the point of maximal tenderness. For LEC, it's typically over the lateral epicondyle. For RTS, tenderness is 3-5 cm distal in the radial tunnel. I'd perform Cozen's and Mill's tests for LEC, and for RTS, I'd test resisted supination and resisted middle-finger extension. I’d also do a neurological exam to rule out motor weakness.
Failing to emphasize the distinction between "superficial" (epicondyle) vs. "deep" (radial tunnel) pain. Candidates often forget to mention that resisted middle-finger extension is a specific stress test for the ECRB origin's involvement in PIN compression.
I would perform a systematic provocation examination. For LEC: Palpation at the lateral epicondyle and positive Mill's/Cozen's tests. For RTS: Palpation at the radial tunnel (4-5 cm distal to the epicondyle), positive Maudsley’s test (resisted middle finger extension), and pain on resisted supination. Crucially, I would evaluate for concomitant PLRI using a pivot-shift maneuver, as instability often mimics or complicates these conditions.
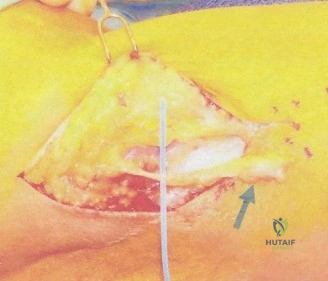
During your exploration for recalcitrant lateral elbow pain, you observe the relationship between the ECRB and the nerve structures. Please describe the five common potential sites of Posterior Interosseous Nerve (PIN) compression within the radial tunnel.
Candidate: The five sites are the fibrous bands anterior to the radial head, the Leash of Henry, the ECRB arcade, the Arcade of Frohse, and the distal edge of the supinator muscle.
Simply listing them without context. A senior candidate should note that the Arcade of Frohse is the most common site and that compression often occurs due to dynamic "wringing out" during pronation/supination.
The five anatomical points are: 1. Fibrous bands at the radiocapitellar joint, 2. The Leash of Henry (recurrent radial vessels), 3. The tendinous ECRB arcade, 4. The Arcade of Frohse (most common), and 5. The distal supinator edge. I would systematically release these during surgery, starting from proximal to distal, while maintaining vigilant protection of the motor branches.
You have diagnosed a patient with chronic deep ECRB tendinosis. They are scheduled for surgery. How do you technically differentiate the ECRL from the ECRB during your dissection, and what is the "gold standard" for managing the pathological tissue at the epicondyle?
Candidate: The ECRL originates more proximally on the supracondylar ridge, while the ECRB is deeper and originates from the lateral epicondyle. I would debride the diseased tissue and reattach the healthy tendon to the epicondyle.
Ignoring the "deep, articular-sided" nature of the pathology. Surgeons who only debride the superficial portion of the common extensor origin often fail to resolve symptoms because the primary tendinosis is deep to the superficial fibers.
I would emphasize that the ECRL is more superficial and lateral. To treat deep-seated pathology, I must reflect the superficial ECRL/EDC fascia to reveal the ECRB origin. The goal is complete excision of the angiofibroblastic (gray/friable) tissue from the articular-sided ECRB until healthy, bleeding tendon is reached. I would then perform decortication of the lateral epicondyle to create a bleeding bony bed, followed by secure reattachment of the healthy ECRB remnant using suture anchors or transosseous sutures.
