Comprehensive Surgical Management of Throwing Injuries of the Elbow
Key Takeaway
Throwing injuries of the elbow encompass a complex spectrum of pathology driven by repetitive valgus extension overload. This includes medial ulnar collateral ligament (UCL) insufficiency, lateral radiocapitellar compression, and posterior shear forces leading to posteromedial impingement. Accurate diagnosis relies on dynamic clinical examination and MR arthrography. Surgical management often involves arthroscopic debridement, osteophyte resection, or osteochondral grafting, followed by a meticulously phased rehabilitation protocol to restore the athlete's throwing mechanics and joint stability.
Comprehensive Introduction and Patho-Epidemiology
The overhead throwing motion represents one of the most violent and biomechanically demanding maneuvers in all of sports, placing extraordinary, repetitive stress on the osseous and ligamentous structures of the elbow joint. During the throwing cascade, the elbow is subjected to extreme valgus torque, rapid extension velocities, and immense compressive forces that frequently exceed the intrinsic tensile strength of the native tissues. The patho-epidemiology of throwing injuries is fundamentally rooted in a constellation of forces collectively known as Valgus Extension Overload (VEO). This biomechanical phenomenon results in a highly predictable triad of pathoanatomy: medial tension failure, lateral articular compression, and posterior osseous shear. As the prevalence of year-round overhead sports participation has exponentially increased, particularly among skeletally immature athletes, the incidence of throwing-related elbow pathology has reached epidemic proportions.
The epidemiology of these injuries spans a broad demographic, from the adolescent Little League pitcher to the elite professional quarterback, javelin thrower, or tennis player. However, the exact nature of the structural failure is heavily dependent on the skeletal maturity of the athlete. In the skeletally immature elbow, the weakest link in the kinetic chain is the physis or apophysis, leading to conditions such as medial epicondyle apophysitis (Little Leaguer's elbow), osteochondritis dissecans (OCD) of the capitellum, or physeal nonunion of the olecranon. Conversely, in the skeletally mature athlete, the physeal plates have fused, shifting the pathological burden to the ligamentous restraints and articular cartilage. This results in ulnar collateral ligament (UCL) attenuation or rupture, radiocapitellar chondromalacia, and the development of posteromedial olecranon osteophytes.
Understanding the epidemiology requires a deep appreciation of the kinetic chain. The elbow does not operate in isolation; it functions as a funnel for kinetic energy generated by the lower extremities, core, and shoulder girdle. Deficits in hip internal rotation, core stability, or scapular dyskinesia inevitably force the elbow to absorb compensatory loads. When the proximal kinetic chain fails to generate or transfer energy efficiently, the arm lags behind the torso during the late cocking phase, drastically increasing the valgus torque applied to the medial elbow. Consequently, any comprehensive surgical management strategy must be predicated on a holistic understanding of the athlete's throwing mechanics, ensuring that isolated surgical correction of elbow pathoanatomy is not subsequently undermined by unaddressed proximal kinetic chain deficits.
The classic pathoanatomical cascade described by Cain et al. remains the foundational framework for understanding throwing injuries. The repetitive medial tension leads to microtearing, mucoid degeneration, and eventual macroscopic failure of the anterior bundle of the UCL. Concurrently, the lateral radiocapitellar joint experiences severe compressive forces, predisposing the capitellum to osteochondral microtrauma and loose body formation. Finally, the rapid deceleration of the extending elbow violently wedges the olecranon tip into the posteromedial olecranon fossa, creating shear forces that generate posteromedial osteophytes and reactive chondromalacia. Loose bodies are a frequent concomitant finding across all compartments and may migrate, further complicating the clinical picture and necessitating meticulous surgical evaluation.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the surgical anatomy and biomechanics of the elbow is the absolute prerequisite for the successful operative management of throwing injuries. The stability of the elbow joint is governed by a highly integrated complex of static and dynamic restraints. On the medial side, the static stability is primarily provided by the ulnar collateral ligament (UCL) complex, which consists of three distinct bundles: the anterior, posterior, and transverse bundles. The anterior bundle of the medial ulnar collateral ligament (AMCL) is the most critical structure in the throwing athlete. It originates from the anteroinferior surface of the medial epicondyle—specifically, slightly posterior to the axis of rotation—and inserts onto the sublime tubercle of the proximal ulna. The AMCL is further subdivided into anterior and posterior bands. The anterior band is taut in extension and provides primary resistance to valgus stress up to 90 degrees of flexion, while the posterior band becomes the primary restraint at flexion angles greater than 90 degrees.
The lateral ligamentous complex, specifically the lateral ulnar collateral ligament (LUCL), is the primary restraint to posterolateral rotatory instability (PLRI). While less commonly injured by the primary throwing motion than the medial structures, the LUCL must be meticulously preserved during lateral surgical approaches or arthroscopic portal placement. The osseous anatomy of the radiocapitellar joint is equally critical; the convex capitellum articulates with the concave radial head, acting as a secondary bony buttress to valgus stress. During the throwing motion, up to 30% of the valgus load is transmitted as compressive force across the radiocapitellar articulation. In the posterior compartment, the olecranon process articulates with the olecranon fossa of the distal humerus. The posteromedial aspect of this articulation is particularly vulnerable to shear forces during the terminal extension phase of throwing, leading to the classic valgus extension overload syndrome.
The biomechanics of the overhead throw are classically divided into six distinct phases: wind-up, early cocking, late cocking, acceleration, deceleration, and follow-through. The late cocking and early acceleration phases are the most deleterious to the elbow. During late cocking, the shoulder is maximally externally rotated, and the elbow is flexed to approximately 90 to 100 degrees. As the torso rotates forward to initiate acceleration, the arm lags behind, generating a peak valgus torque that can exceed 64 Newton-meters (Nm). Cadaveric studies have demonstrated that the ultimate tensile failure load of the native UCL is approximately 34 Nm. This biomechanical paradox indicates that the dynamic stabilizers—specifically the flexor-pronator mass (flexor carpi ulnaris and flexor digitorum superficialis)—must fire forcefully to absorb the remaining stress and protect the UCL from catastrophic failure.
During the deceleration phase, the elbow extends at a staggering angular velocity, often exceeding 2,500 degrees per second. The eccentric contraction of the biceps brachii and brachialis is required to decelerate the extending forearm, while the triceps brachii fires to control the terminal extension. This rapid extension creates extreme posterior shear forces as the olecranon is driven into the posteromedial fossa. The repetitive nature of these extreme biomechanical forces leads to adaptive, yet ultimately pathological, changes. The anterior capsule may become attenuated, the flexor-pronator mass may develop chronic tendinosis, and the articular cartilage undergoes microstructural degradation. A comprehensive understanding of these phase-specific forces allows the orthopedic surgeon to accurately correlate the athlete's specific mechanical pain with the underlying structural pathology.
Exhaustive Indications and Contraindications
The decision to proceed with surgical intervention in the throwing athlete is highly nuanced and must be tailored to the patient's chronicity of symptoms, specific pathoanatomy, skeletal maturity, and future athletic aspirations. Surgical management is strictly indicated only after exhaustive conservative measures—including prolonged rest, structured physical therapy focusing on the kinetic chain, non-steroidal anti-inflammatory medications, and biomechanical throwing analysis—have failed to provide durable relief. The primary goal of surgery is to restore the anatomical stability and kinematic function of the elbow, allowing for a safe return to elite-level overhead activity.
Indications for surgical intervention vary significantly based on the anatomical compartment involved. For medial-sided pathology, formal UCL reconstruction (Tommy John surgery) is definitively indicated in the competitive throwing athlete with a documented full-thickness rupture of the AMCL, or in athletes with high-grade partial undersurface tears who have failed a minimum of three to six months of non-operative management (which may include biologic augmentation such as Platelet-Rich Plasma injections). For lateral-sided pathology, such as capitellar osteochondritis dissecans (OCD), surgical intervention is indicated for unstable lesions (Grade III or IV), detached loose bodies, or progressive capitellar flattening. Posterior compartment surgery is indicated for symptomatic posteromedial osteophytes causing mechanical impingement, fixed flexion contractures, or the presence of symptomatic loose bodies that restrict range of motion.
Contraindications to surgical management are equally critical to recognize to prevent disastrous postoperative outcomes. Absolute contraindications include active local or systemic infection, severe medical comorbidities precluding safe anesthesia, and the presence of complex regional pain syndrome (CRPS) in the affected extremity. Relative contraindications are more common and require meticulous clinical judgment. Operating on a partial UCL tear in a non-throwing athlete or a recreational athlete who can modify their activities is generally discouraged. Furthermore, performing an isolated posteromedial osteophyte resection in the presence of gross, unaddressed UCL insufficiency is a strict relative contraindication, as removing the posterior bony buttress will exponentially exacerbate the medial instability.
| Pathological Entity | Primary Surgical Indication | Conservative / Alternative Management | Strict Surgical Contraindications |
|---|---|---|---|
| UCL Insufficiency | Full-thickness rupture in an elite thrower; failed non-op partial tears. | Rest, kinetic chain rehab, PRP injections, bracing. | Non-overhead athlete; asymptomatic incidental MRI finding. |
| Posteromedial Impingement | Mechanical catching, fixed flexion contracture, failed 3-6 months rehab. | NSAIDs, intra-articular corticosteroid injection, rest. | Gross UCL instability (unless performed concomitantly with UCL reconstruction). |
| Capitellar OCD | Grade III/IV unstable lesions, loose bodies, mechanical locking. | Cessation of throwing, hinged bracing (for Grade I/II in immature athletes). | Asymptomatic stable lesions in skeletally immature patients. |
| Symptomatic Plica | Persistent catching/snapping failing conservative care; ruled out OCD. | Activity modification, NSAIDs, diagnostic/therapeutic injection. | Vague lateral pain without mechanical symptoms or MRI correlation. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful surgical outcomes in the management of throwing injuries. The clinical evaluation must be exhaustive, beginning with a detailed history of the athlete's throwing mechanics, pitch counts, velocity changes, and the exact phase of throwing that elicits pain. Physical examination must include the moving valgus stress test, the milking maneuver, and a rigorous assessment of the ulnar nerve for subluxation or signs of neuritis. Advanced imaging is strictly indicated when an overhead athlete presents with elbow pain refractory to conservative treatment. Standard radiographs (AP, lateral, oblique, and axial projections) are essential for evaluating osteophyte formation, loose bodies, and the status of the physes in young athletes.
Magnetic Resonance Imaging (MRI) without contrast is highly sensitive for detecting bone marrow edema, stress reactions, and gross ligamentous disruptions. However, Magnetic Resonance Arthrography (MRA), utilizing an intra-articular injection of a gadolinium contrast agent, remains the gold standard for fully evaluating partial, undersurface tears of the ulnar collateral ligament. The classic "T-sign" on MRA indicates contrast material leaking medial to the sublime tubercle, confirming an undersurface detachment of the AMCL. In cases of capitellar OCD, MRI is invaluable for assessing the stability of the subchondral bone plate and the viability of the surrounding cartilage, which directly dictates whether the surgeon will plan for microfracture, internal fixation, or an Osteochondral Autograft Transfer System (OATS) procedure.
Patient positioning in the operating room is dictated by the specific pathology being addressed and the surgeon's institutional preference. For isolated arthroscopic procedures (osteophyte excision, loose body removal, plica excision), the patient is typically placed in either the lateral decubitus position over a bolster or in the prone position. The lateral decubitus position, utilizing a dedicated arm holder, allows for excellent access to both the anterior and posterior compartments while allowing the elbow to hang freely at 90 degrees. A non-sterile tourniquet is placed high on the brachium. The prone position offers superior access to the posterior compartment and is highly favored when extensive posteromedial osteophyte resection is anticipated.
For procedures requiring open medial or lateral approaches, such as UCL reconstruction or open OATS procedures, the patient is positioned supine with the operative extremity resting on a radiolucent hand table. This allows for seamless integration of fluoroscopy, which is critical for confirming tunnel placement during ligament reconstruction or graft congruency during osteochondral transfer. Regardless of the position, meticulous padding of all bony prominences and strict attention to the contralateral extremity are mandatory. Fluid management during arthroscopy is paramount; a gravity or low-pressure mechanical pump system is utilized to prevent excessive fluid extravasation, which can lead to devastating compartment syndrome of the forearm.
Step-by-Step Surgical Approach and Fixation Technique
The surgical management of throwing injuries often requires a hybrid approach, combining advanced diagnostic and therapeutic arthroscopy with open reconstructive techniques. Diagnostic arthroscopy is the definitive initial step when structural pathology is suspected but not entirely elucidated by advanced imaging, or when concomitant intra-articular lesions must be addressed prior to extra-articular reconstruction. The procedure begins with the establishment of the proximal anteromedial portal, created under direct visualization via a spinal needle, to avoid iatrogenic injury to the medial antebrachial cutaneous nerve. The arthroscope is then introduced to visualize the anterior compartment, specifically focusing on the radiocapitellar and ulnohumeral articulations.
Dynamic Arthroscopic Stress Testing
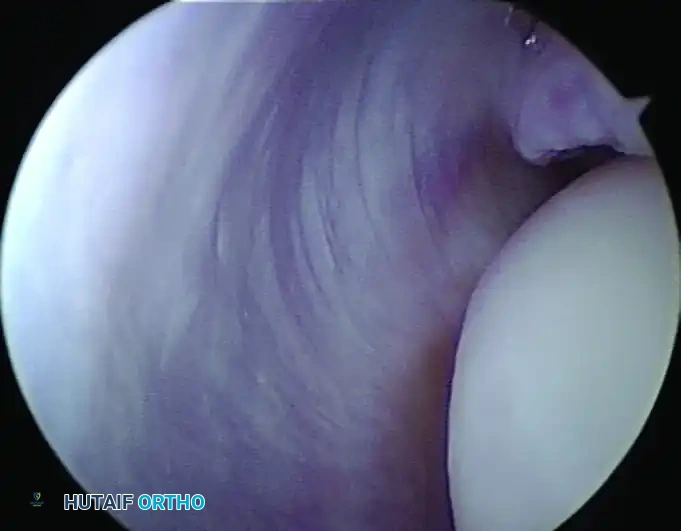
The functional integrity of the anterior bundle of the UCL can be meticulously evaluated during this diagnostic phase. The forearm is fully supinated, and the elbow is flexed to exactly 70 degrees to unlock the olecranon from its fossa, thereby isolating the AMCL. A controlled valgus stress is applied to the joint by the surgeon. Normally, the ulnohumeral joint opens less than 1 mm. An opening of more than 1 to 2 mm, according to the criteria established by Andrews and Baumgarten, indicates functional instability of the UCL.
Arthroscopic examination showing medial instability to stress examination at 70 degrees of flexion. Note the pathologic 2-mm opening between the coronoid and the trochlea, indicative of UCL incompetence.
It is critical to recognize the "undersurface tear pitfall." Incomplete undersurface tears of the UCL may not open to valgus stress during arthroscopy because the superficial fibers remain intact, masking the deep fiber failure. In these cases, localized ligamentous hemorrhage, capsular avulsion, or a positive "drive-through" sign between the coronoid and trochlea may be the only visual clues. If gross instability is confirmed, the surgeon must be prepared to transition to an open UCL reconstruction.
Posterior Impingement and the 3-Millimeter Rule
When addressing Valgus Extension Overload (VEO), the posterior compartment is accessed utilizing a posterolateral viewing portal and a direct posterior working portal. A thorough diagnostic sweep is performed to extract any elusive loose bodies hiding in the olecranon fossa. A motorized 4.0mm burr is then introduced to resect the impinging posteromedial osteophyte. Strict adherence to biomechanical limits during this resection is mandatory. Studies by Kamineni et al. have definitively shown that it is safe to remove the osteophyte and no more than 3 mm of native bone at the tip of the olecranon. More aggressive removal destroys the critical bony buttress that resists valgus stress in terminal extension, exponentially increasing stress transfer to the UCL and risking catastrophic iatrogenic instability.
Management of OCD and Plica Syndrome
For lateral-sided compression injuries, such as capitellar OCD, the surgical strategy is dictated by lesion grade. For contained Grade I or II lesions, arthroscopic debridement of the unstable cartilage is performed using a 3.0mm shaver, followed by microfracture of the sclerotic base using specialized arthroscopic awls to stimulate marrow-derived fibrocartilage healing. In cases of large, uncontained Grade III lesions, an open or mini-open Osteochondral Autograft Transfer System (OATS) is required. Cylindrical osteochondral plugs are harvested from the non-weight-bearing periphery of the ipsilateral knee (typically the lateral supracondylar ridge) and press-fit into the meticulously prepared capitellar defect, restoring the hyaline articular contour.
Posterolateral synovial plica syndrome, often presenting as a mechanical snapping during terminal extension, is addressed via the anterolateral and direct lateral portals. The hypertrophic, fibrotic radiocapitellar plica is identified as it impinges between the radial head and capitellum. Arthroscopic excision is performed using a radiofrequency wand or motorized shaver, ensuring complete resection of the fibrotic band while meticulously preserving the underlying lateral ulnar collateral ligament (LUCL) capsule to prevent iatrogenic posterolateral rotatory instability.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, the operative management of throwing injuries in the elbow carries a distinct profile of potential complications. The dense neurovascular anatomy, the propensity of the elbow capsule to develop arthrofibrosis, and the extreme biomechanical demands placed on the joint postoperatively all contribute to surgical risk. The most common and arguably most frustrating complication following surgical intervention—particularly open medial-sided procedures like UCL reconstruction—is postoperative ulnar neuropathy. Ulnar neuritis or frank neuropathy can result from excessive traction during exposure, compression from postoperative hematoma, or perineural fibrosis.
Iatrogenic instability is a devastating complication primarily associated with overzealous resection of the olecranon during the treatment of posterior impingement. As previously noted, violating the 3-millimeter rule compromises the osseous buttress, leading to immediate overload of the medial ligamentous structures. Arthrofibrosis, characterized by a profound loss of terminal extension and flexion, is a common sequela of extensive capsular work or prolonged postoperative immobilization. Infection, while relatively rare in elbow arthroscopy, can occur and requires aggressive, immediate management to prevent catastrophic chondrolysis. Graft failure or re-rupture following UCL reconstruction occurs in a small percentage of elite athletes, often due to premature return to throwing or technical errors such as non-isometric tunnel placement.
Salvage management requires a highly customized approach. Postoperative ulnar neuropathy that fails to resolve with conservative measures (gabapentinoids, bracing) may necessitate secondary surgery for formal ulnar nerve transposition (subcutaneous or submuscular). Iatrogenic instability resulting from olecranon over-resection is incredibly difficult to salvage; it often requires a formal UCL reconstruction to compensate for the lost bony restraint, and in severe cases, osteochondral grafting of the olecranon has been described, though outcomes are unpredictable. Recalcitrant arthrofibrosis is managed with aggressive, supervised physical therapy and dynamic splinting; if this fails after 6 months, an open or arthroscopic capsular release (capsulectomy) is indicated.
| Complication | Estimated Incidence | Primary Etiology / Risk Factor | Salvage / Management Strategy |
|---|---|---|---|
| Ulnar Neuropathy | 5% - 15% (UCL Recon) | Traction injury, hematoma, scar tethering. | Observation, gabapentin; secondary transposition if refractory > 3 months. |
| Arthrofibrosis | 5% - 10% | Prolonged immobilization, excessive capsular trauma. | Dynamic splinting; arthroscopic/open capsulectomy if no progress by 6 months. |
| Iatrogenic Instability | < 2% (VEO Surgery) | Resection of > 3mm of native olecranon tip. | Formal UCL reconstruction to restore medial restraint. |
| Graft Failure (UCL) | 2% - 5% | Non-isometric tunnels, premature return to throwing. | Revision UCL reconstruction (often utilizing different graft/technique). |
| Superficial/Deep Infection | < 1% | Poor sterile technique, compromised soft tissue envelope. | I&D, copious lavage, culture-directed IV antibiotics. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following surgical intervention for throwing injuries is just as critical as the surgical procedure itself. The elbow is notoriously unforgiving; it rapidly develops stiffness if immobilized too long, yet healing ligamentous or capsular tissues will stretch out and fail if subjected to premature stress. Therefore, rehabilitation must be meticulously phased, utilizing a criterion-based progression rather than a strictly time-based one. The following protocol outlines the comprehensive recovery strategy following arthroscopic intervention (debridement, osteophyte excision, plica removal). It is important to note that formal UCL reconstruction or large OATS procedures require significantly more conservative, extended timelines.
Phase I: Immediate Postoperative (Weeks 0-2)
The primary goals of Phase I are the protection of healing tissues, control of postoperative edema, and the prevention of distal atrophy. Immediately following surgery, a well-padded posterior cast or rigid soft splint is applied with the elbow positioned at 90 degrees of flexion and neutral rotation. This splint is worn continuously for the first 10 to 14 days to allow for acute soft tissue healing and to minimize hemarthrosis. During this period, active range of motion (ROM) of the wrist, hand, and shoulder is heavily encouraged to maintain distal perfusion, reduce edema, and preserve proximal muscle tone. Cryotherapy is utilized continuously.
Phase II: Intermediate ROM and Strengthening (Weeks 3-8)
At the beginning of Phase II, the rigid splint is discontinued, and a hinged elbow brace may be utilized depending on the extent of the procedure. Range-of-motion exercises for the elbow are formally initiated. The emphasis is immediately placed on restoring full terminal extension, which is often the most difficult arc of motion to regain following posterior compartment surgery or prolonged flexion splinting. Active-assisted and passive ROM exercises are performed multiple times daily. By week 6, patients should ideally achieve a functional arc of motion (0 to 130 degrees). Submaximal isometric strengthening of the biceps, triceps, and forearm flexor-pronator mass is initiated, gradually progressing to light isotonic resistance as tolerated.
Phase III: Advanced Strengthening and Kinetic Chain Integration (Weeks 9-16)
Phase III focuses on restoring symmetric strength, muscular endurance, and integrating the entire kinetic chain. Heavy emphasis is placed on scapular stabilization, core strengthening, and lower extremity power generation. The flexor-pronator mass is aggressively strengthened, as these muscles serve as the primary dynamic protectors of the medial elbow during the throwing motion. Plyometric exercises, such as two-handed chest passes and medicine ball throws, are introduced to prepare the upper extremity for the ballistic forces of throwing. The athlete must demonstrate full, painless ROM and symmetric strength before progressing to the next phase.
Phase IV: Return to Throwing Progression (Months 4-6+)
The final phase is the structured interval throwing program. Patients are allowed to begin this program only when they are completely asymptomatic during daily activities and high-level plyometrics. The program starts strictly with underhand tossing at short distances (30-45 feet) to reintroduce the arm to throwing mechanics without extreme valgus stress. By 4 to 5 months postoperatively, gentle overhand throwing is permitted, focusing entirely on proper mechanics rather than velocity. Pitchers will progress to throwing off flat ground before eventually moving to the mound. Full throwing from the mound at maximum velocity is typically permitted at 6 months for arthroscopic procedures (and 12-18 months for UCL reconstruction), provided the athlete has regained flawless kinetic chain mechanics and remains entirely pain-free.
Summary of Landmark Literature and Clinical Guidelines
The evolution of surgical management for throwing injuries of the elbow is deeply rooted in several landmark biomechanical and clinical studies. Frank Jobe’s original 1986 publication on the reconstruction of the ulnar collateral ligament using a free palmaris longus autograft revolutionized the treatment of the overhead athlete. Prior to this, a ruptured UCL was considered a career-ending injury. Jobe’s figure-of-eight technique laid the groundwork for modern variations, including the docking technique popularized by Altchek and the DANE TJ technique, which have further optimized graft tensioning and reduced the incidence of postoperative ulnar neuropathy by minimizing nerve handling.
The understanding of arthroscopic evaluation of the elbow was fundamentally advanced by Andrews and Baumgarten, who defined the criteria for arthroscopic valgus stress testing. Their observation that an opening of greater than 1 to 2 mm between the coronoid and trochlea under dynamic stress at 70 degrees of flexion signifies UCL incompetence remains the gold standard for intraoperative diagnosis. Furthermore, the concept of undersurface tears, extensively researched by Timmerman and Andrews, highlighted the limitations of standard MRI and the necessity of MRA or direct arthroscopic visualization to diagnose deep-fiber failure that leaves the superficial ligament intact.
The surgical management of Valgus Extension Overload (VEO) is governed by the critical biomechanical studies performed by Kamineni et al. Their landmark cadaveric research definitively established the "3-millimeter rule." They demonstrated that the olecranon tip provides a crucial osseous buttress against valgus stress during terminal extension. Resecting more than 3 mm of native bone significantly alters the joint kinematics, transferring intolerable loads to the AMCL and precipitating iatrogenic instability. This study serves as a universal clinical guideline, cautioning surgeons against aggressive posterior resections.
Finally, the overarching pathoanatomical framework of throwing injuries relies on the triad described by Cain et al. Their comprehensive description of medial tension, lateral compression, and posterior shear forces provides the theoretical basis for evaluating the entire joint rather than focusing on isolated lesions. Current clinical guidelines, including those endorsed by the American Orthopaedic Society for Sports Medicine (AOSSM), universally mandate that the surgical management of the throwing elbow must be coupled with an exhaustive evaluation of the athlete's kinetic chain, ensuring that proximal mechanical deficits are corrected to prevent recurrent elbow pathology.
