Elbow Capitellar Osteochondritis Dissecans: Epidemiology, Biomechanics & Comprehensive Management
Key Takeaway
Elbow osteochondritis dissecans (OCD) is necrosis of subchondral bone and cartilage, predominantly affecting the capitellum in adolescent overhead throwing athletes (ages 10-15). It's caused by repetitive valgus compressive forces during activities like pitching, leading to microtrauma and potential vascular insufficiency. Symptoms include pain and restricted motion, necessitating early diagnosis for optimal management.
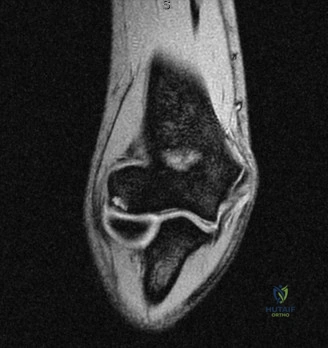
You are presented with a 14-year-old competitive baseball pitcher complaining of right-sided elbow pain for 6 months. He notes difficulty with terminal extension and occasional "catching" during throwing. The following radiograph is provided.
How do you approach the clinical assessment, and what is your immediate differential diagnosis?
Candidate: I would take a thorough history focusing on the duration and mechanical symptoms. On exam, I'd look for a flexion contracture, tenderness at the radiocapitellar joint, and pain on valgus stress testing. My primary differential is Osteochondritis Dissecans (OCD) of the capitellum vs. Panner’s disease, though his age makes OCD more likely. I would also consider lateral epicondylitis or osteochondral loose bodies.
Candidates often focus solely on the lesion and forget to mention the "throwing history." Failing to mention the age-based distinction between Panner's (typically <10) and OCD (10-15) is a major red flag for an examiner. Furthermore, missing the importance of checking the MCL for valgus instability (medial-sided stress affecting the lateral compartment) shows a lack of biomechanical understanding.
A high-scoring answer follows a structured approach: 1. History: Clarify the "throwing program," frequency, and mechanical symptoms (locking/catching). 2. Exam: Specifically check for a flexion contracture (a classic sign of intra-articular pathology), localized tenderness at the radiocapitellar joint, and MCL integrity. 3. Differential: Systematically exclude Panner’s (age/radiographic profile), stress-related injuries of the growth plate (Little League Elbow), and osteochondral loose bodies. 4. Synthesis: Emphasize that the patient's age and clinical presentation strongly suggest Capitellar OCD, and the next step is MRI to assess fragment stability.
The MRI confirms an unstable osteochondral fragment of the capitellum with a fluid signal at the interface and a small loose body. The patient is 14. What are your indications for surgical intervention versus continued observation?
Candidate: Surgery is indicated because the lesion is unstable and there is a loose body, which causes mechanical symptoms. Non-operative management is reserved for stable, asymptomatic lesions in younger patients. Since he is 14 and has mechanical symptoms, observation is inappropriate as it could lead to premature arthritis.
Failing to link the "unstable" nature of the lesion on MRI to the physical finding of mechanical symptoms. A weak answer fails to mention that skeletal maturity (or lack thereof) changes the prognosis and surgical options, such as the potential for microfracture vs. rigid fixation.
The candidate should categorize by Lesion Stability and Symptom Severity: 1. Surgical Indication: Unstable lesions (fluid rim on MRI), presence of loose bodies, failure of 3-6 months of conservative management, and the presence of persistent mechanical symptoms or loss of extension >15 degrees. 2. Goal of Surgery: To restore articular congruity and prevent secondary degenerative joint disease. 3. Mention the "Staging": Briefly reference that the Bednar or DIPA classification guides the decision, confirming that this patient falls into the "unstable/surgical" cohort.
During the arthroscopic evaluation of this 14-year-old, you confirm a 1.5 cm diameter osteochondral fragment that is stable but has clear evidence of subchondral bone necrosis. What is your surgical strategy?
Candidate: If the fragment is stable and the size is around 1.5 cm, I would perform a debridement of any unstable cartilage followed by marrow stimulation (microfracture) to encourage healing. If the fragment were large and loose, I would perform open reduction and internal fixation (ORIF) with headless screws.
Ignoring the "subchondral bone necrosis" aspect. Simply doing microfracture without ensuring the underlying bed is viable is a common failure. Also, failing to consider the patient's age and future sporting demands (e.g., if he's a elite pitcher, does he need a more robust restoration like OATS?) is a missed opportunity.
The gold standard answer provides a tiered approach: 1. Preparation: Meticulous debridement of the fibrous interface to reach healthy, bleeding subchondral bone. 2. Technique Selection: For a 1.5 cm stable lesion in a 14-year-old, if the fragment is salvageable, ORIF with countersunk headless compression screws is the gold standard for long-term articular preservation. 3. Alternative: If the fragment is non-viable or comminuted, suggest microfracture for smaller defects or OATS (osteochondral autograft transfer) if the defect is too large for biological healing, noting the risk of donor site morbidity.
