Medial Elbow Pain in Overhead Athletes: Comprehensive Diagnosis & Management
Key Takeaway
Medial elbow pain in overhead athletes stems from repetitive valgus stress during throwing, leading to UCL injuries, flexor-pronator tendinopathy, or ulnar nerve irritation. Accurate diagnosis involves understanding anatomy and biomechanics. Initial treatment often includes rest, activity modification, NSAIDs, and physical therapy, especially for skeletally immature athletes or mild cases.
You are assessing a 22-year-old collegiate baseball pitcher presenting with medial elbow pain. He reports a sensation of "popping" followed by immediate pain during a pitch in the late-cocking phase. On examination, he has tenderness over the sublime tubercle and a positive moving valgus stress test. What is your initial investigation of choice, and what do you expect to see?
Candidate: I would order an MRI arthrogram of the elbow to assess the integrity of the UCL. I would expect to see increased signal intensity at the sublime tubercle attachment site, possibly with extravasation of contrast, indicating a tear or significant laxity of the anterior bundle.
Candidates often jump straight to "MRI" without specifying the "arthrogram" component. In a high-demand athlete, a standard non-contrast MRI may miss partial-thickness tears on the deep surface of the ligament, which is the most critical area for surgical decision-making.
I would request an MRI arthrogram, as it is the gold standard for visualizing the UCL complex, specifically the anterior bundle. I am looking for high-signal intensity (T2 fat-sat) at the sublime tubercle attachment or within the ligament substance. I would also correlate this with plain radiographs—specifically stress views—to look for medial gapping compared to the contralateral elbow, which provides functional confirmation of UCL insufficiency.
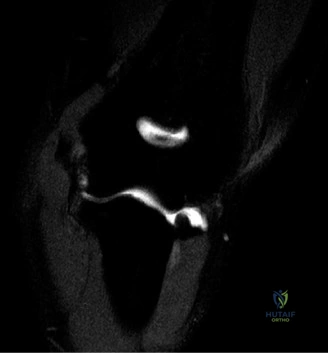
The patient has been diagnosed with a chronic UCL insufficiency and you are proceeding with surgical reconstruction. Referring to the image below, explain the key anatomical considerations for graft placement.

Candidate: The goal is to restore the isometric point of the anterior bundle. On the humerus, the graft should be placed near the center of rotation of the elbow, which is just anterior and distal to the medial epicondyle. On the ulna, the target is the sublime tubercle.
Failing to mention the "isometric point." A common mistake is placing the humeral tunnel too far posteriorly, which causes the graft to tighten during flexion and restrict range of motion (over-constraint).
The key is achieving isometry. The humeral tunnel should be placed at the anatomic origin on the medial epicondyle, specifically 2–3 mm proximal and posterior to the articular edge. If placed too far anteriorly or posteriorly, the graft will undergo length changes during flexion, leading to graft failure or joint stiffness. On the ulna, the target is the sublime tubercle, typically 18 mm distal to the coronoid tip and 4 mm distal to the joint line.
During your exposure for the UCL reconstruction, you encounter the ulnar nerve. How do you decide if a transposition is required?

Candidate: I would transpose if there is pre-existing cubital tunnel syndrome or if I think the nerve will be at risk during the drilling process for the tunnels. If it's stable, I might leave it in situ.
Being overly simplistic or suggesting routine transposition without mentioning the risks of transposition (e.g., devascularization of the nerve or iatrogenic nerve injury).
My decision is based on both clinical and intra-operative factors. If the patient has preoperative symptoms of cubital tunnel syndrome, or if the nerve shows instability (subluxation over the medial epicondyle during flexion) upon mobilization, I perform an anterior transposition. Prophylactic transposition is often favored in UCL reconstruction because the nerve is already mobilized during the exposure, and the graft tunnel creation risks traction injury or postoperative nerve tension. I ensure the nerve is protected from kinking and that the transposition bed is adequate.
Look at this post-operative radiograph. The patient has reached 6 months post-UCLR. What are you assessing in this view, and what is your return-to-sport strategy?

Candidate: I'm checking for hardware integrity and osseous integration. At 6 months, he should be in the late stages of rehab and starting a structured interval throwing program.
Forgetting to mention the "Interval Throwing Program" (ITP) and failing to define criteria for entry, such as symmetry in strength and absence of pain.
I am assessing the hardware position, confirming no displacement, and looking for evidence of tunnel widening or osseous integration. Return to sport is based on a milestone-based approach rather than time alone. At 6 months, the candidate must demonstrate full, painless ROM and symmetrical strength in the rotator cuff and scapular stabilizers. I then initiate a formalized Interval Throwing Program (ITP), beginning with flat-ground throwing at sub-maximal effort, monitoring closely for any medial-sided symptoms or mechanical breakdown before progressing to mound pitching.
